25 May 2016 - Case of the Week #389
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Leow Wei Qiang, Singapore General Hospital (Singapore) for contributing this case and discussion. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) If you are starting a new job or fellowship in June or July, please email us with your new email so you can continue to receive our newsletters.
(2) As of 18 May 2016, we have 5,267 followers on Twitter and 7,622 likes (business equivalent to "friends") on Facebook. Are you following PathologyOutlines.com on social media? If not, you may be missing out on quick access to updates, and occasional advertiser giveaways and specials, that are found on our Facebook and Twitter pages. Most recently, Mopec posted information about how to enter to win a free dissecting kit. Not only did someone win a dissecting kit, but Mopec reported an increase in followers across social channels and an increase in engagement and impressions. A win-win! For more information on posting on our Facebook and Twitter pages, contact us at (248) 646-0325 or pathoutads@gmail.com.
(3) We recently posted a new Management page article: Preparing for the Merit-Based Incentive Payment System by Alex Mitchell, Vachette Pathology. Keep your eyes open for other articles to be posted in upcoming weeks. We also recently posted information about new products being offered by Mopec and Milestone Medical. We post new information, as it becomes available, on our New Products and Services page.
Visit and follow our Blog to see recent updates to the website.
Case of the Week #389
Clinical history:
A 27 year old man with familial adenomatous polyposis (FAP), status post pan-proctocolectomy 10 years ago, underwent an elective gastroscopy. There were multiple polyps identified in the gastric fundus and body, which were biopsied.
Gross description:
The specimen consists of two pieces of tissue measuring 0.2 cm and 0.5 cm.
Micro images:

What is your diagnosis?
Diagnosis:
Familial adenomatous polyposis (FAP) associated fundic gland polyps with low grade dysplasia
Discussion:
The biopsies were described as follows:
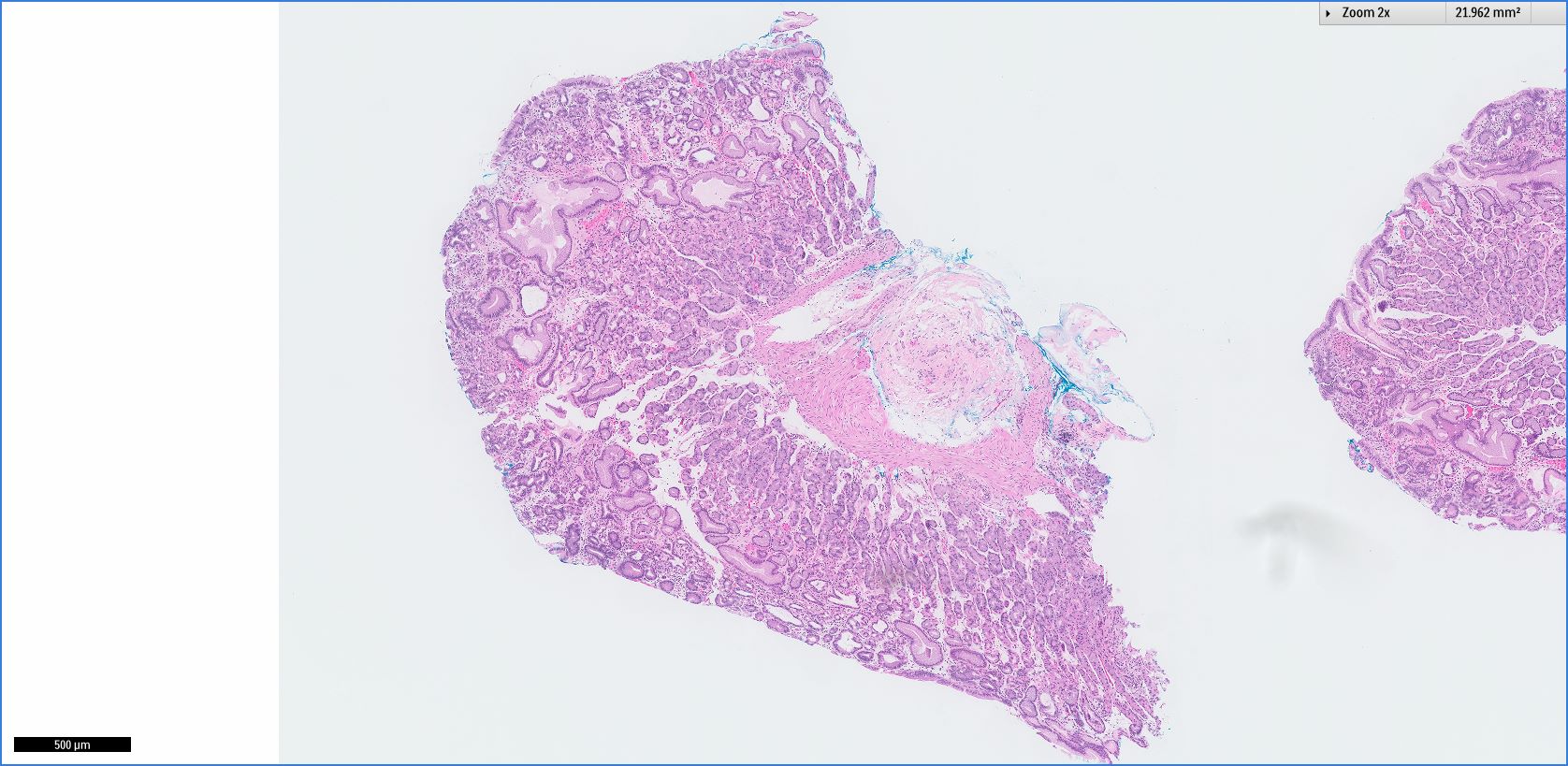
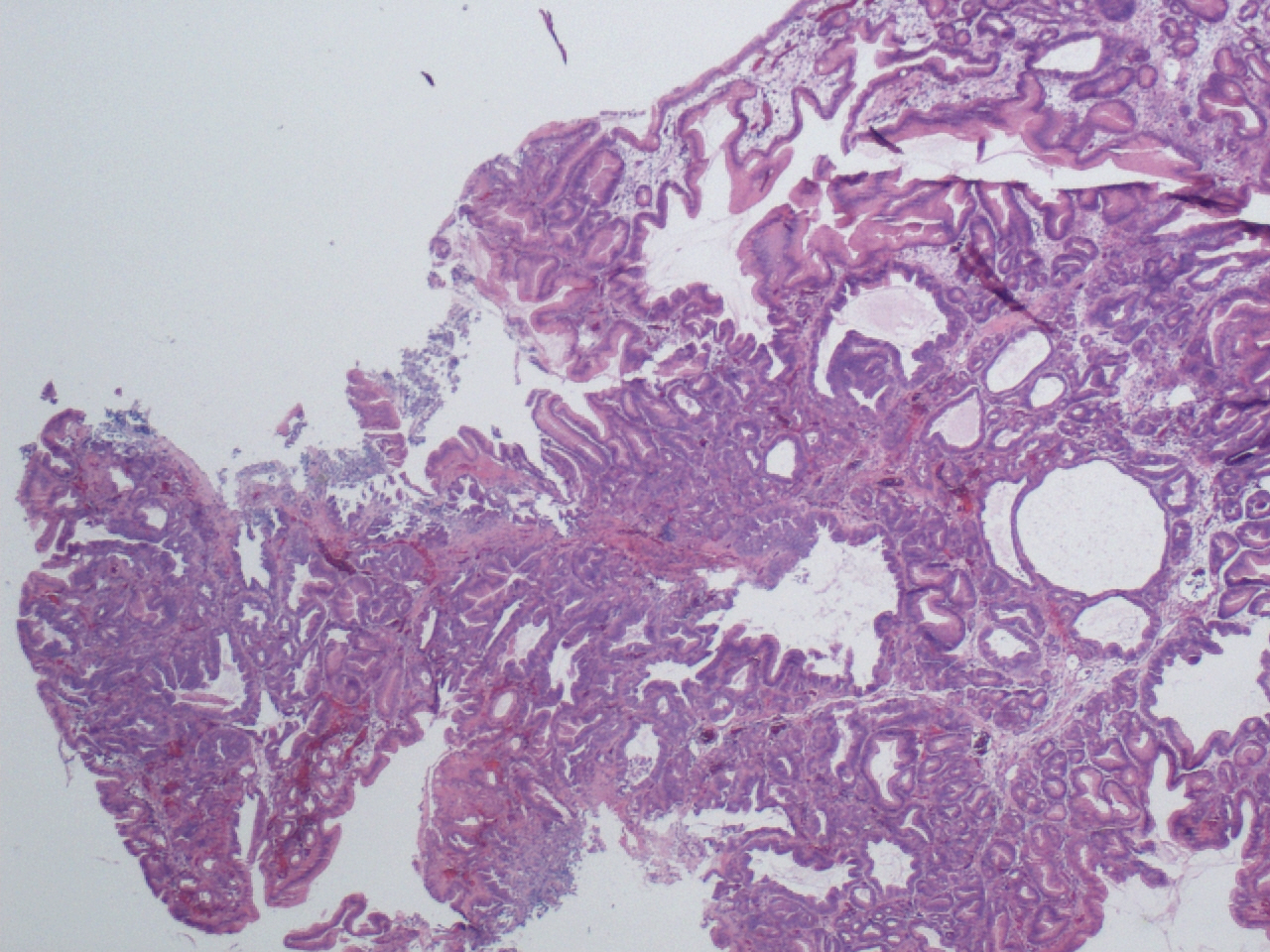
Figure 1: Specialized gastric mucosa consistent with biopsy taken from gastric fundus / body
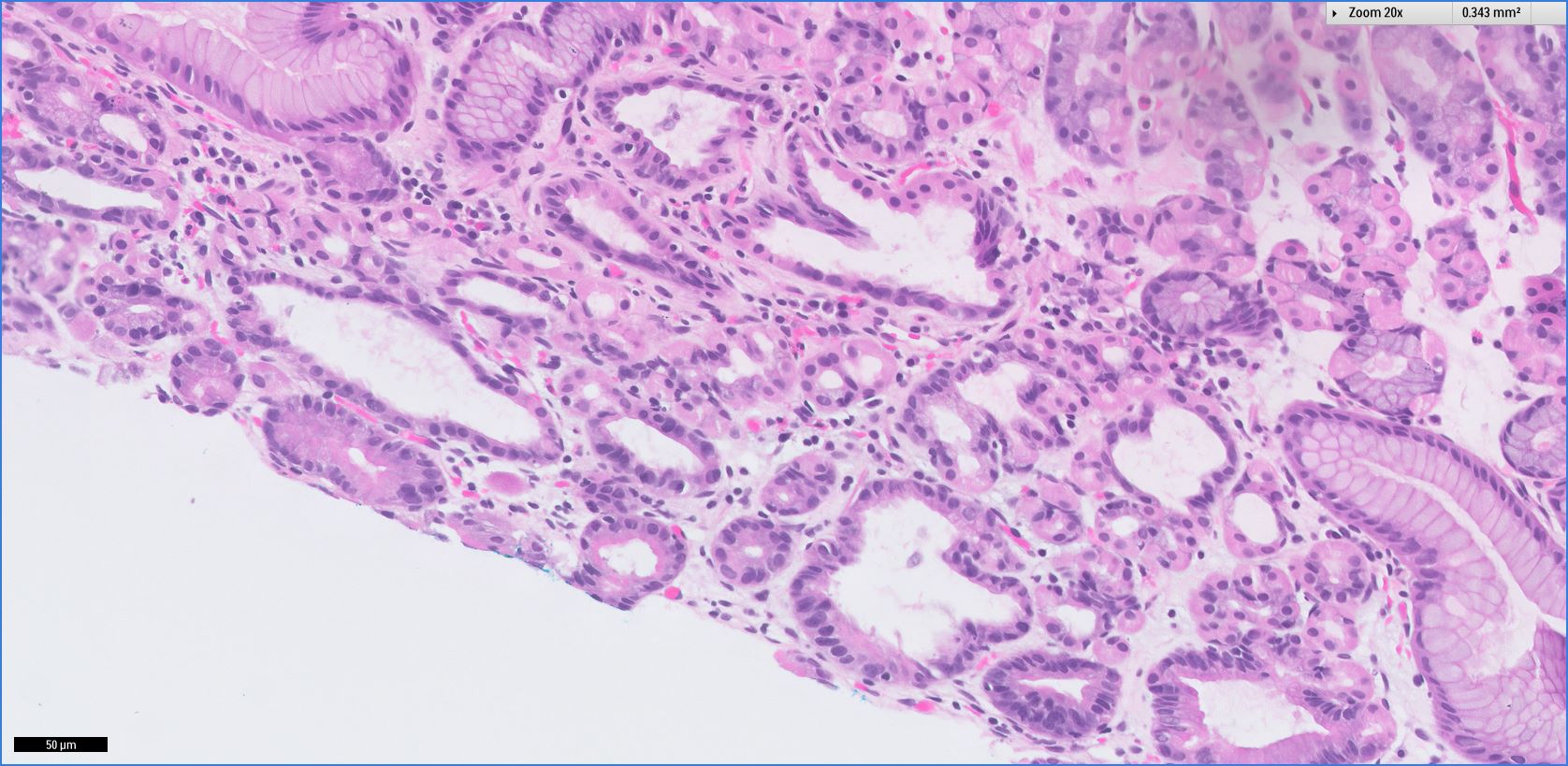
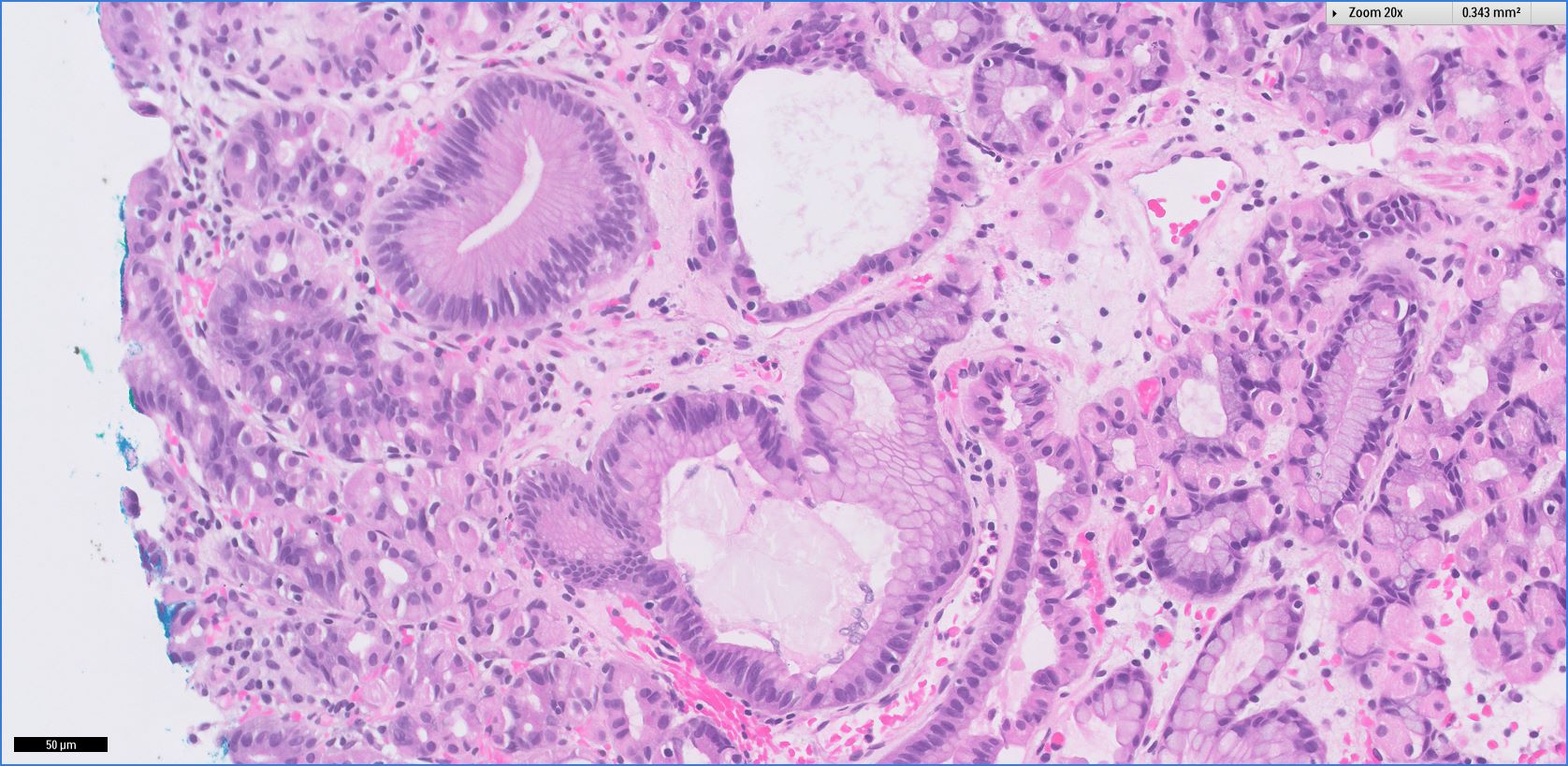
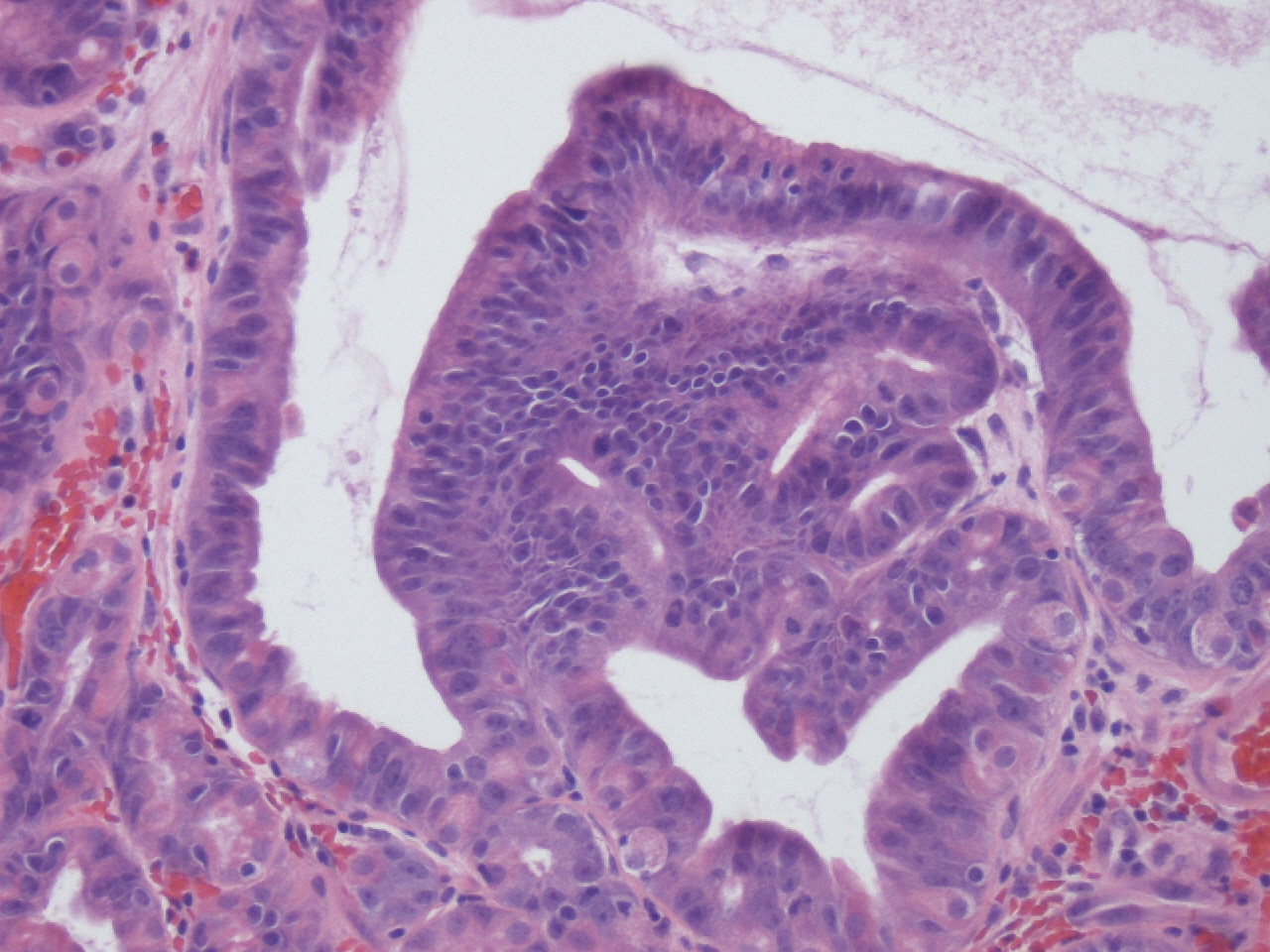
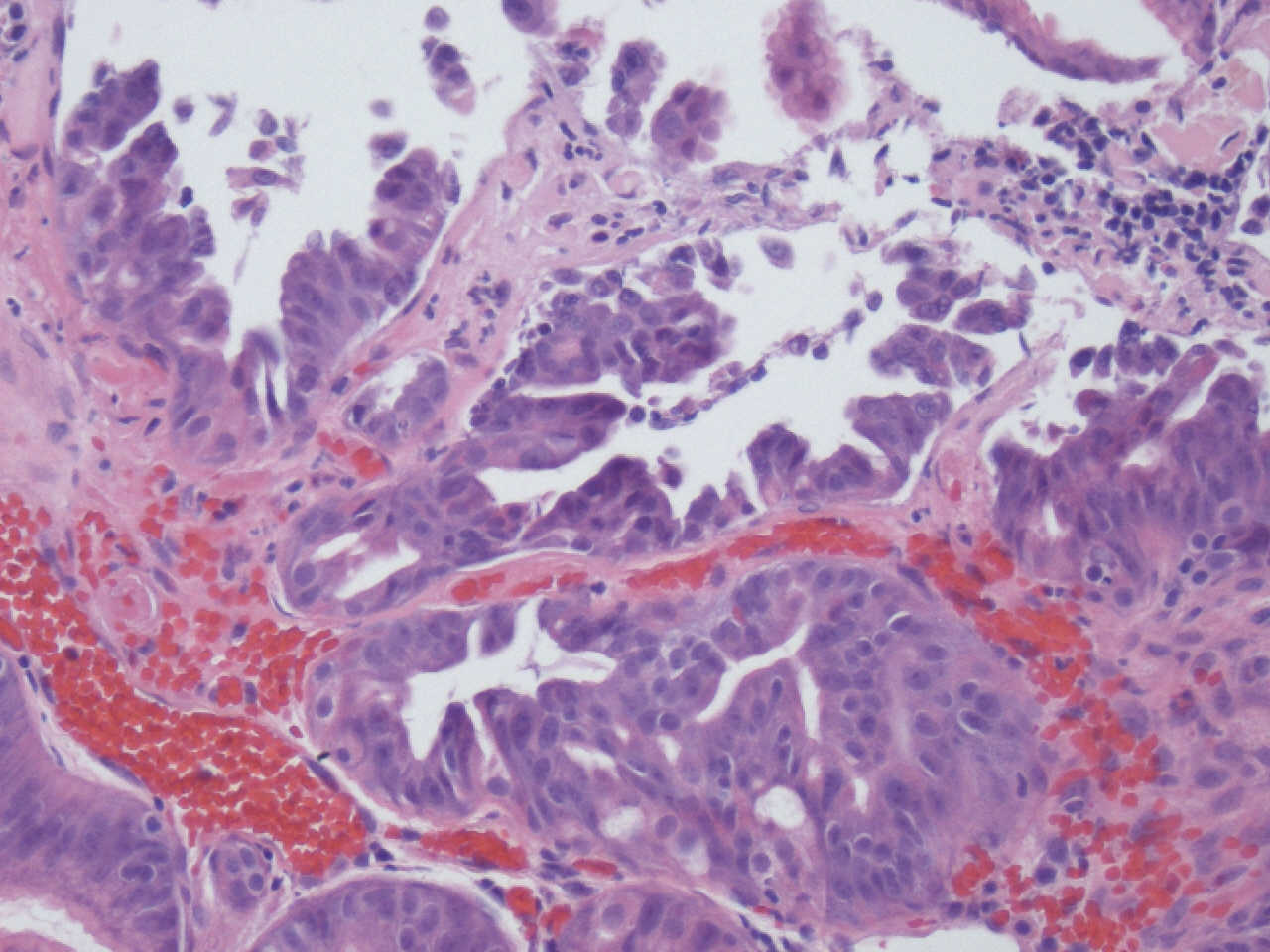
Figure 2, 3: Scattered dilated fundic type glands
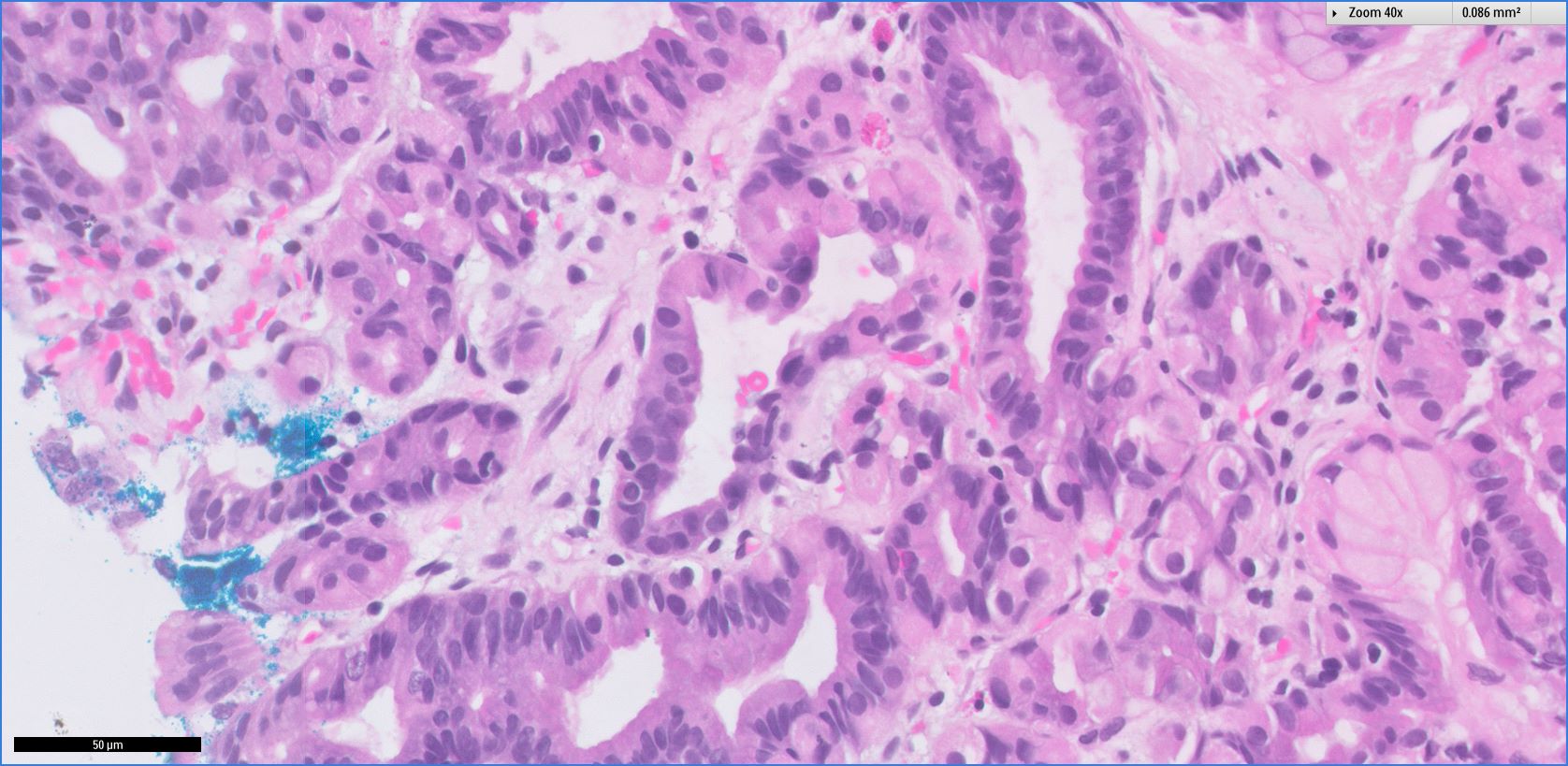
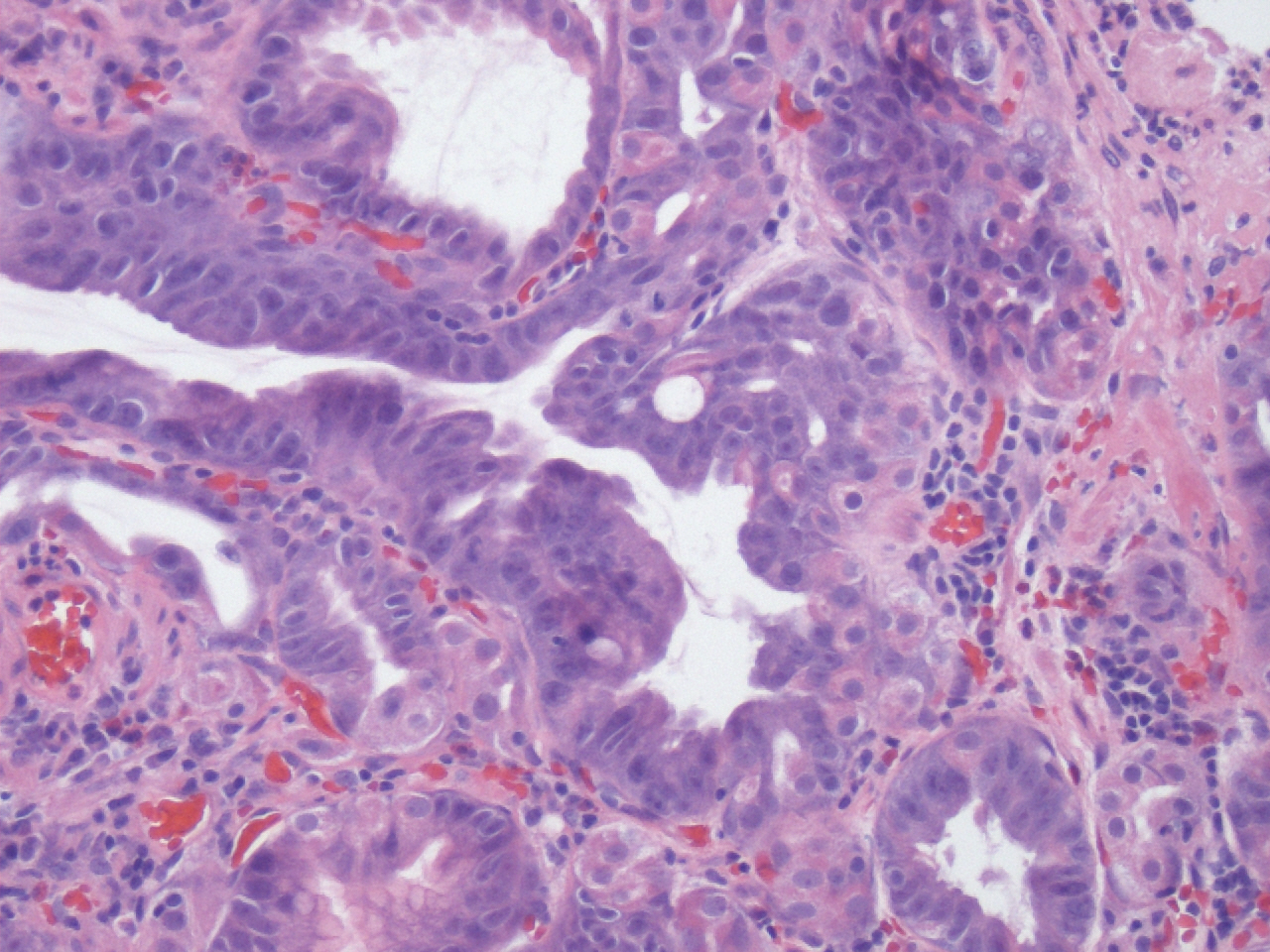
Figure 4, 5: Scattered dilated fundic type glands with nuclear enlargement, hyperchromasia and stratification; consistent with low grade dysplasia
Fundic gland polyps (FGPs) are one of the most common types of gastric polyps. Macroscopically, they are well circumscribed, smooth, sessile lesions that occur in gastric oxyntic mucosa. Histologically, fundic gland polyps are composed of cystically dilated and architecturally irregular fundic glands. They can occur sporadically or as part of familial adenomatous polyposis (FAP).
Sporadic FGPs have been associated with proton pump inhibitor use, and the morphology of FGPs can overlap with proton pump inhibitor effect (dilated oxyntic glands, cells with apocrine-like snouts). Sporadic FGPs very frequently have activating somatic mutations in CTNNB1.
FGPs were originally reported as a manifestation of FAP. FAP and attenuated FAP are autosomal dominant syndromes characterized by multiple adenomatous polyps in the colon and rectum due to APC mutations. FGPs occur in most patients with FAP and attenuated FAP, with about half of these patients having > 100 polyps (fundic gland polyposis). Although morphologically indistinguishable from sporadic FGPs, those associated with FAP / attenuated FAP have mutations in the APC gene. Detection of fundic gland polyps in younger individuals should always prompt consideration of FAP, as sporadic FGPs are extremely uncommon in the pediatric population.
Low grade dysplasia occurs in less than 1% of all sporadic FGPs. Features of dysplastic change include elongated hyperchromatic nuclei, increased nuclear-cytoplasmic ratio, nuclear pseudostratification and lack of surface maturation. Although sporadic FGPs with low grade dysplasia can have somatic mutations in APC, they have never been reported to progress to carcinoma. Dysplasia is much more common in FAP associated FGPs, and high grade dysplasia can be seen; however, progression to adenocarcinoma is still uncommon (Clin Gastroenterol Hepatol 2008;6:180).
Example of fundic gland polyp with dysplasia (another case):


Gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS) is a rare, recently described syndrome caused by a mutation in the APC gene promoter 1B with fundic gland polyposis and a significant risk of gastric cancer (Am J Hum Genet 2016;98:830). Although this gene is also affected in FAP / attenuated FAP, in GAPPS, duodenal and colorectal polyps are typically NOT seen.
Additional references: Montgomery (2012): Biopsy Interpretation of the Gastrointestinal Tract Mucosa
Discussion edited by: Dr. Hillary Z. Kimbrell, Myriad Genetics, Inc., Utah (USA)
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Leow Wei Qiang, Singapore General Hospital (Singapore) for contributing this case and discussion. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
New Books for May Listed on PathologyOutlines.com!
- Diagnostic Pathology: Genitourinary (2nd ed, 2016) by Mahul B. Amin, Satish K. Tickoo, 1072 pages, $293 list (Els.)
- Henry's Clinical Diagnosis and Management by Laboratory Methods (23rd ed, 2016) by Richard A. McPherson, Matthew R. Pincus, 1584 pages, $182 list (Els.)
To view more books recently listed on our site, click here.
Website news:
(1) If you are starting a new job or fellowship in June or July, please email us with your new email so you can continue to receive our newsletters.
(2) As of 18 May 2016, we have 5,267 followers on Twitter and 7,622 likes (business equivalent to "friends") on Facebook. Are you following PathologyOutlines.com on social media? If not, you may be missing out on quick access to updates, and occasional advertiser giveaways and specials, that are found on our Facebook and Twitter pages. Most recently, Mopec posted information about how to enter to win a free dissecting kit. Not only did someone win a dissecting kit, but Mopec reported an increase in followers across social channels and an increase in engagement and impressions. A win-win! For more information on posting on our Facebook and Twitter pages, contact us at (248) 646-0325 or pathoutads@gmail.com.
(3) We recently posted a new Management page article: Preparing for the Merit-Based Incentive Payment System by Alex Mitchell, Vachette Pathology. Keep your eyes open for other articles to be posted in upcoming weeks. We also recently posted information about new products being offered by Mopec and Milestone Medical. We post new information, as it becomes available, on our New Products and Services page.
Visit and follow our Blog to see recent updates to the website.
Case of the Week #389
Clinical history:
A 27 year old man with familial adenomatous polyposis (FAP), status post pan-proctocolectomy 10 years ago, underwent an elective gastroscopy. There were multiple polyps identified in the gastric fundus and body, which were biopsied.
Gross description:
The specimen consists of two pieces of tissue measuring 0.2 cm and 0.5 cm.
Micro images:
20x
100x
200x
400x
What is your diagnosis?
Diagnosis:
Familial adenomatous polyposis (FAP) associated fundic gland polyps with low grade dysplasia
Discussion:
The biopsies were described as follows:
Figure 1: Specialized gastric mucosa consistent with biopsy taken from gastric fundus / body
Figure 2, 3: Scattered dilated fundic type glands
Figure 4, 5: Scattered dilated fundic type glands with nuclear enlargement, hyperchromasia and stratification; consistent with low grade dysplasia
Fundic gland polyps (FGPs) are one of the most common types of gastric polyps. Macroscopically, they are well circumscribed, smooth, sessile lesions that occur in gastric oxyntic mucosa. Histologically, fundic gland polyps are composed of cystically dilated and architecturally irregular fundic glands. They can occur sporadically or as part of familial adenomatous polyposis (FAP).
Sporadic FGPs have been associated with proton pump inhibitor use, and the morphology of FGPs can overlap with proton pump inhibitor effect (dilated oxyntic glands, cells with apocrine-like snouts). Sporadic FGPs very frequently have activating somatic mutations in CTNNB1.
FGPs were originally reported as a manifestation of FAP. FAP and attenuated FAP are autosomal dominant syndromes characterized by multiple adenomatous polyps in the colon and rectum due to APC mutations. FGPs occur in most patients with FAP and attenuated FAP, with about half of these patients having > 100 polyps (fundic gland polyposis). Although morphologically indistinguishable from sporadic FGPs, those associated with FAP / attenuated FAP have mutations in the APC gene. Detection of fundic gland polyps in younger individuals should always prompt consideration of FAP, as sporadic FGPs are extremely uncommon in the pediatric population.
Low grade dysplasia occurs in less than 1% of all sporadic FGPs. Features of dysplastic change include elongated hyperchromatic nuclei, increased nuclear-cytoplasmic ratio, nuclear pseudostratification and lack of surface maturation. Although sporadic FGPs with low grade dysplasia can have somatic mutations in APC, they have never been reported to progress to carcinoma. Dysplasia is much more common in FAP associated FGPs, and high grade dysplasia can be seen; however, progression to adenocarcinoma is still uncommon (Clin Gastroenterol Hepatol 2008;6:180).
Example of fundic gland polyp with dysplasia (another case):
Contributed by: Dr. Anne Herdman, PathGroup / Associated Pathologists, Tennessee (USA)
Gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS) is a rare, recently described syndrome caused by a mutation in the APC gene promoter 1B with fundic gland polyposis and a significant risk of gastric cancer (Am J Hum Genet 2016;98:830). Although this gene is also affected in FAP / attenuated FAP, in GAPPS, duodenal and colorectal polyps are typically NOT seen.
Additional references: Montgomery (2012): Biopsy Interpretation of the Gastrointestinal Tract Mucosa
Discussion edited by: Dr. Hillary Z. Kimbrell, Myriad Genetics, Inc., Utah (USA)