1 October 2014 - Case #328
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Oana Rafael, Lenox Hill Hospital, New York (USA), for contributing this case and discussion.
For more information, visit our Books page.
Advertisement
Case #328
Clinical history:
A 34 year old man had gradually increasing abdominal and left scrotal pain. Scrotal ultrasound demonstrated a left testicular heterogeneous hypoechoic lesion with no significant internal vascularity (figures 1, 2). Radical orchiectomy was performed.
The testis was bivalved to show a hemorrhagic, well defined, soft, dark red lesion (figure 3).
Scrotal ultrasound:


Gross images:

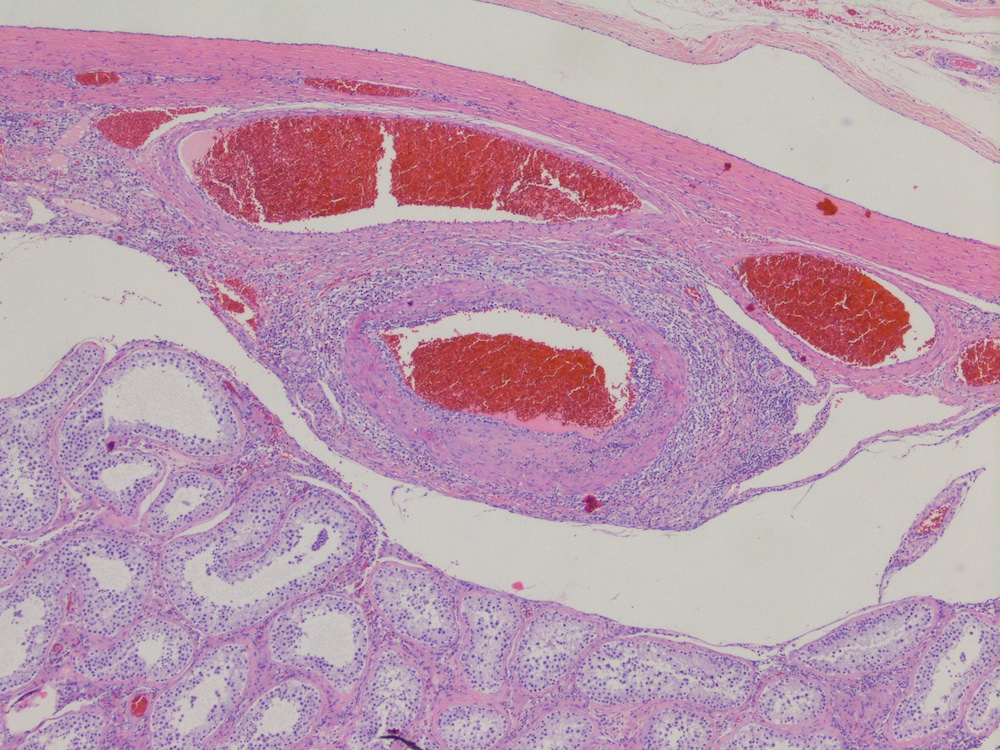
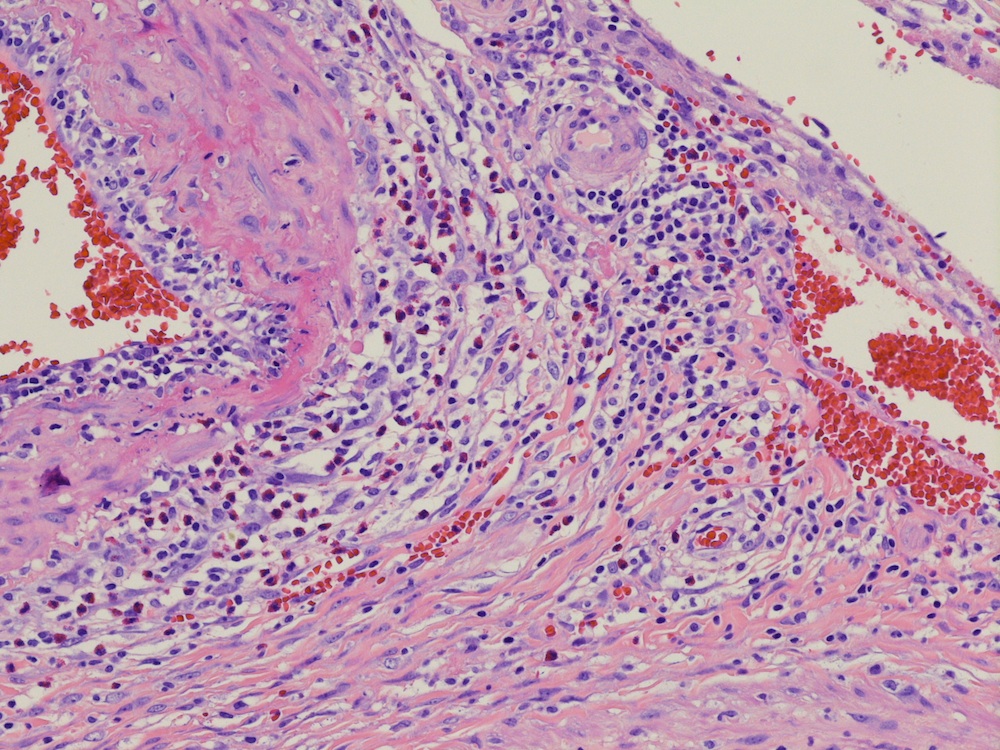
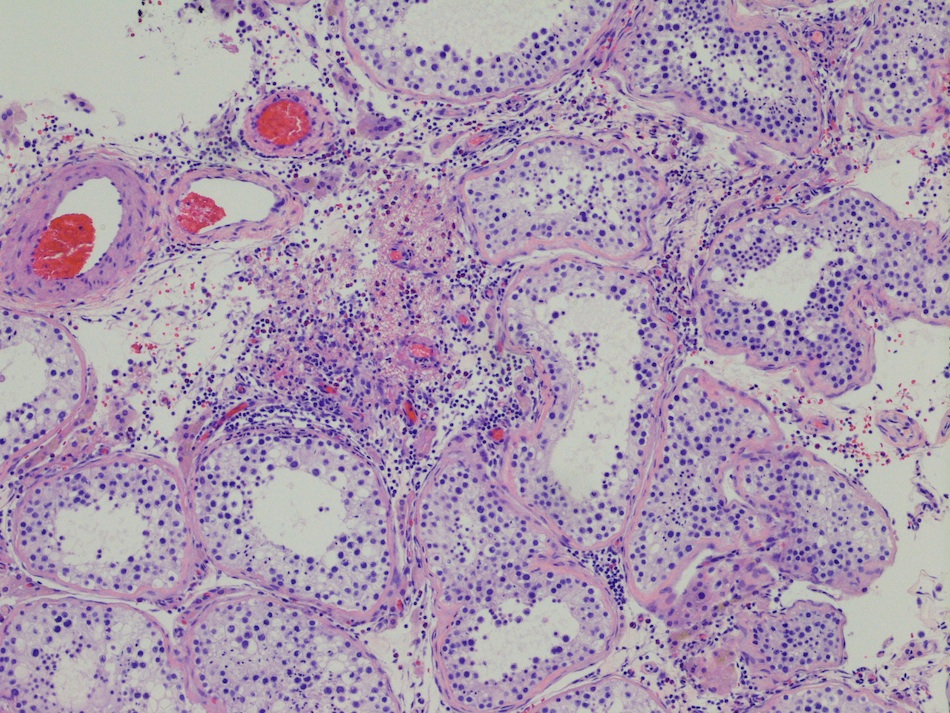
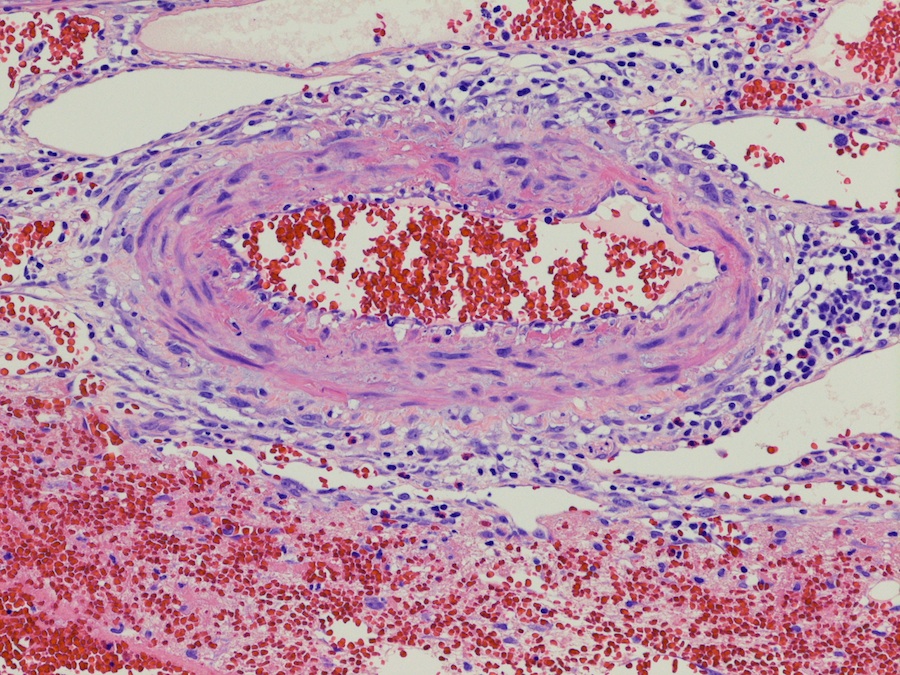
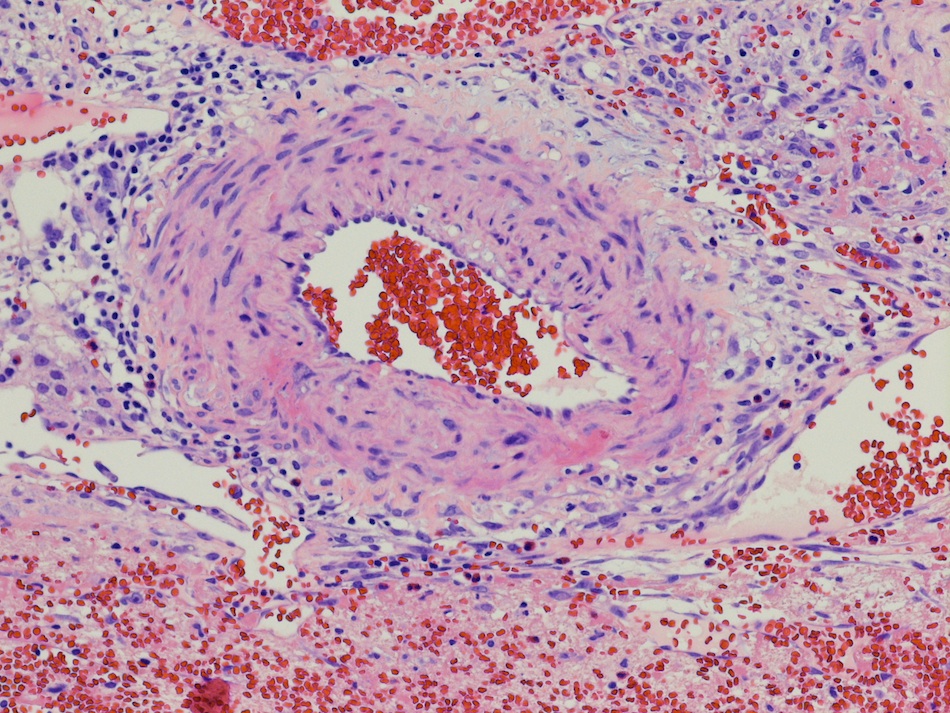
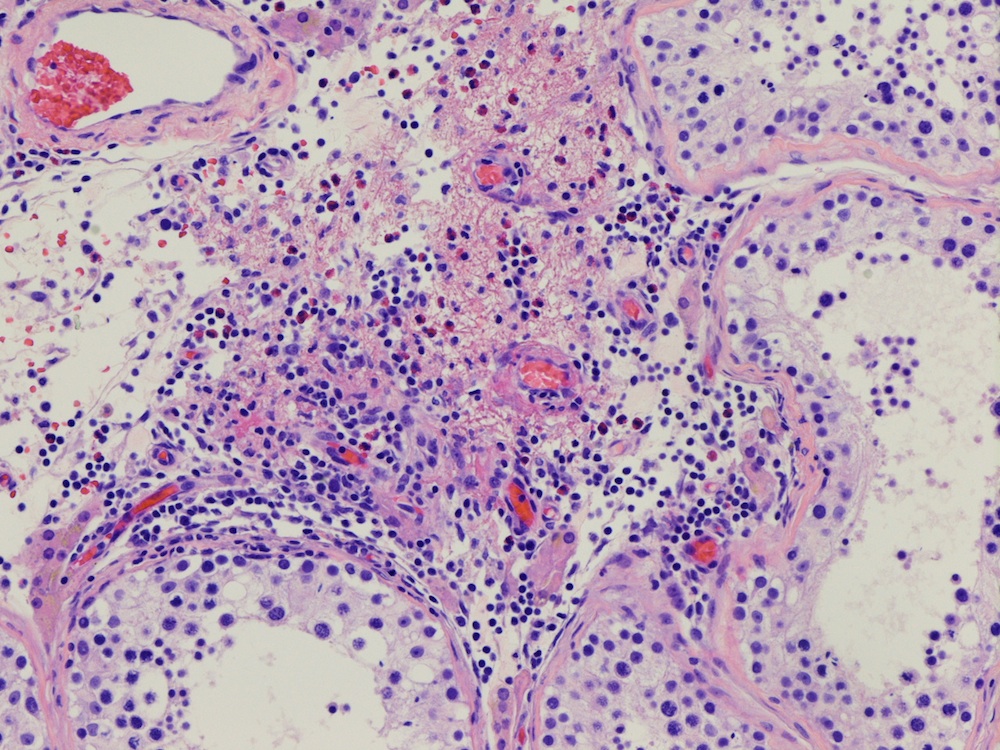
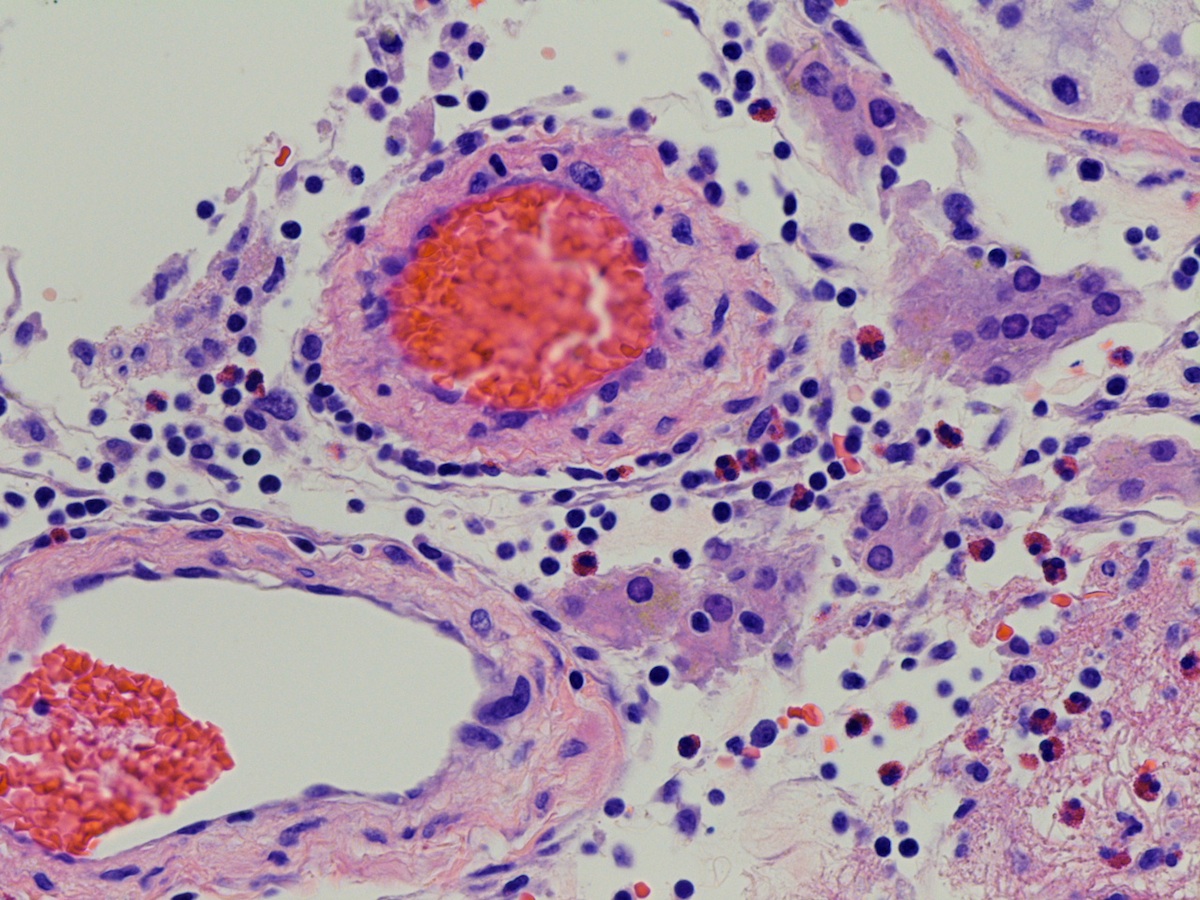
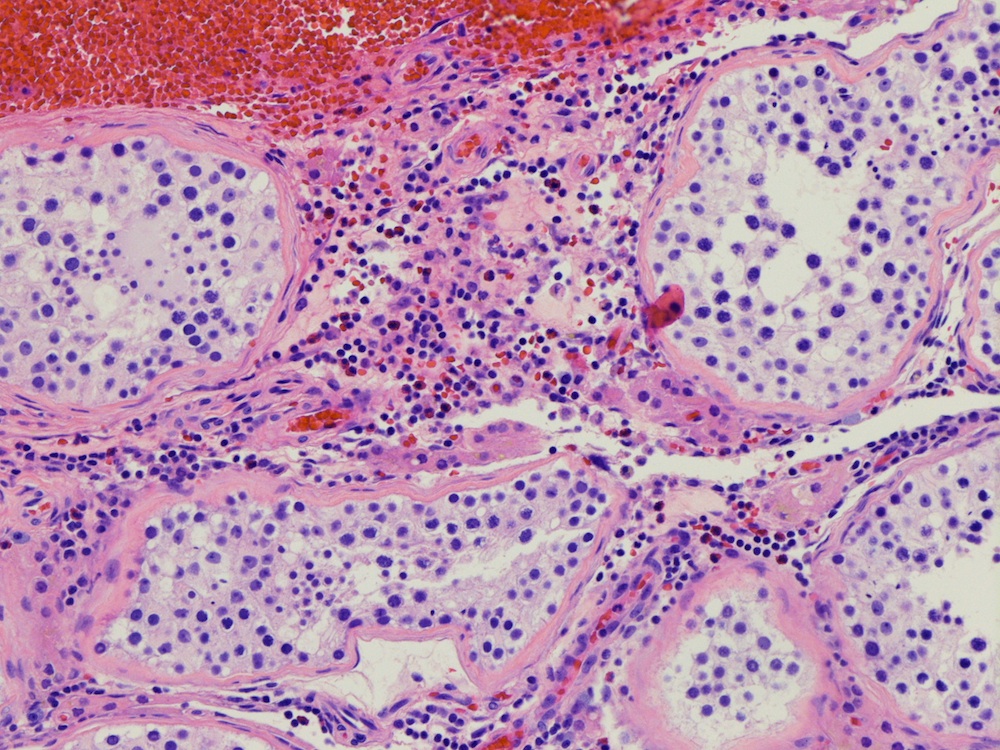
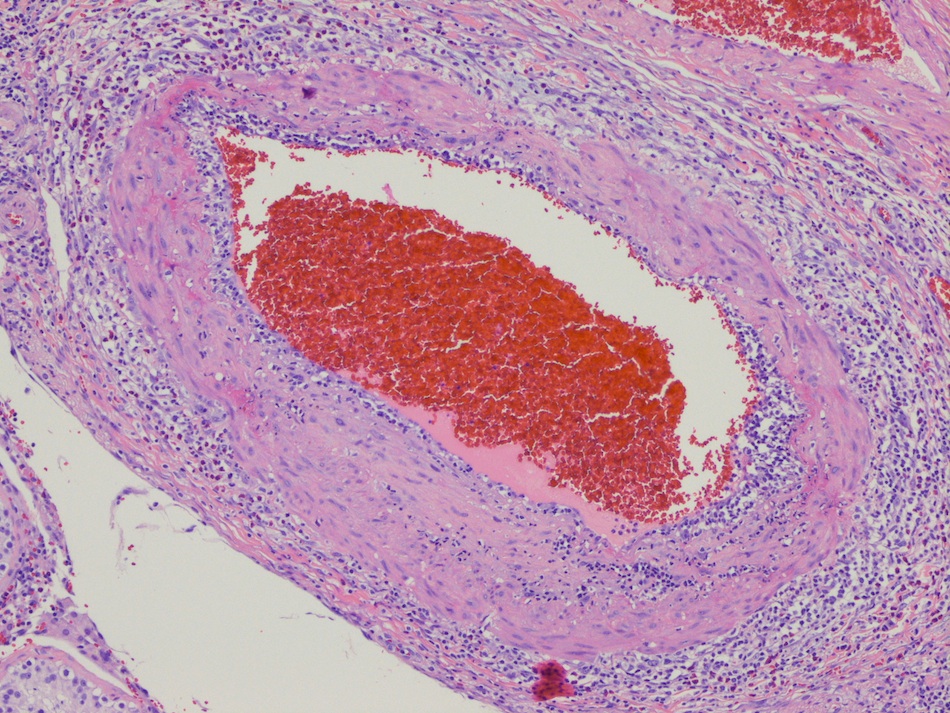
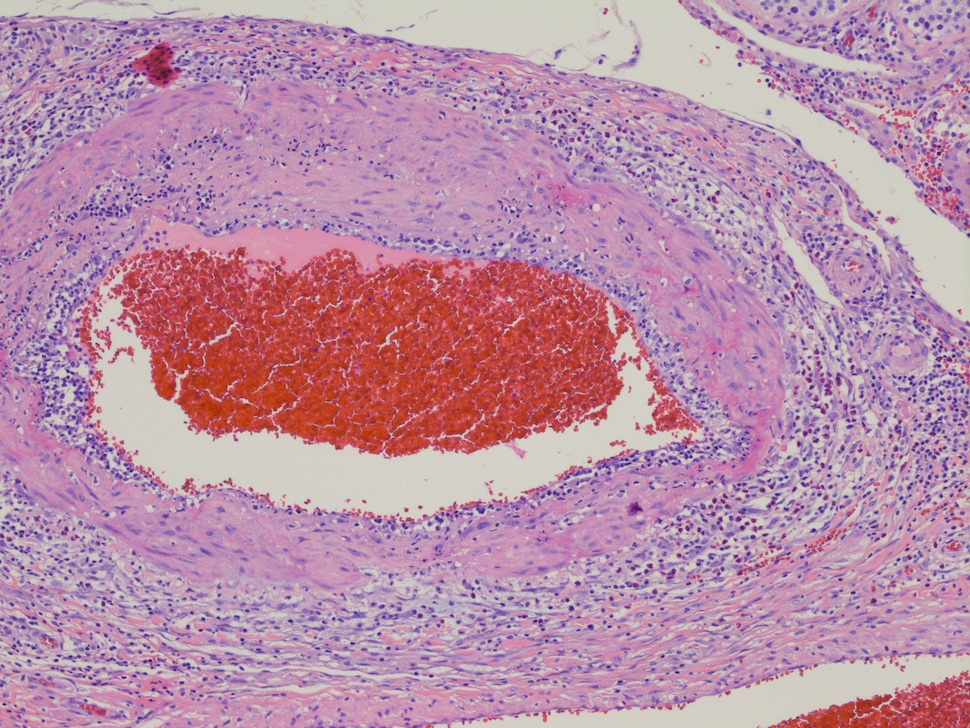
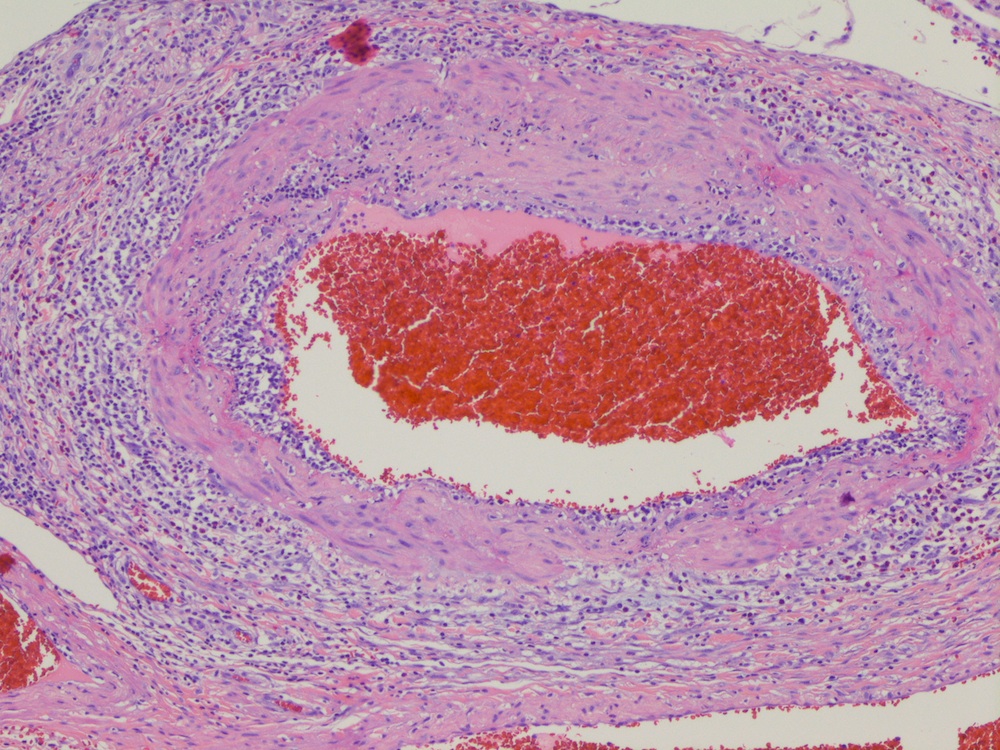
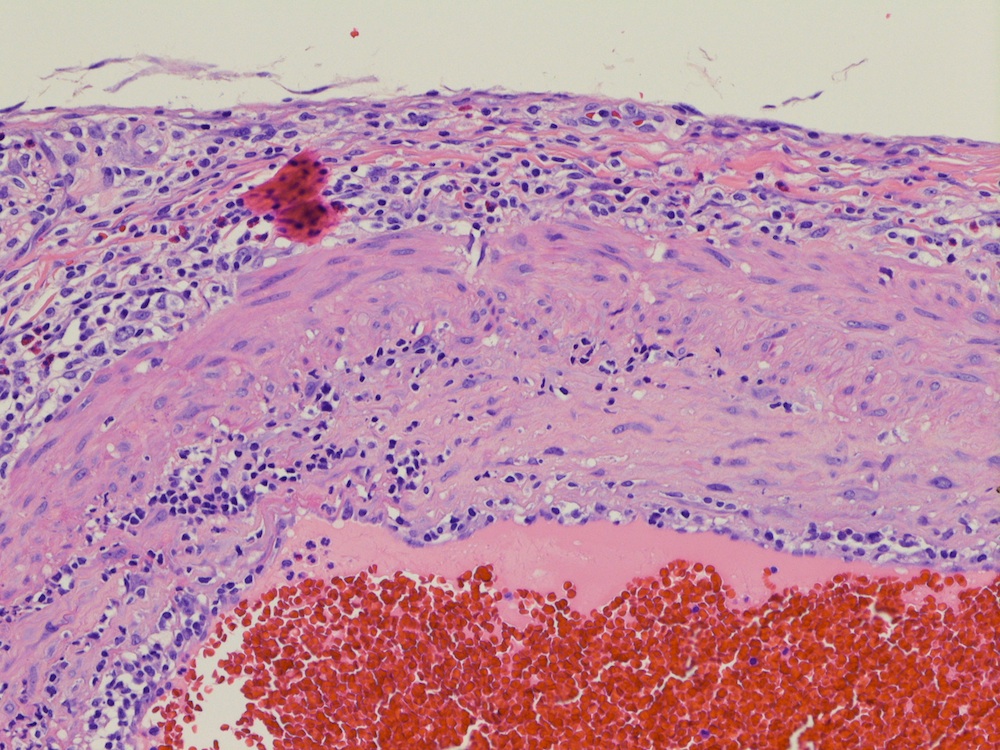
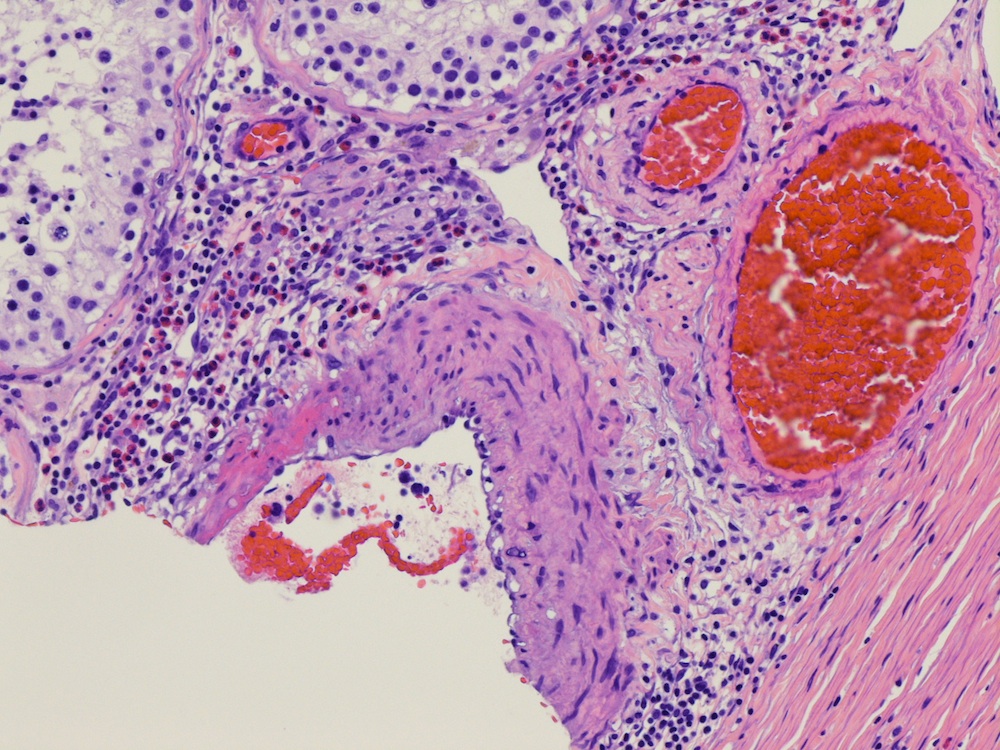
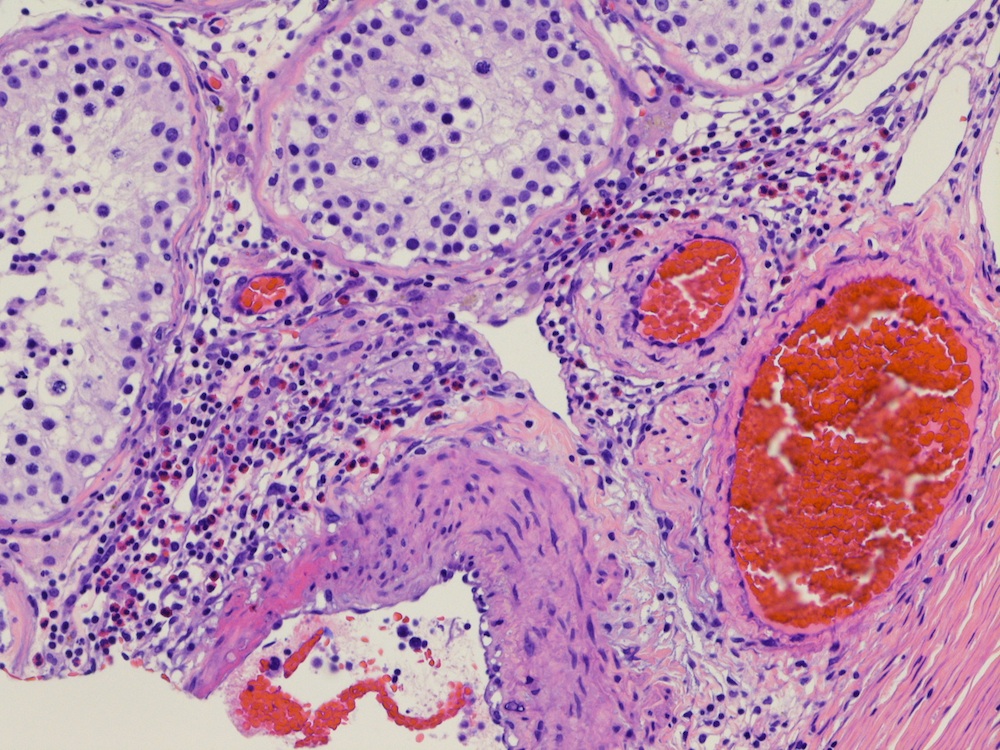
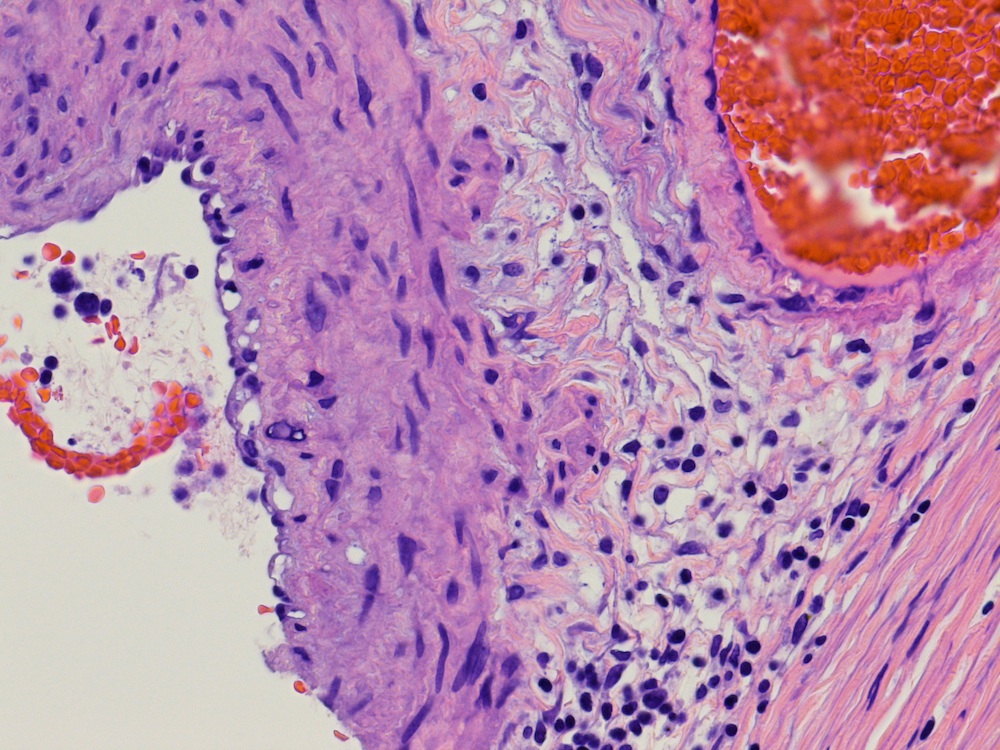
Microscopic images:






What is your diagnosis?
Diagnosis: Testicular necrotizing vasculitis
Discussion:
Microscopic examination of the lesion revealed focal hemorrhage with early organization and small arteries around the area of hemorrhage showing necrotizing vasculitis.
Necrotizing vasculitis is a systemic disease which manifests as inflammation of arteries with fibrinoid necrosis and fibrosis of the vascular wall. It can be associated with a variety of other entities or may be idiopathic (Cardiovascular Pathology 1994;3:197). While necrotizing vasculitis can involve any organ, isolated testicular involvement is rare and can pose diagnostic difficulties, especially in the absence of clinical and laboratory evidence of systemic involvement (World J Surg Oncol 2011;9:63).
Polyarteritis nodosa (PAN) is the most common form of testicular vasculitis, predominantly seen in the fourth to sixth decades of life. It is often associated with hepatitis B virus and human immunodeficiency virus. Although 60% to 86% of patients with PAN show testicular involvement at autopsy (ScientificWorldJournal 2010;10:1915), testicular symptoms are present in < 20% of patients (Hum Pathol 1988;19:186). Other vasculitides that may involve the testes include granulomatosis with polyangiitis (Wegener's), Henoch-Schonlein purpura, giant cell arteritis and various autoimmune connective tissue disorders such as systemic lupus erythematosis (J Urol 2006;176:2682).
Testicular vasculitis can present with acute onset of pain and swelling, presumably related to intratesticular hemorrhage (Ir Med J 2006;99:27). Systemic disease is frequently already present at the time of initial presentation of testicular vasculitis or develops shortly thereafter. Some cases, however, remain isolated to the testes with no evidence of progression to systemic disease (J Clin Pathol 1994;47:1121). It is, therefore, unclear whether isolated testicular vasculitis represents an early site of involvement by systemic disease or a separate entity (World J Surg Oncol 2011;9:63). Only several cases of isolated testicular vasculitis were reported in the literature and a presentation suggestive of a testicular neoplasm is even less common (J Clin Pathol 1994;47:1121). Since testicular biopsy is contraindicated when malignancy is suspected, the diagnosis is usually reported postorchiectomy in these cases (ScientificWorldJournal 2010;10:1915, Urology 2003;61:1035).
Treatment options are still debated and frequently hinge on individual factors which need to be carefully considered in each patient. Immunosuppressive therapy has been administered to some of the patients. In other cases, careful follow up to exclude progression to systemic disease was preferred (J Clin Pathol 1994;47:1121). Some authors have even postulated that the excision of the affected organ might be curative, obviating the need for pharmacologic therapy (ScientificWorldJournal 2010;10:1915). Close follow up, including serology, is recommended since the risk of progression to systemic disease is unknown (J Clin Pathol 1994;47:1121).
Although uncommon, isolated necrotizing testicular vasculitis remains in the differential diagnosis of hypovascular testicular lesions. Long term follow up and additional research is needed in order to further elucidate the pathogenesis of isolated organ vasculitis and the subsequent risk of disease progression.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Oana Rafael, Lenox Hill Hospital, New York (USA), for contributing this case and discussion.

- Do you use Amazon.com? You can support our free website just by making an Amazon purchase, IF you enter Amazon through a banner or link on our website (above) or by clicking here. Amazon uses third parties to market their website and pays out of the money they receive - it doesn't cost you anything extra.
- Heptinstall's Pathology of the Kidney, 7th Edition by J. Charles Jennette, Vivette D'Agati, Jean Olson and Fred Silva is the right book if you're looking to deepen your understanding of kidney disease. Authored by the world's most accomplished renal pathologists, this image-rich text conveys the intricacies and comprehensiveness of renal disease, offering powerful diagnostic and treatment recommendations from decades of clinical research. Stay up to date on the cutting edge of kidney research and treatment and offer your patients the best therapeutic options and preventative measures available today.
For more information, visit our Books page.
Website news:
(1) Looking to print a page off our website? Use PrintFriendly.com! It is a free, easy to use website that allows you make any web page print friendly.
Remember if you want to search for a topic on our website, use the Google search bar at the top of our Home page. Also, the 'cached' feature can still be found by using the Google search bar on the bottom of our Home Page.
(2) We have decided to slightly change our policy, to post only 3 cases of the week per calendar year per contributor. You may still send cases at any time but we will only post 3 per year. This is based on posting cases in the manner we usually do - unfortunately, we cannot switch around the order of cases for your benefit. Thank you for your contributions to PathologyOutlines.com!
(3) PathologyOutlines.com is the major sponsor of The Detroit College Promise (DCP), a tax-exempt nonprofit which provides scholarships for Detroit Public School students. DCP is part of an online fundraising challenge, with the potential to receive an additional $10,000 to $50,000 for raising the most funds. If you value PathologyOutlines.com and feel charitable, please consider donating to this campaign. Please click here to donate.
(4) We broke another website traffic record with 28,022 visits on September 18, 2014. We keep improving so you will keep coming back. Thank you!
Visit and follow our Blog to see recent updates to the website.
(1) Looking to print a page off our website? Use PrintFriendly.com! It is a free, easy to use website that allows you make any web page print friendly.
Remember if you want to search for a topic on our website, use the Google search bar at the top of our Home page. Also, the 'cached' feature can still be found by using the Google search bar on the bottom of our Home Page.
(2) We have decided to slightly change our policy, to post only 3 cases of the week per calendar year per contributor. You may still send cases at any time but we will only post 3 per year. This is based on posting cases in the manner we usually do - unfortunately, we cannot switch around the order of cases for your benefit. Thank you for your contributions to PathologyOutlines.com!
(3) PathologyOutlines.com is the major sponsor of The Detroit College Promise (DCP), a tax-exempt nonprofit which provides scholarships for Detroit Public School students. DCP is part of an online fundraising challenge, with the potential to receive an additional $10,000 to $50,000 for raising the most funds. If you value PathologyOutlines.com and feel charitable, please consider donating to this campaign. Please click here to donate.
(4) We broke another website traffic record with 28,022 visits on September 18, 2014. We keep improving so you will keep coming back. Thank you!
Visit and follow our Blog to see recent updates to the website.
Case #328
Clinical history:
A 34 year old man had gradually increasing abdominal and left scrotal pain. Scrotal ultrasound demonstrated a left testicular heterogeneous hypoechoic lesion with no significant internal vascularity (figures 1, 2). Radical orchiectomy was performed.
The testis was bivalved to show a hemorrhagic, well defined, soft, dark red lesion (figure 3).
Scrotal ultrasound:
Gross images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Testicular necrotizing vasculitis
Discussion:
Microscopic examination of the lesion revealed focal hemorrhage with early organization and small arteries around the area of hemorrhage showing necrotizing vasculitis.
Necrotizing vasculitis is a systemic disease which manifests as inflammation of arteries with fibrinoid necrosis and fibrosis of the vascular wall. It can be associated with a variety of other entities or may be idiopathic (Cardiovascular Pathology 1994;3:197). While necrotizing vasculitis can involve any organ, isolated testicular involvement is rare and can pose diagnostic difficulties, especially in the absence of clinical and laboratory evidence of systemic involvement (World J Surg Oncol 2011;9:63).
Polyarteritis nodosa (PAN) is the most common form of testicular vasculitis, predominantly seen in the fourth to sixth decades of life. It is often associated with hepatitis B virus and human immunodeficiency virus. Although 60% to 86% of patients with PAN show testicular involvement at autopsy (ScientificWorldJournal 2010;10:1915), testicular symptoms are present in < 20% of patients (Hum Pathol 1988;19:186). Other vasculitides that may involve the testes include granulomatosis with polyangiitis (Wegener's), Henoch-Schonlein purpura, giant cell arteritis and various autoimmune connective tissue disorders such as systemic lupus erythematosis (J Urol 2006;176:2682).
Testicular vasculitis can present with acute onset of pain and swelling, presumably related to intratesticular hemorrhage (Ir Med J 2006;99:27). Systemic disease is frequently already present at the time of initial presentation of testicular vasculitis or develops shortly thereafter. Some cases, however, remain isolated to the testes with no evidence of progression to systemic disease (J Clin Pathol 1994;47:1121). It is, therefore, unclear whether isolated testicular vasculitis represents an early site of involvement by systemic disease or a separate entity (World J Surg Oncol 2011;9:63). Only several cases of isolated testicular vasculitis were reported in the literature and a presentation suggestive of a testicular neoplasm is even less common (J Clin Pathol 1994;47:1121). Since testicular biopsy is contraindicated when malignancy is suspected, the diagnosis is usually reported postorchiectomy in these cases (ScientificWorldJournal 2010;10:1915, Urology 2003;61:1035).
Treatment options are still debated and frequently hinge on individual factors which need to be carefully considered in each patient. Immunosuppressive therapy has been administered to some of the patients. In other cases, careful follow up to exclude progression to systemic disease was preferred (J Clin Pathol 1994;47:1121). Some authors have even postulated that the excision of the affected organ might be curative, obviating the need for pharmacologic therapy (ScientificWorldJournal 2010;10:1915). Close follow up, including serology, is recommended since the risk of progression to systemic disease is unknown (J Clin Pathol 1994;47:1121).
Although uncommon, isolated necrotizing testicular vasculitis remains in the differential diagnosis of hypovascular testicular lesions. Long term follow up and additional research is needed in order to further elucidate the pathogenesis of isolated organ vasculitis and the subsequent risk of disease progression.