1 June 2016 - Case of the Week #390
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Ankur Sangoi, El Camino Hospital, California (USA) for contributing this case. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) If you are starting a new job or fellowship in June or July, please email us with your new email so you can continue to receive our newsletters.
(2) We recently posted new Product Questionnaires. These can help pathologists compare and contrast the various products and services offered by participating companies. Creative Diagnostics, Rowley Biochemical and Quidel Corporation have new questionnaires located under Diagnostic Testing Kits / Reagents, and Rowley Biochemical has a new questionnaire under Histology Products and Services.
(3) We have now posted versions of the Jobs, Fellowships by Specialty and State / Country, and Conferences pages as of April 1, 2016 and May 1, 2016.
Visit and follow our Blog to see recent updates to the website.
Case of the Week #390
Clinical history:
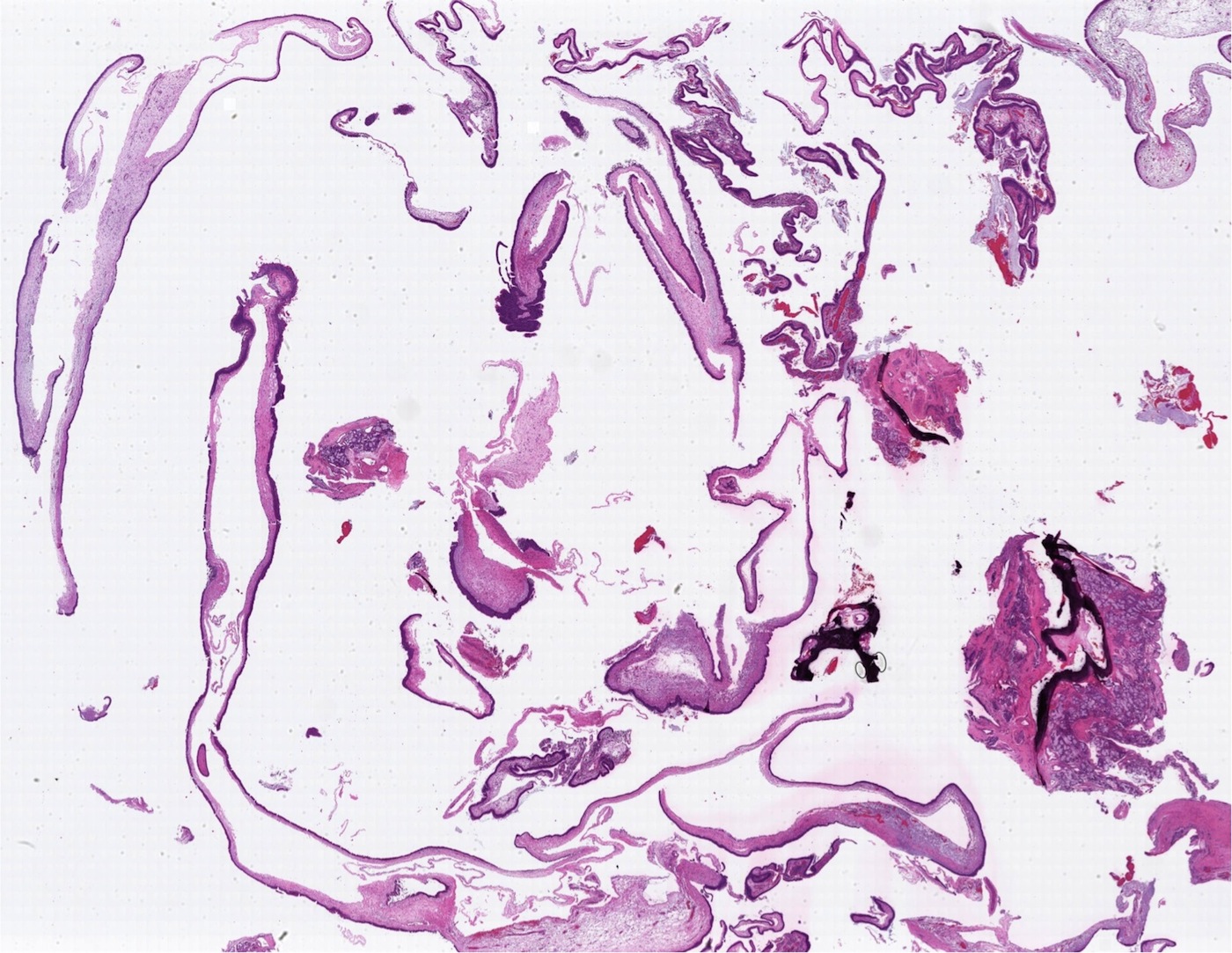
A 27 year old woman presented with a right nasal polyp, which was excised.
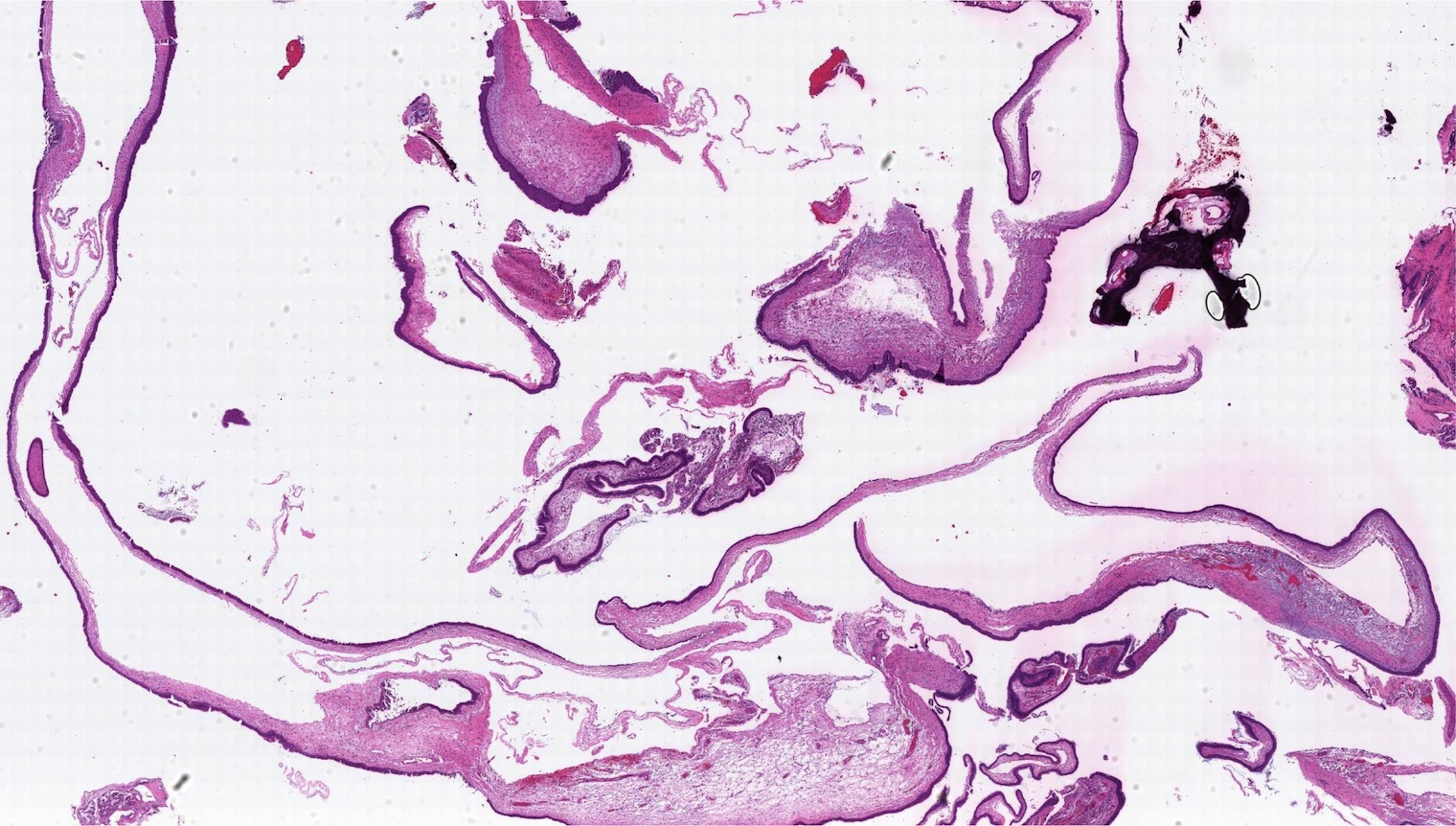
Micro images:

What is your diagnosis?
Diagnosis:
Antrochoanal polyp
Discussion:
Nasal polyps are non-neoplastic; their formation is associated with inflammation, allergy or mucoviscidosis. A choanal polyp arises from the paranasal sinuses, and these are subdivided based on location, with antrocholanal the most common (Rosai: Rosai and Ackerman's Surgical Pathology, 10th ed, 2011). Antrochoanal polyps represent 4-6% of all nasal polyps and occur most frequently in childhood. 90% are solitary and they usually arise from the wall of the maxillary antrum, extending through a large primary or secondary maxillary ostium into the nasal cavity. In this case, the ENT surgeon confirmed that the elongate polyp arose from the maxillary sinus and extended into the nasal cavity.
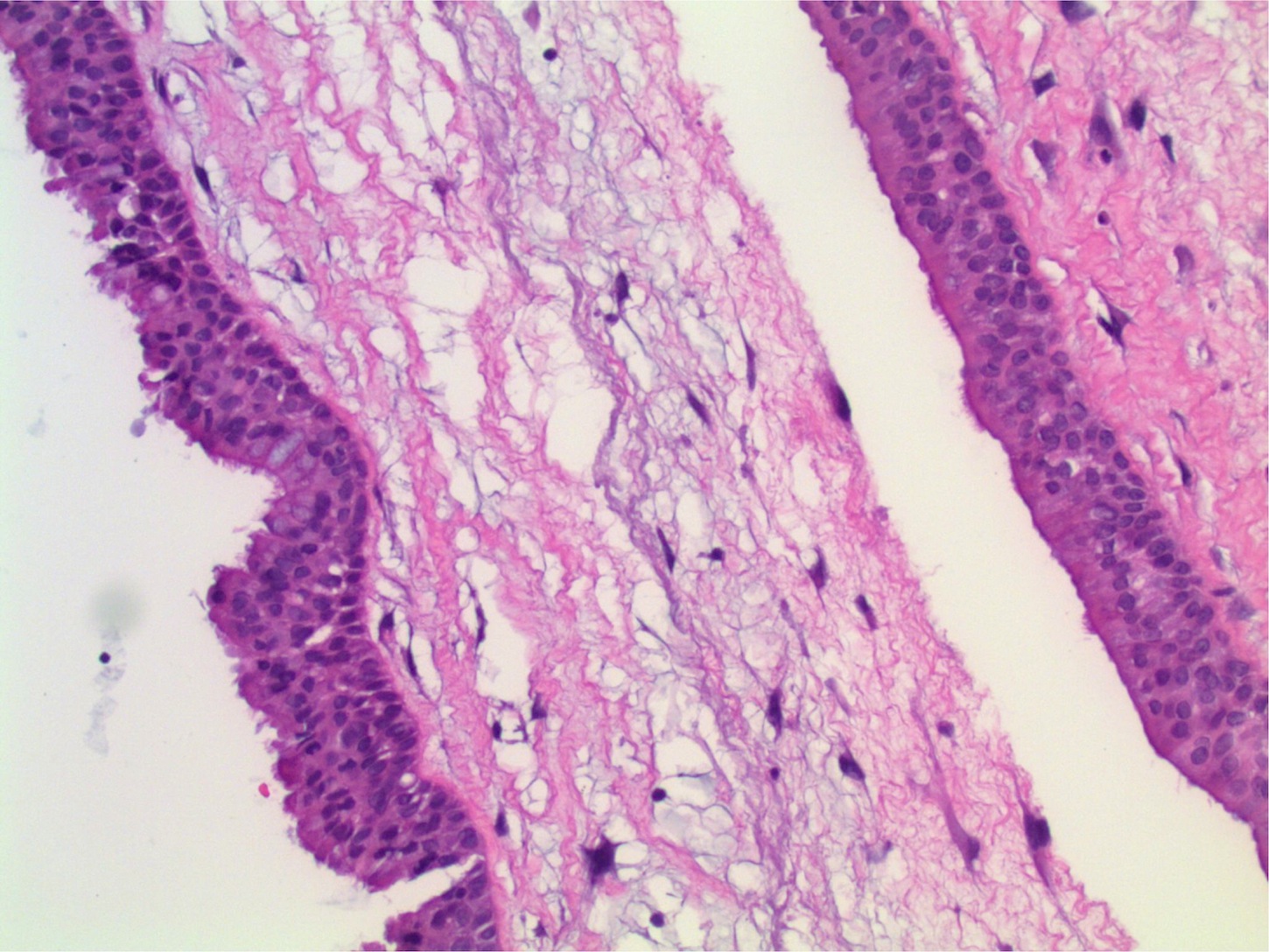
Grossly, there is a long narrow stalk with a firm, fibrous body. Histopathology is similar to an inflammatory polyp and shows surface respiratory mucosa with no significant cytologic atypia. Areas of squamous metaplasia may be seen. The stroma contains stellate cells which are reactive in nature. A prominent component of dilated vessels with thrombosis or infarct is often present. Prominent eosinophils are seen in only 20%, in contrast to inflammatory polyp, which usually contains more.
The primary differential diagnosis includes inflammatory / allergic polyp, which typically shows more eosinophils and more submucous glands (Acta Otolaryngol 1995;115:543). The prominent dilated vessels of the antrochoanal polyp can also be a helpful distinguishing feature.
Local recurrence is common following surgical removal, likely because of persistence of inciting pathogenetic factors (Rosai: Rosai and Ackerman's Surgical Pathology, 10th ed, 2011).
Discussion by: Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences (USA).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Ankur Sangoi, El Camino Hospital, California (USA) for contributing this case. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) If you are starting a new job or fellowship in June or July, please email us with your new email so you can continue to receive our newsletters.
(2) We recently posted new Product Questionnaires. These can help pathologists compare and contrast the various products and services offered by participating companies. Creative Diagnostics, Rowley Biochemical and Quidel Corporation have new questionnaires located under Diagnostic Testing Kits / Reagents, and Rowley Biochemical has a new questionnaire under Histology Products and Services.
(3) We have now posted versions of the Jobs, Fellowships by Specialty and State / Country, and Conferences pages as of April 1, 2016 and May 1, 2016.
Visit and follow our Blog to see recent updates to the website.
Case of the Week #390
Clinical history:
A 27 year old woman presented with a right nasal polyp, which was excised.
Micro images:
What is your diagnosis?
Diagnosis:
Antrochoanal polyp
Discussion:
Nasal polyps are non-neoplastic; their formation is associated with inflammation, allergy or mucoviscidosis. A choanal polyp arises from the paranasal sinuses, and these are subdivided based on location, with antrocholanal the most common (Rosai: Rosai and Ackerman's Surgical Pathology, 10th ed, 2011). Antrochoanal polyps represent 4-6% of all nasal polyps and occur most frequently in childhood. 90% are solitary and they usually arise from the wall of the maxillary antrum, extending through a large primary or secondary maxillary ostium into the nasal cavity. In this case, the ENT surgeon confirmed that the elongate polyp arose from the maxillary sinus and extended into the nasal cavity.
Grossly, there is a long narrow stalk with a firm, fibrous body. Histopathology is similar to an inflammatory polyp and shows surface respiratory mucosa with no significant cytologic atypia. Areas of squamous metaplasia may be seen. The stroma contains stellate cells which are reactive in nature. A prominent component of dilated vessels with thrombosis or infarct is often present. Prominent eosinophils are seen in only 20%, in contrast to inflammatory polyp, which usually contains more.
The primary differential diagnosis includes inflammatory / allergic polyp, which typically shows more eosinophils and more submucous glands (Acta Otolaryngol 1995;115:543). The prominent dilated vessels of the antrochoanal polyp can also be a helpful distinguishing feature.
Local recurrence is common following surgical removal, likely because of persistence of inciting pathogenetic factors (Rosai: Rosai and Ackerman's Surgical Pathology, 10th ed, 2011).
Discussion by: Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences (USA).