
3 September 2015 - Case of the Week #363
All cases are archived on our website. To view them sorted by number, diagnosis or category, visit our Home Page and click on the Case of the Week button. To subscribe or unsubscribe to the Case of the Week or our other email lists, click here.
Thanks to Dr. Fatima Akhlaqi, Aga Khan University Hospital (Pakistan), for contributing this case, and to Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences, for the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto. To contribute a Case of the Week, follow the guidelines on our Case of the Week page.
Advertisement
Website news:
(1) Our Feature page for September is Antibodies / Biomarkers, and highlights our advertisers Advanced Cell Diagnostics, Inc. (ACD) and Ventana Medical. It also contains an original short article, "Biomarkers in Proteomics: Deciphering Protein Signatures", by Jaleh Mansouri, M.D.
(2) The number of subscribers continues to increase for our email newsletters. As of 3 September 2015, we have 6010 subscribers to the Case of the Week email, 4163 subscribers to the Jobs, Fellowships and Conferences email and 3119 subscribers to the Website News email. Click here to review your email preferences.
(3) Thanks to J. Manuel Gamboa M.D., our newest member, see our Membership page. Thanks for supporting PathologyOutlines.com - visit our Individual Membership page to see why you should become a member too!
(4) Welcome to Dr. Jennifer Kaley, University of Arkansas for Medical Sciences (USA), our Case of the Week author for discussions.
(5) We have starting the second phase of our website upgrade. In the first phase, we gave the Home Page a cleaner look, and converted all interior pages to a database format (although not apparent to users). In Phase 2, our interior pages will also have a cleaner look.
(6) Visit our Blog to see recent updates to the website.
Case of the Week #363
Clinical History:
A 14 year old girl with vaginal bleeding had a mass involving the vagina and cervix.
Micro images:
What is your diagnosis?
Diagnosis:
Clear cell carcinoma of the vagina and cervix
Discussion:
Clear cell adenocarcinoma (CCA) of the vagina and cervix is rare, accounting for 5-10% of vaginal malignancies. The association of CCA with in-utero exposure to diethylstilbestrol (DES) has been well documented; however, cases of primary vaginal clear cell carcinoma not associated with DES have been reported in the literature in the settings of vaginal endometriosis (Acta Cytol 2002;46:577, Iran J Med Sci 2014;39:298, Gynecol Oncol 2006;103:1130) and congenital anomalies of the genitourinary tract (J Obstet Gynaecol Res 2010;36:681). The age distribution is therefore bimodal, with the age of diagnosis among DES exposed patients between 14 to 22 years (median age of 19 years) and 55 years in postmenopausal women with no history of DES exposure (N Engl J Med 1987;316:514, Gynecol Oncol 2006;103:1130).
Diethylstilbestrol (DES) is a synthetic estrogen used off-label from the early 1940's through 1975 to prevent adverse pregnancy outcomes in women with a history of miscarriage. DES disrupts normal embryogenesis of the female genital tract by inhibiting the replacement of the Müllerian duct-derived columnar epithelium with ascending squamous epithelium from the urogenital sinus, resulting in persistence of glandular epithelium. In most cases, squamous metaplasia ensues as the patient ages; rarely, the ectopic glandular epithelium undergoes malignant transformation (Can Fam Physician 1984;30:1679). The risk of developing CCA among the exposed is small, on the order of 1 in 1,000. The rarity of this tumor among exposed women suggests that diethylstilbestrol is not a complete carcinogen and that other factors such as obesity and unopposed estrogens are involved in the pathogenesis (N Engl J Med 1987;316:514, Am J Obstet Gynecol 1977;128:43, Gynecol Oncol 2006;103:1130).
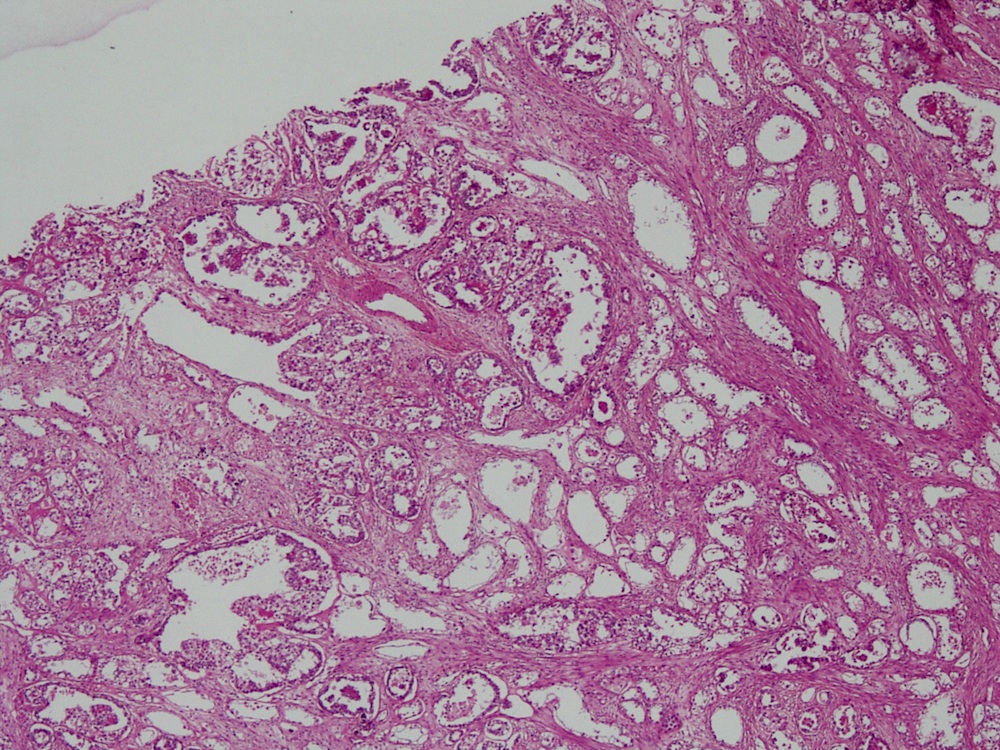
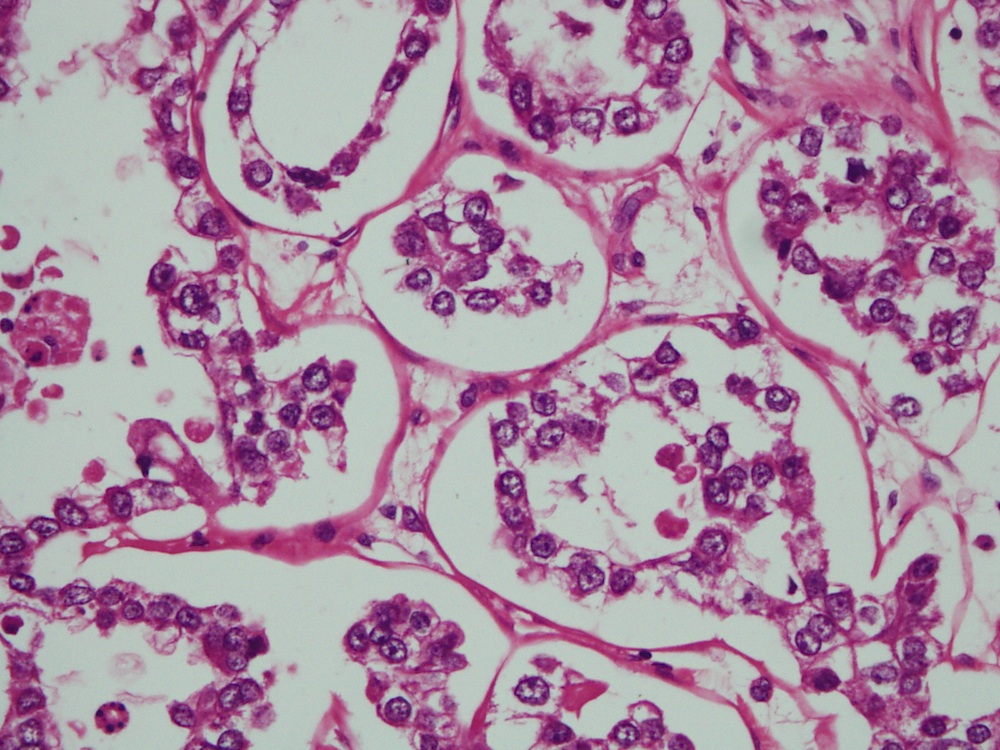
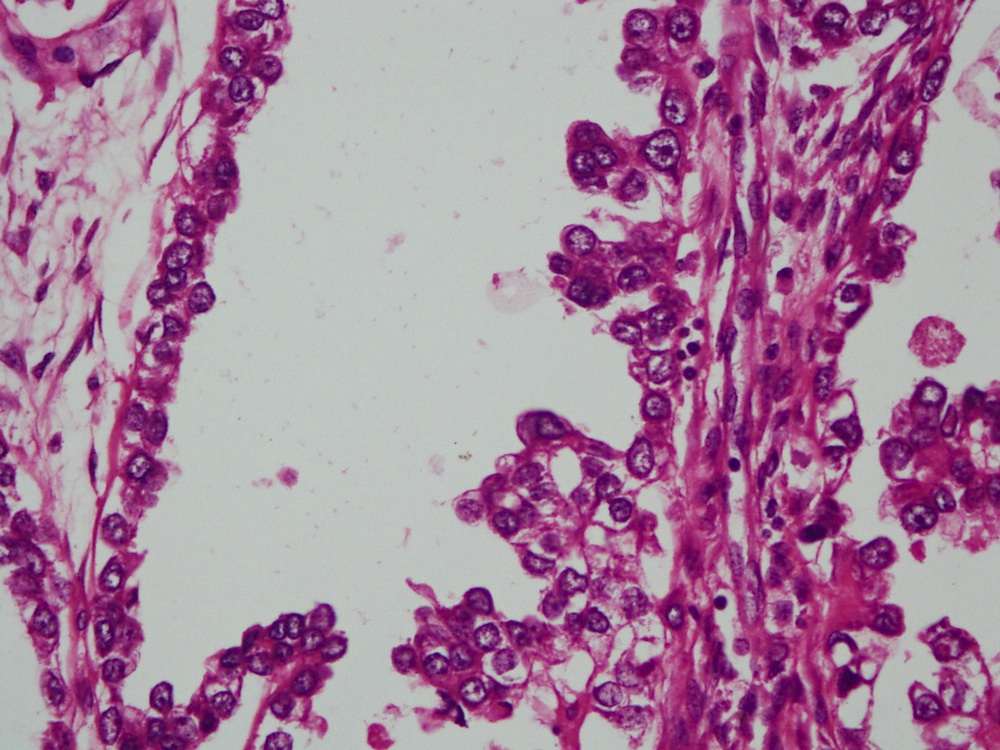
CCA of the vagina and cervix usually presents with abnormal vaginal bleeding (Gynecol Oncol 2007;105:273), and clinical exam reveals a polypoid mass originating from the upper two-thirds of the anterior vaginal wall. Biopsy shows cuboidal cells with eosinophilic to clear cytoplasm (figure 16) arranged in cystic, papillary, tubular or solid configurations (figure 1). Areas of necrosis may be seen. Nuclei may protrude into the lumina, imparting a "hobnail" appearance (figure 18), and glycogen is abundant. The immunophenotype is similar to CCA arising elsewhere in the gynecologic tract, showing positivity for CK7, CAM5.2, 34 beta E12, and CA125 (Int J Gynecol Pathol 2001;20:252). NapsinA, HNF1 and AMACR are frequently positive; of theses NapsinA offers the best sensitivity and specificity (Obstet Gynecol Int 2019;2019:9465375, Pathology 2015;47:105, Int J Gynecol Pathol 2019;38:276). Most cases show normal expression of p53. Monoclonal CEA is negative (Am J Surg Pathol 2011;35:633).
Treatment can involve surgical intervention and radiation therapy. Non DES associated adenocarcinomas generally have a worse prognosis than SCC tumors, especially when present at a younger age, but DES associated clear cell tumors have a relatively good prognosis (DeVita: Cancer Principles and Practice of Oncology (2014), Iran J Med Sci 2014;39:298). The overall recurrence rate for clear cell carcinoma approaches 21%, with the lungs, supraclavicular lymph nodes and pelvis being the most common areas, although cerebral metastasis has also been reported (Gynecol Oncol 2007;105:273, Am J Obstet Gynecol 1979;135:876). Recurrence has been observed as long as 20 years after primary therapy emphasizing the importance of prolonged follow-up (Semin Surg Oncol 1990;6:343).
Discussion by Jennifer R. Kaley, M.D., University of Arkansas for Medical Sciences
All cases are archived on our website. To view them sorted by number, diagnosis or category, visit our Home Page and click on the Case of the Week button. To subscribe or unsubscribe to the Case of the Week or our other email lists, click here.
Thanks to Dr. Fatima Akhlaqi, Aga Khan University Hospital (Pakistan), for contributing this case, and to Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences, for the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto. To contribute a Case of the Week, follow the guidelines on our Case of the Week page.
- Diagnostic Pathology: Gastrointestinal (2nd ed) by Joel Greenson, M.D. 2015, 800 pages, 2,500+ illus, $230 list (Els.)
- OB-GYN Pathology for the Clinician by Debra Heller, 2015, 254 pages, 393 illus, $109 list (Spr.)
For more information, visit our New Books page.
Website news:
(1) Our Feature page for September is Antibodies / Biomarkers, and highlights our advertisers Advanced Cell Diagnostics, Inc. (ACD) and Ventana Medical. It also contains an original short article, "Biomarkers in Proteomics: Deciphering Protein Signatures", by Jaleh Mansouri, M.D.
(2) The number of subscribers continues to increase for our email newsletters. As of 3 September 2015, we have 6010 subscribers to the Case of the Week email, 4163 subscribers to the Jobs, Fellowships and Conferences email and 3119 subscribers to the Website News email. Click here to review your email preferences.
(3) Thanks to J. Manuel Gamboa M.D., our newest member, see our Membership page. Thanks for supporting PathologyOutlines.com - visit our Individual Membership page to see why you should become a member too!
(4) Welcome to Dr. Jennifer Kaley, University of Arkansas for Medical Sciences (USA), our Case of the Week author for discussions.
(5) We have starting the second phase of our website upgrade. In the first phase, we gave the Home Page a cleaner look, and converted all interior pages to a database format (although not apparent to users). In Phase 2, our interior pages will also have a cleaner look.
(6) Visit our Blog to see recent updates to the website.
Case of the Week #363
Clinical History:
A 14 year old girl with vaginal bleeding had a mass involving the vagina and cervix.
Micro images:
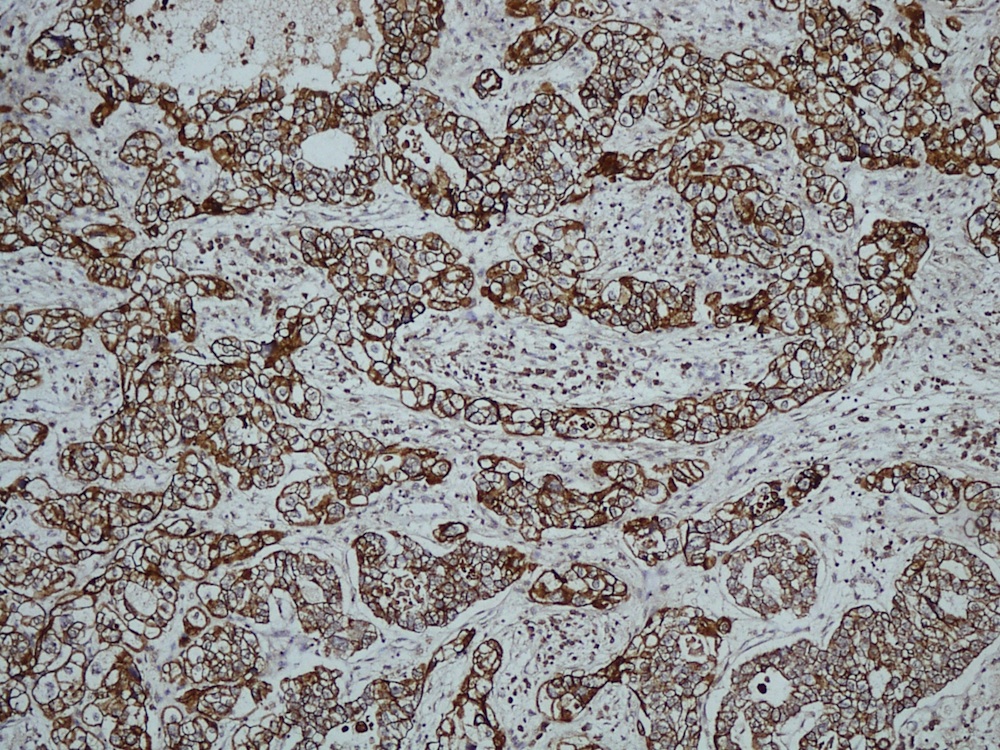
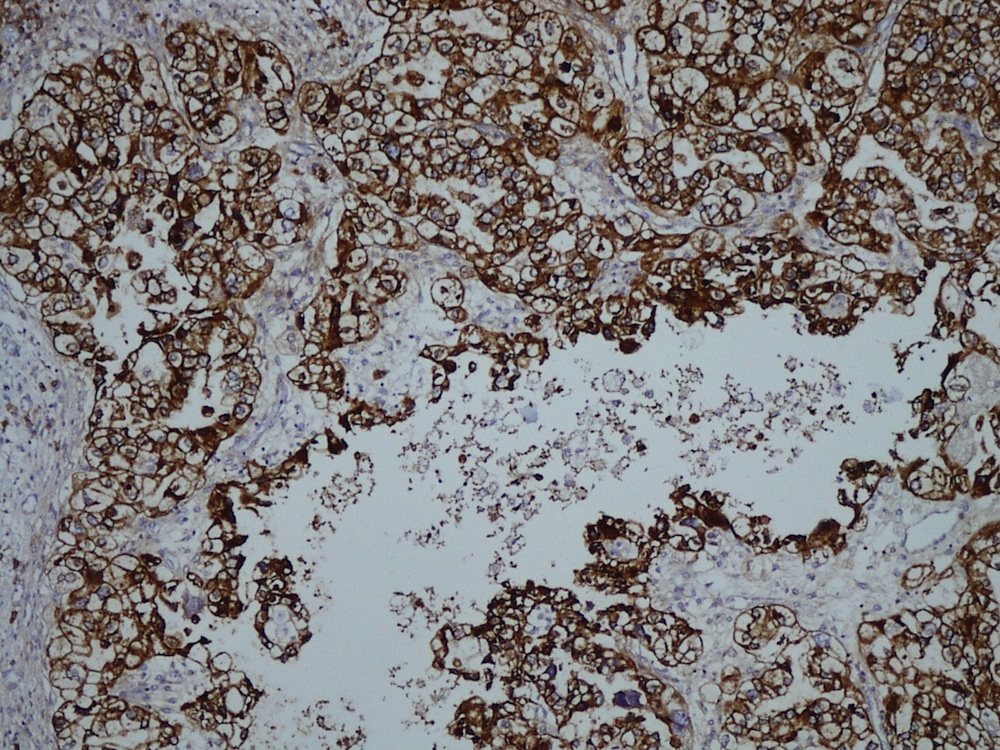
CK7
EMA
What is your diagnosis?
Diagnosis:
Clear cell carcinoma of the vagina and cervix
Discussion:
Clear cell adenocarcinoma (CCA) of the vagina and cervix is rare, accounting for 5-10% of vaginal malignancies. The association of CCA with in-utero exposure to diethylstilbestrol (DES) has been well documented; however, cases of primary vaginal clear cell carcinoma not associated with DES have been reported in the literature in the settings of vaginal endometriosis (Acta Cytol 2002;46:577, Iran J Med Sci 2014;39:298, Gynecol Oncol 2006;103:1130) and congenital anomalies of the genitourinary tract (J Obstet Gynaecol Res 2010;36:681). The age distribution is therefore bimodal, with the age of diagnosis among DES exposed patients between 14 to 22 years (median age of 19 years) and 55 years in postmenopausal women with no history of DES exposure (N Engl J Med 1987;316:514, Gynecol Oncol 2006;103:1130).
Diethylstilbestrol (DES) is a synthetic estrogen used off-label from the early 1940's through 1975 to prevent adverse pregnancy outcomes in women with a history of miscarriage. DES disrupts normal embryogenesis of the female genital tract by inhibiting the replacement of the Müllerian duct-derived columnar epithelium with ascending squamous epithelium from the urogenital sinus, resulting in persistence of glandular epithelium. In most cases, squamous metaplasia ensues as the patient ages; rarely, the ectopic glandular epithelium undergoes malignant transformation (Can Fam Physician 1984;30:1679). The risk of developing CCA among the exposed is small, on the order of 1 in 1,000. The rarity of this tumor among exposed women suggests that diethylstilbestrol is not a complete carcinogen and that other factors such as obesity and unopposed estrogens are involved in the pathogenesis (N Engl J Med 1987;316:514, Am J Obstet Gynecol 1977;128:43, Gynecol Oncol 2006;103:1130).
CCA of the vagina and cervix usually presents with abnormal vaginal bleeding (Gynecol Oncol 2007;105:273), and clinical exam reveals a polypoid mass originating from the upper two-thirds of the anterior vaginal wall. Biopsy shows cuboidal cells with eosinophilic to clear cytoplasm (figure 16) arranged in cystic, papillary, tubular or solid configurations (figure 1). Areas of necrosis may be seen. Nuclei may protrude into the lumina, imparting a "hobnail" appearance (figure 18), and glycogen is abundant. The immunophenotype is similar to CCA arising elsewhere in the gynecologic tract, showing positivity for CK7, CAM5.2, 34 beta E12, and CA125 (Int J Gynecol Pathol 2001;20:252). NapsinA, HNF1 and AMACR are frequently positive; of theses NapsinA offers the best sensitivity and specificity (Obstet Gynecol Int 2019;2019:9465375, Pathology 2015;47:105, Int J Gynecol Pathol 2019;38:276). Most cases show normal expression of p53. Monoclonal CEA is negative (Am J Surg Pathol 2011;35:633).
Treatment can involve surgical intervention and radiation therapy. Non DES associated adenocarcinomas generally have a worse prognosis than SCC tumors, especially when present at a younger age, but DES associated clear cell tumors have a relatively good prognosis (DeVita: Cancer Principles and Practice of Oncology (2014), Iran J Med Sci 2014;39:298). The overall recurrence rate for clear cell carcinoma approaches 21%, with the lungs, supraclavicular lymph nodes and pelvis being the most common areas, although cerebral metastasis has also been reported (Gynecol Oncol 2007;105:273, Am J Obstet Gynecol 1979;135:876). Recurrence has been observed as long as 20 years after primary therapy emphasizing the importance of prolonged follow-up (Semin Surg Oncol 1990;6:343).
Discussion by Jennifer R. Kaley, M.D., University of Arkansas for Medical Sciences
