24 September 2014 - Case #327
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jamie Shutter, Women's Care Florida Laboratory (USA), for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Advertisement
Case #327
Clinical history:
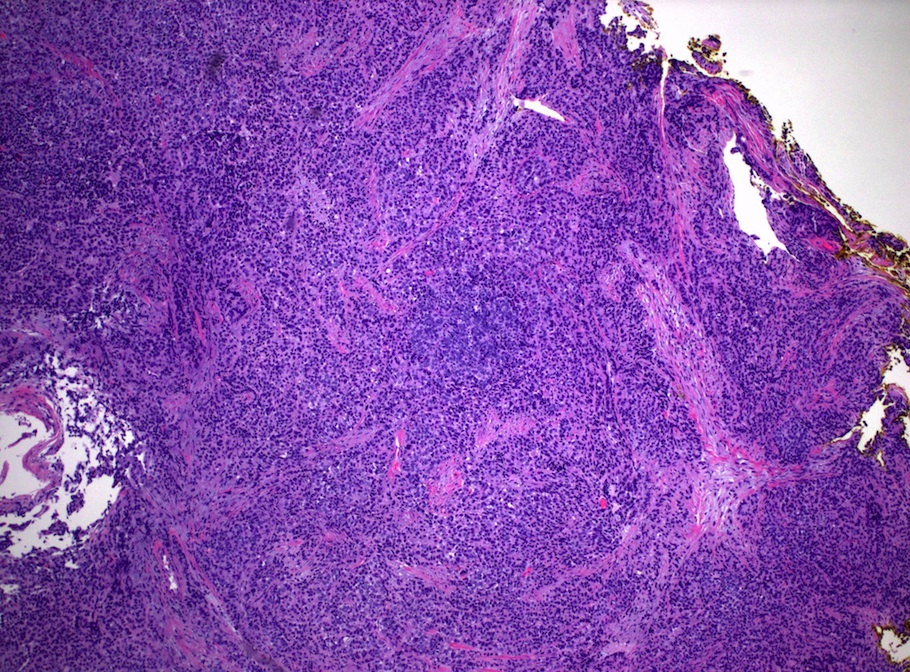
A 27 year old woman had a 6 cm cervical mass, which was biopsied. The outside diagnosis was poorly differentiated carcinoma, suggestive of adenocarcinoma.
Microscopic images:
What is your diagnosis?
Diagnosis: Neuroendocrine carcinoma of the cervix, small cell type
Immunostain images:
Discussion:
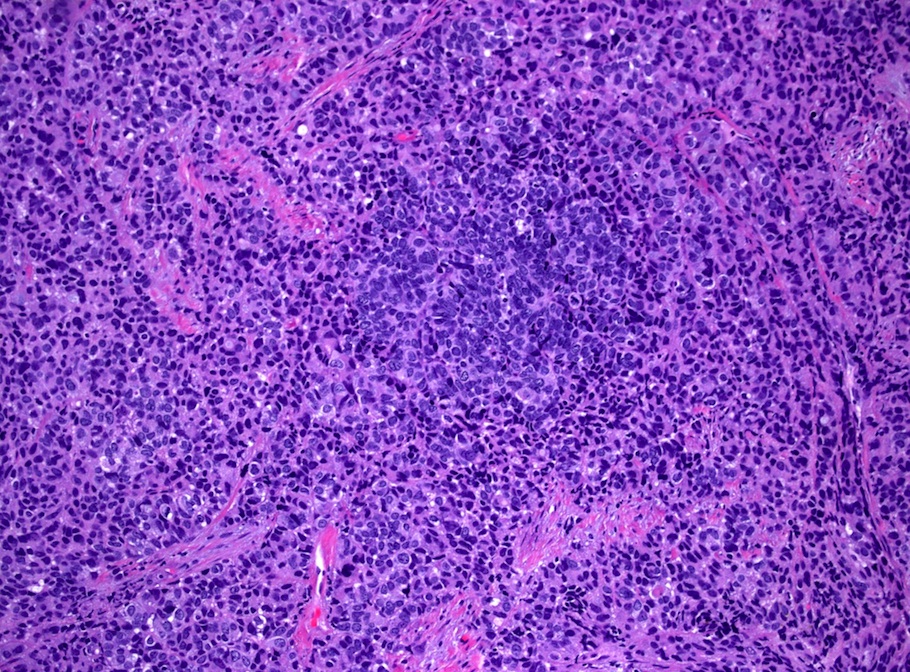
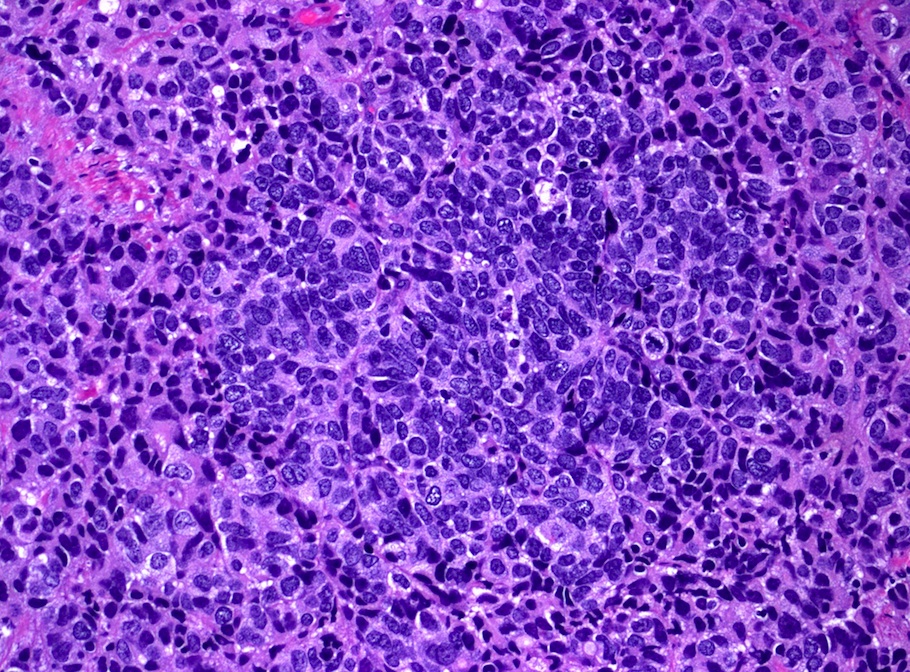
The biopsy shows a poorly differentiated carcinoma with neuroendocrine histology, including a vague ribbon pattern and salt and pepper chromatin. There is hyperchromasia and nuclear molding, as well as conspicuous apoptosis and mitotes. Immunohistochemistry also confirmed the tumor's neuroendocrine features:
Additional immunostain results were focal p63 staining and negative staining for HMB45, LCA / CD45, CK20, NSE, polyclonal CEA, vimentin and p53. The morphologic features and positive (albeit not strong) neuroendocrine immunostains are most consistent with a poorly differentiated malignancy, namely small cell neuroendocrine carcinoma. The clinical presentation and the overexpression of p16 (acting as surrogate of HPV infection) are most in keeping with a primary cervical origin.
Cervical neuroendocrine carcinomas, whether small cell or large cell type, are aggressive tumors with rapid metastases. They are frequently treated with a combination of chemotherapy and radiation, so the initial biopsy may be the only time to get diagnostic tissue.
The differential diagnosis includes:
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jamie Shutter, Women's Care Florida Laboratory (USA), for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Advertisement
Website news:
(1) PathologyOutlines.com is the major sponsor of The Detroit College Promise (DCP), a tax-exempt nonprofit which provides scholarships for Detroit Public School students. DCP is part of an online fundraising challenge, with the potential to receive an additional $10,000 to $50,000 for raising the most funds. If you value PathologyOutlines.com, and feel charitable, please consider donating to this campaign. If you donate at least $25, you will automatically be signed up to win one of four $500 Moosejaw gift cards, and can also feel good about helping make the world a better place.
(2) We broke another website traffic record with 28,022 visits on September 18, 2014. We keep improving so you will keep coming back. Thank you!
(3) Do you use Amazon.com? You can support our free website just by making an Amazon purchase if you enter Amazon through a banner or link on our website, or by clicking here. Amazon uses third parties to market their website, and pays out of the money they receive - it doesn't cost you anything extra. Thanks!
(4) We enjoy seeing and talking with the pathology community at the conferences we attend, and CAP '14 is no different. Thanks again to everyone who stopped by. Pictures are available on our Facebook page.
Visit and follow our Blog to see recent updates to the website.
(1) PathologyOutlines.com is the major sponsor of The Detroit College Promise (DCP), a tax-exempt nonprofit which provides scholarships for Detroit Public School students. DCP is part of an online fundraising challenge, with the potential to receive an additional $10,000 to $50,000 for raising the most funds. If you value PathologyOutlines.com, and feel charitable, please consider donating to this campaign. If you donate at least $25, you will automatically be signed up to win one of four $500 Moosejaw gift cards, and can also feel good about helping make the world a better place.
(2) We broke another website traffic record with 28,022 visits on September 18, 2014. We keep improving so you will keep coming back. Thank you!
(3) Do you use Amazon.com? You can support our free website just by making an Amazon purchase if you enter Amazon through a banner or link on our website, or by clicking here. Amazon uses third parties to market their website, and pays out of the money they receive - it doesn't cost you anything extra. Thanks!
(4) We enjoy seeing and talking with the pathology community at the conferences we attend, and CAP '14 is no different. Thanks again to everyone who stopped by. Pictures are available on our Facebook page.
Visit and follow our Blog to see recent updates to the website.
Case #327
Clinical history:
A 27 year old woman had a 6 cm cervical mass, which was biopsied. The outside diagnosis was poorly differentiated carcinoma, suggestive of adenocarcinoma.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Neuroendocrine carcinoma of the cervix, small cell type
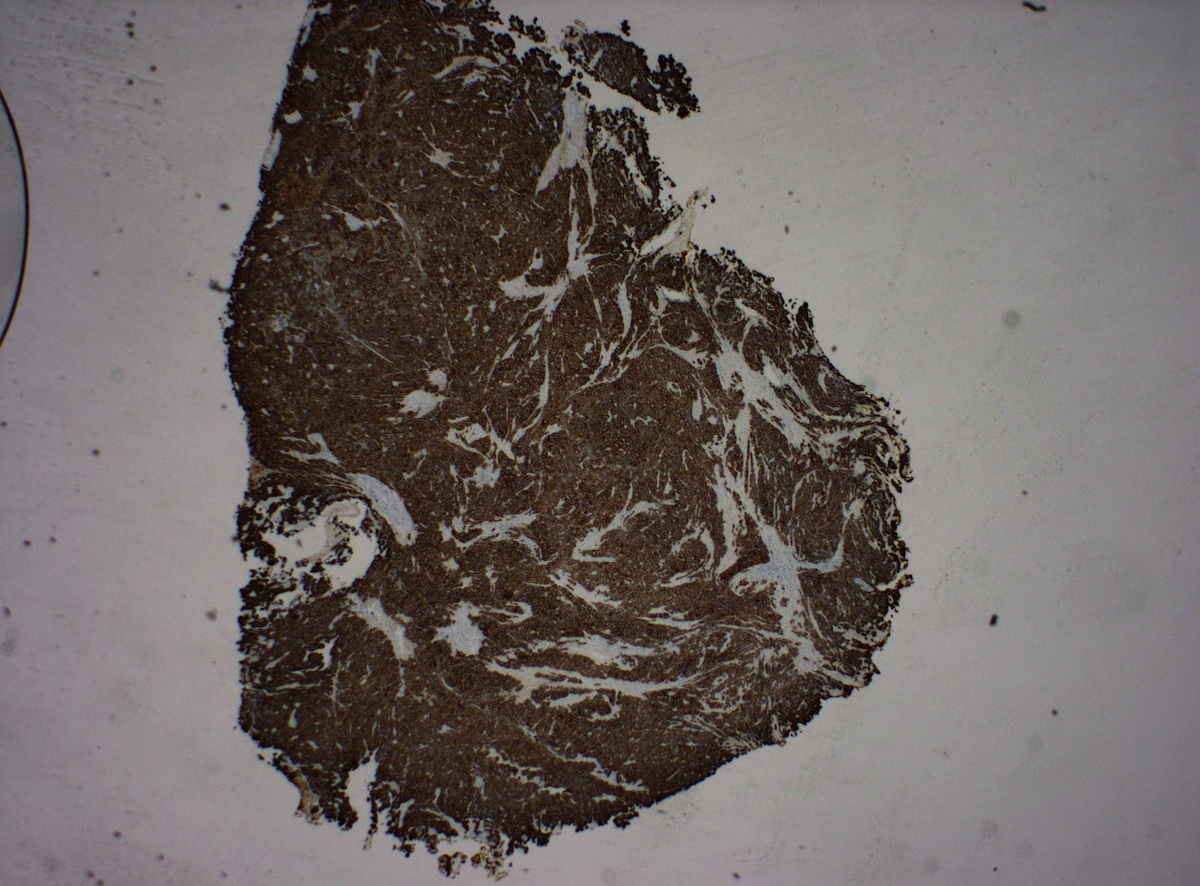
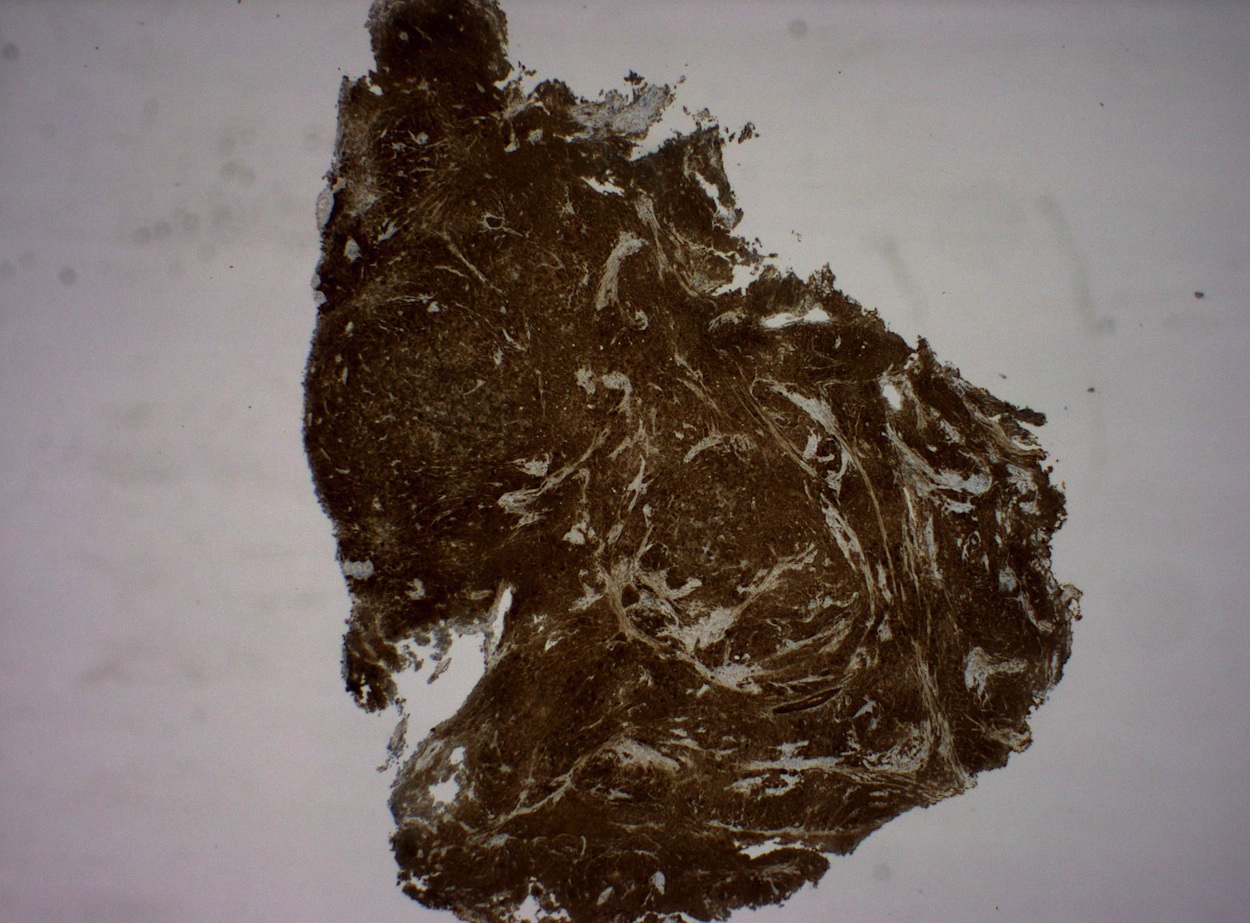
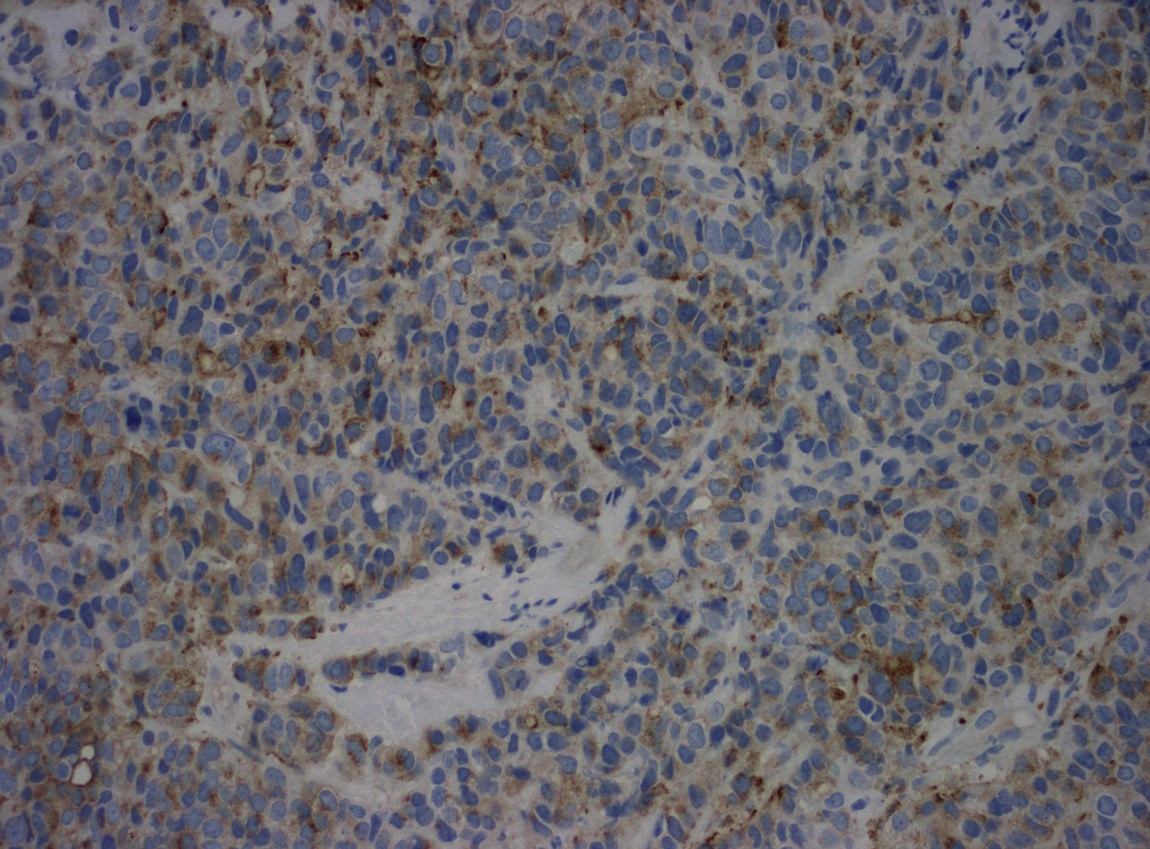
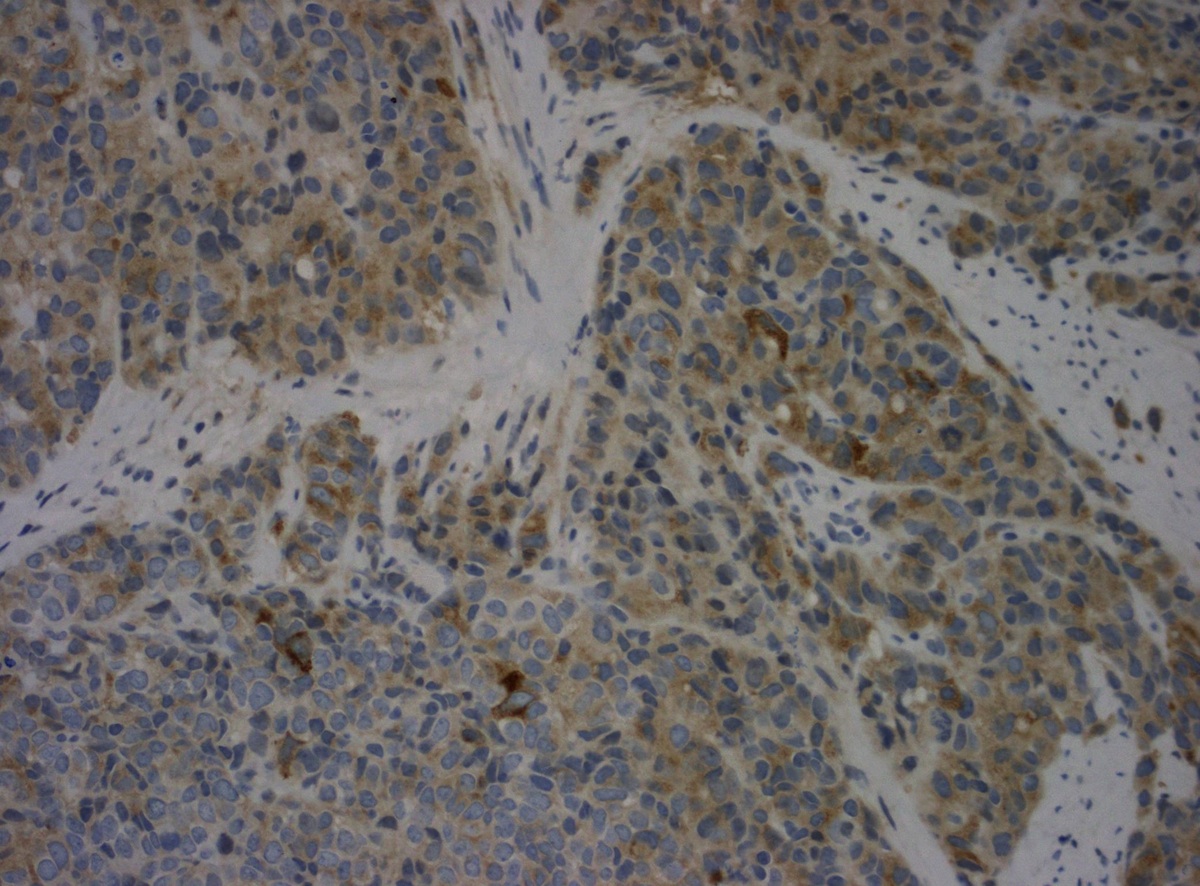
Immunostain images:
CK7
p16
Chromogranin
Synaptophysin
Discussion:
The biopsy shows a poorly differentiated carcinoma with neuroendocrine histology, including a vague ribbon pattern and salt and pepper chromatin. There is hyperchromasia and nuclear molding, as well as conspicuous apoptosis and mitotes. Immunohistochemistry also confirmed the tumor's neuroendocrine features:
Additional immunostain results were focal p63 staining and negative staining for HMB45, LCA / CD45, CK20, NSE, polyclonal CEA, vimentin and p53. The morphologic features and positive (albeit not strong) neuroendocrine immunostains are most consistent with a poorly differentiated malignancy, namely small cell neuroendocrine carcinoma. The clinical presentation and the overexpression of p16 (acting as surrogate of HPV infection) are most in keeping with a primary cervical origin.
Cervical neuroendocrine carcinomas, whether small cell or large cell type, are aggressive tumors with rapid metastases. They are frequently treated with a combination of chemotherapy and radiation, so the initial biopsy may be the only time to get diagnostic tissue.
The differential diagnosis includes:
- Metastatic neuroendocrine carcinoma from the lung or another primary site:
- Clinical history, negative p16 / HPV molecular studies
- Carcinoid tumor:
- Distinct architecture with insular, trabecular, tubular morphology and absence of high grade cytomorphology
- Basaloid squamous cell carcinoma:
- Distinct nesting, absence of nuclear molding and brisk apoptosis / mitoses, strong p63 staining, no neuroendocrine features