4 June 2014 - Case #314
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Weiwei Chen, State University of New York (SUNY) at Buffalo (USA), for contributing this case.
Advertisement
Case #314
Clinical history:
A 68 year old woman presented with a history of CLL and papillary thyroid carcinoma. She was recently found to have progressively enlarging right inguinal lymph nodes. One of the lymph nodes was biopsied.
Microscopic images:
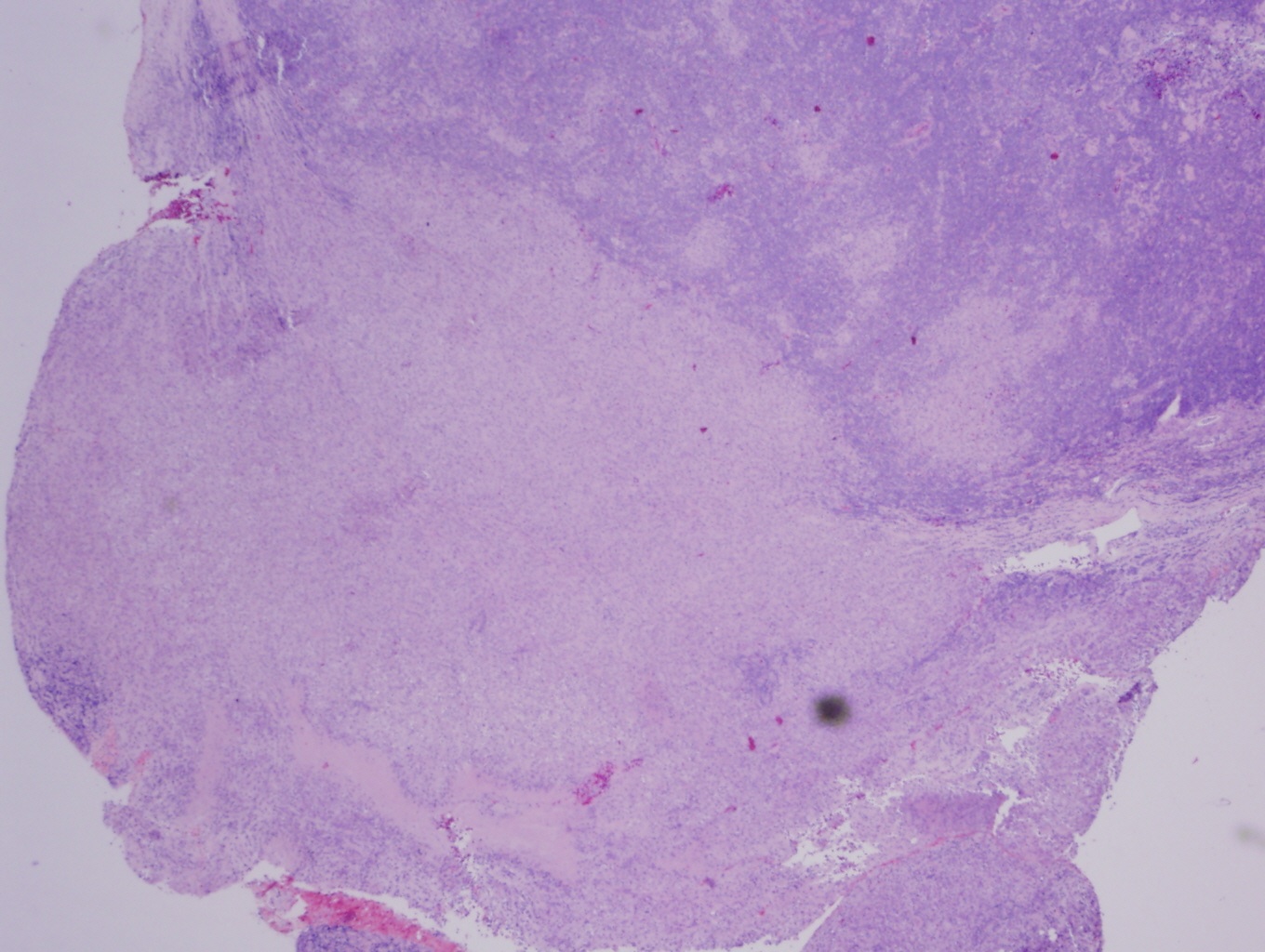
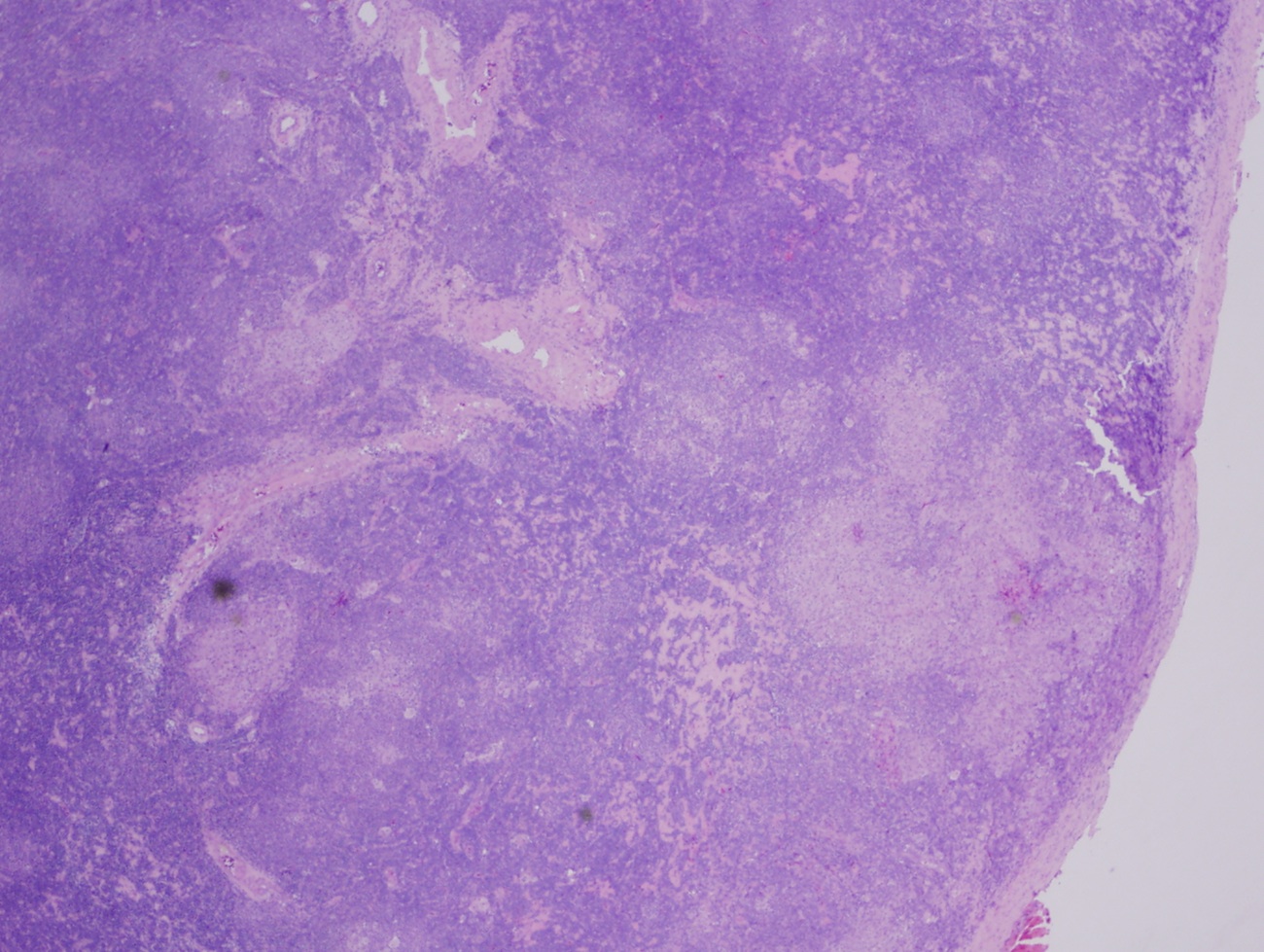
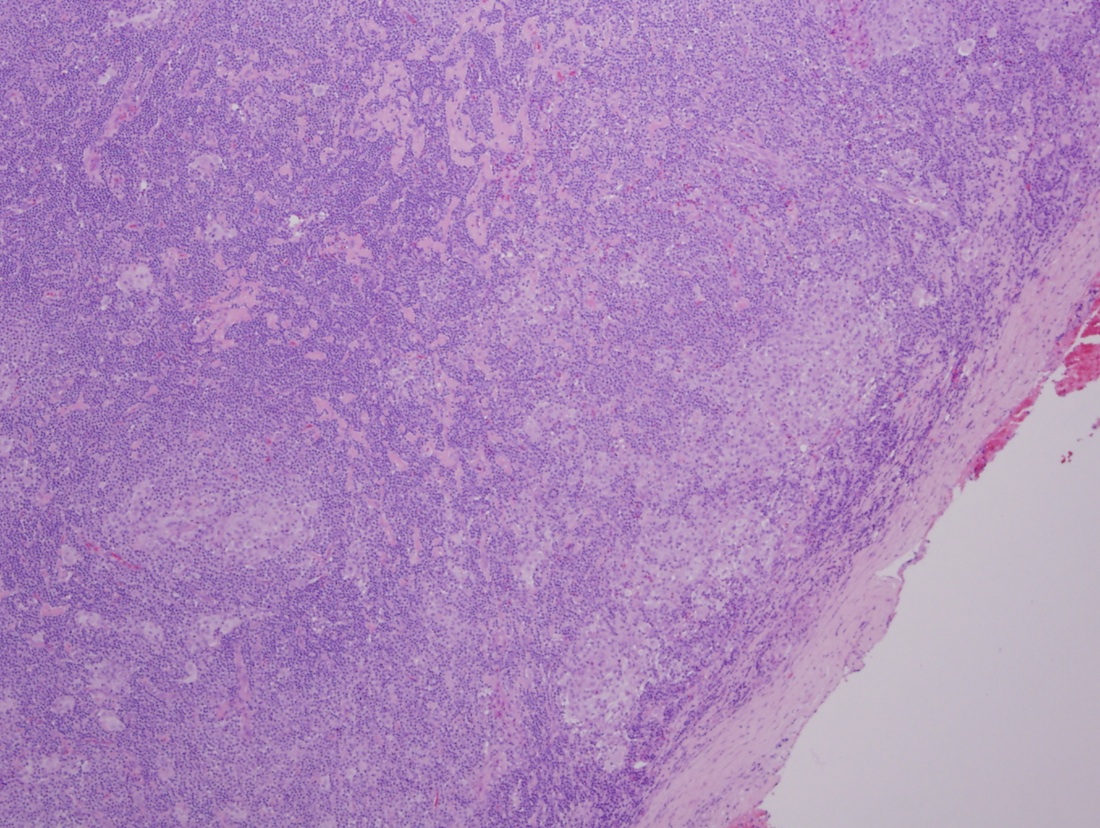
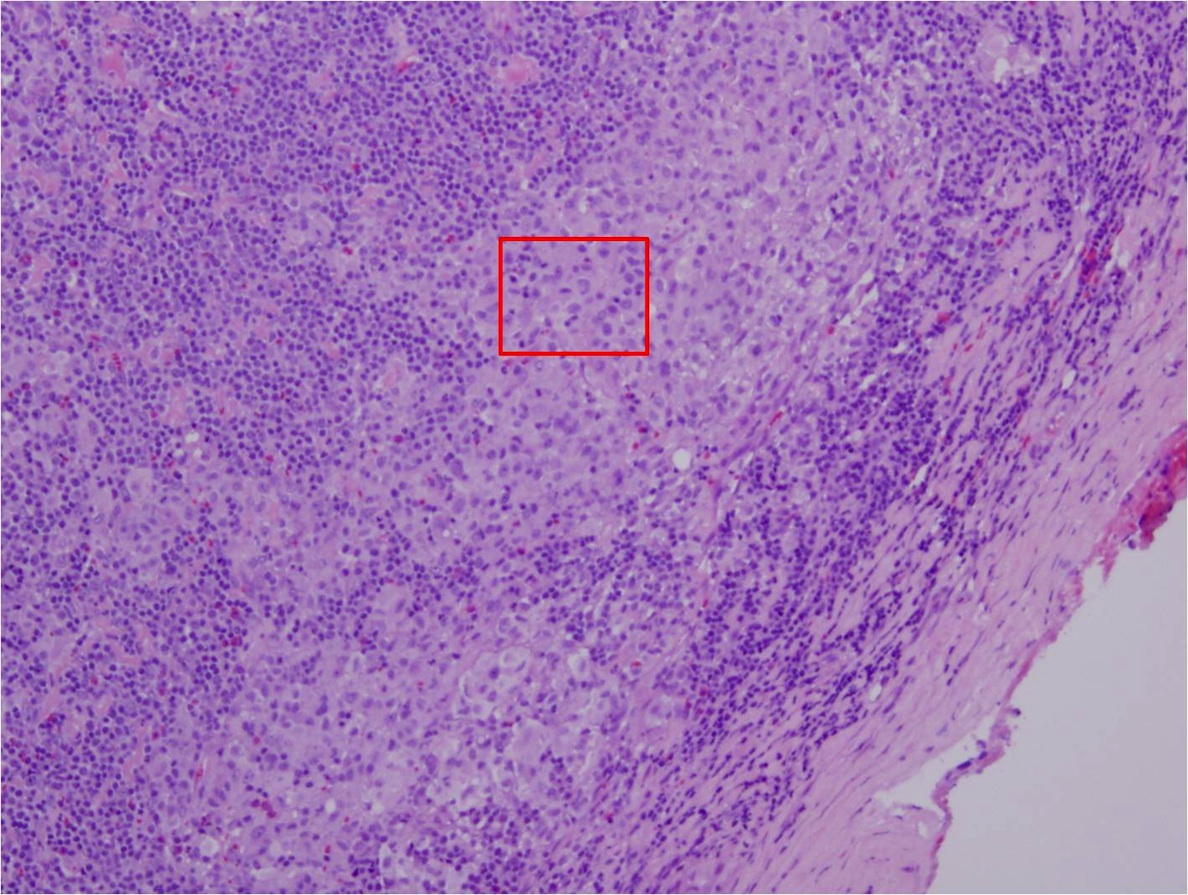
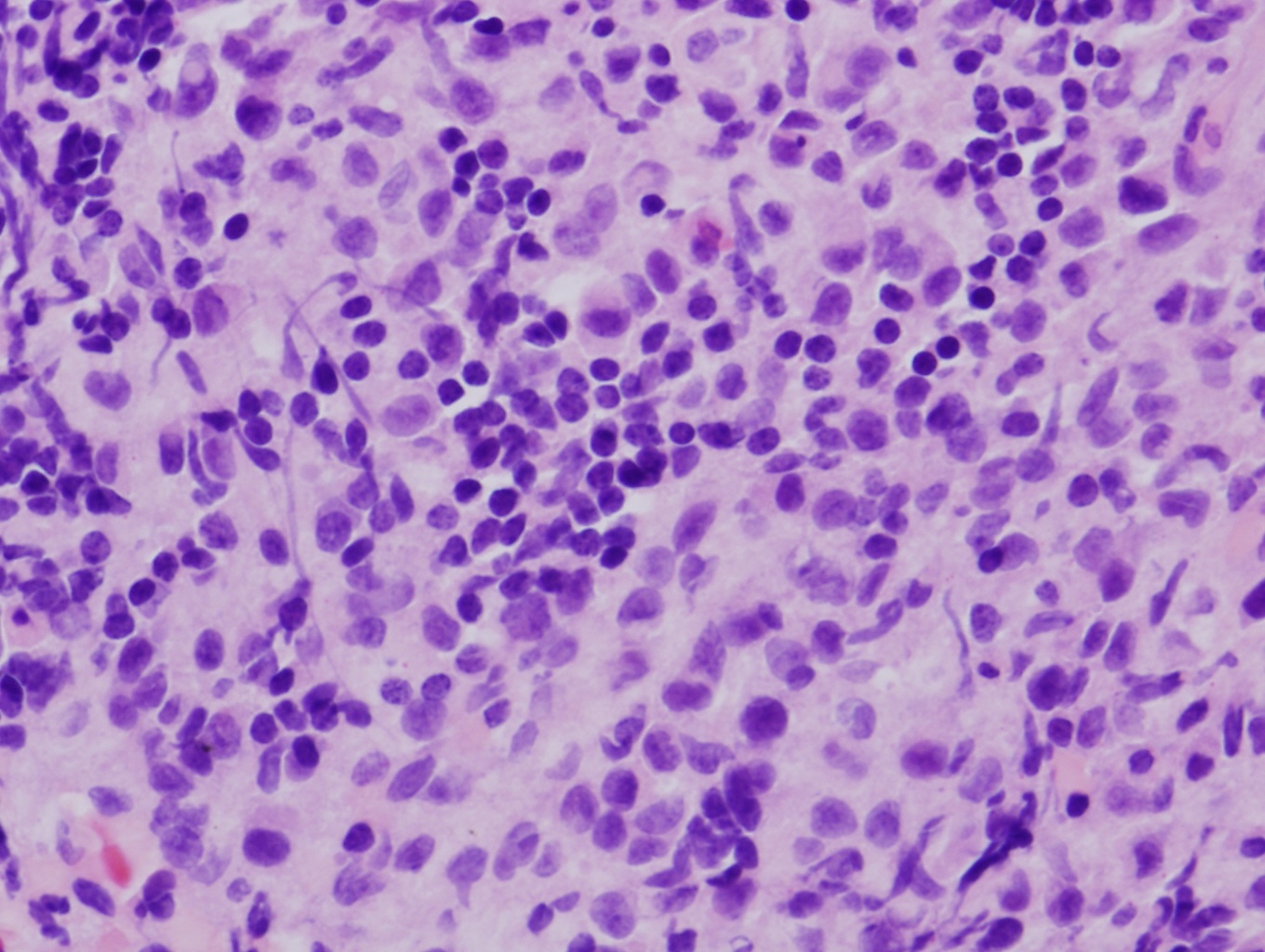
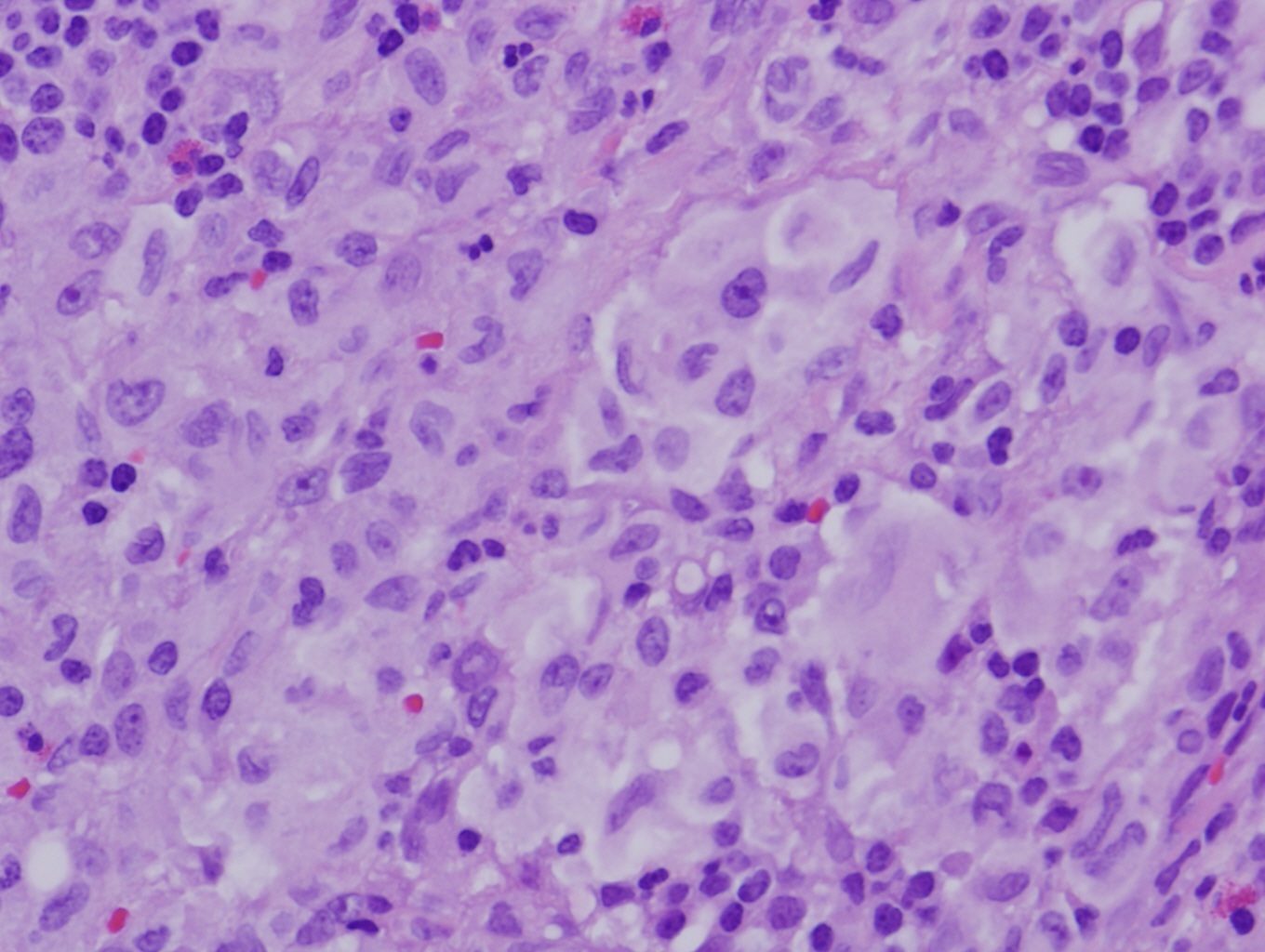

What is your diagnosis?
Diagnosis: Synchronous Langerhans cell sarcoma and small lymphocytic lymphoma / chronic lymphocytic leukemia
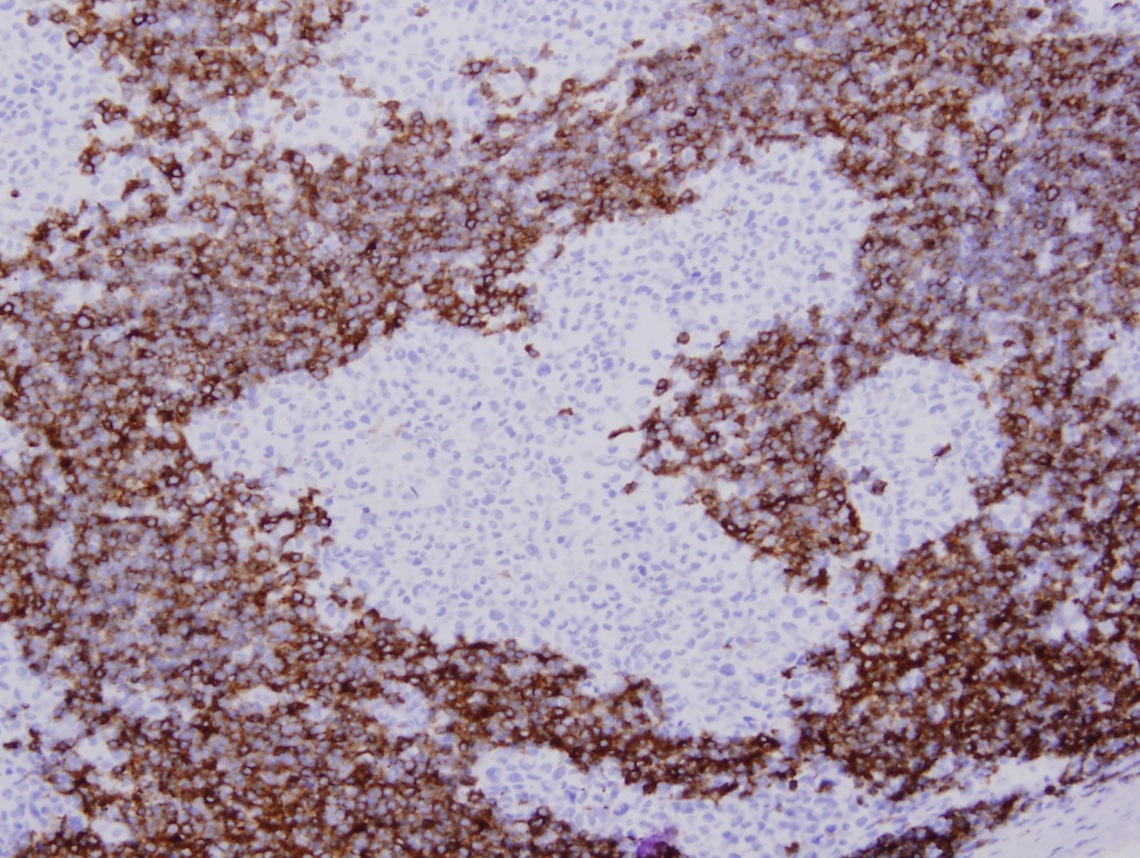
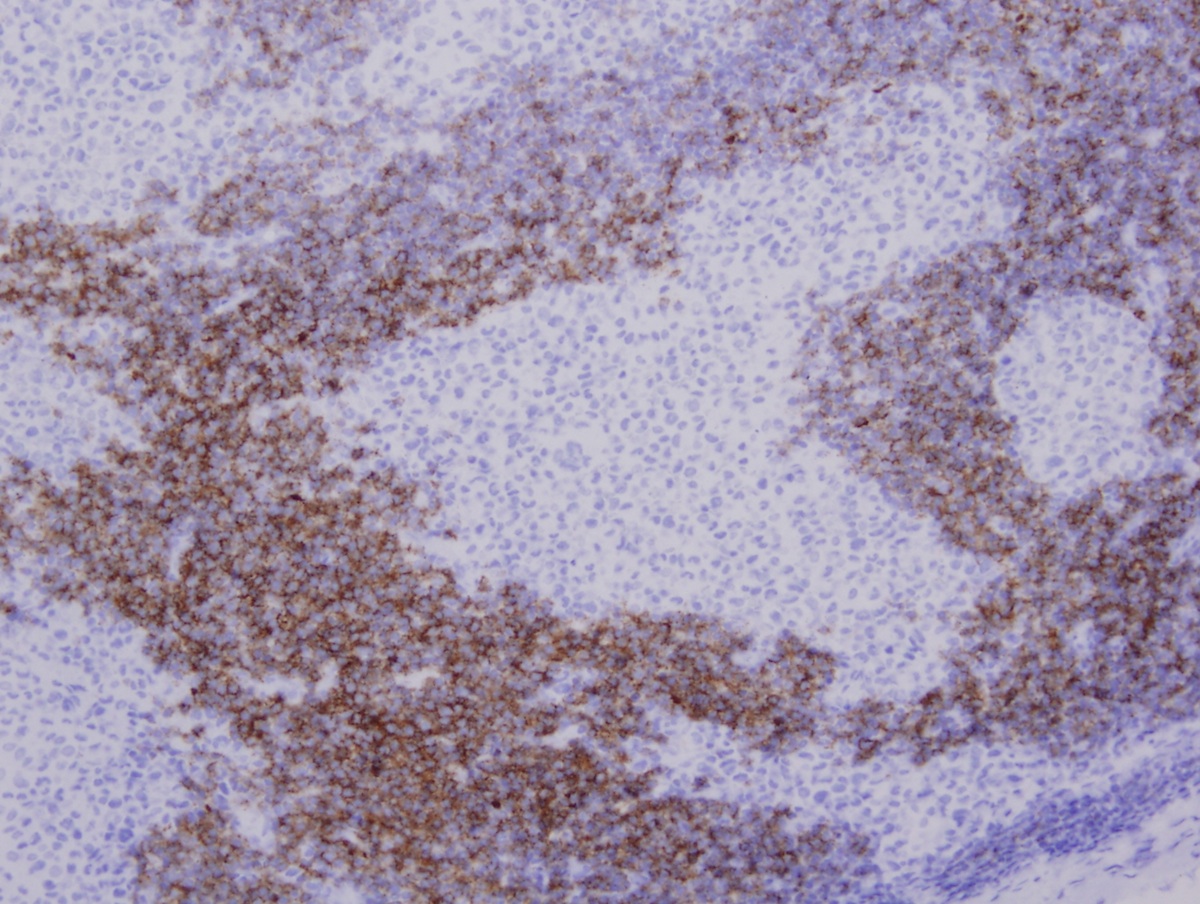
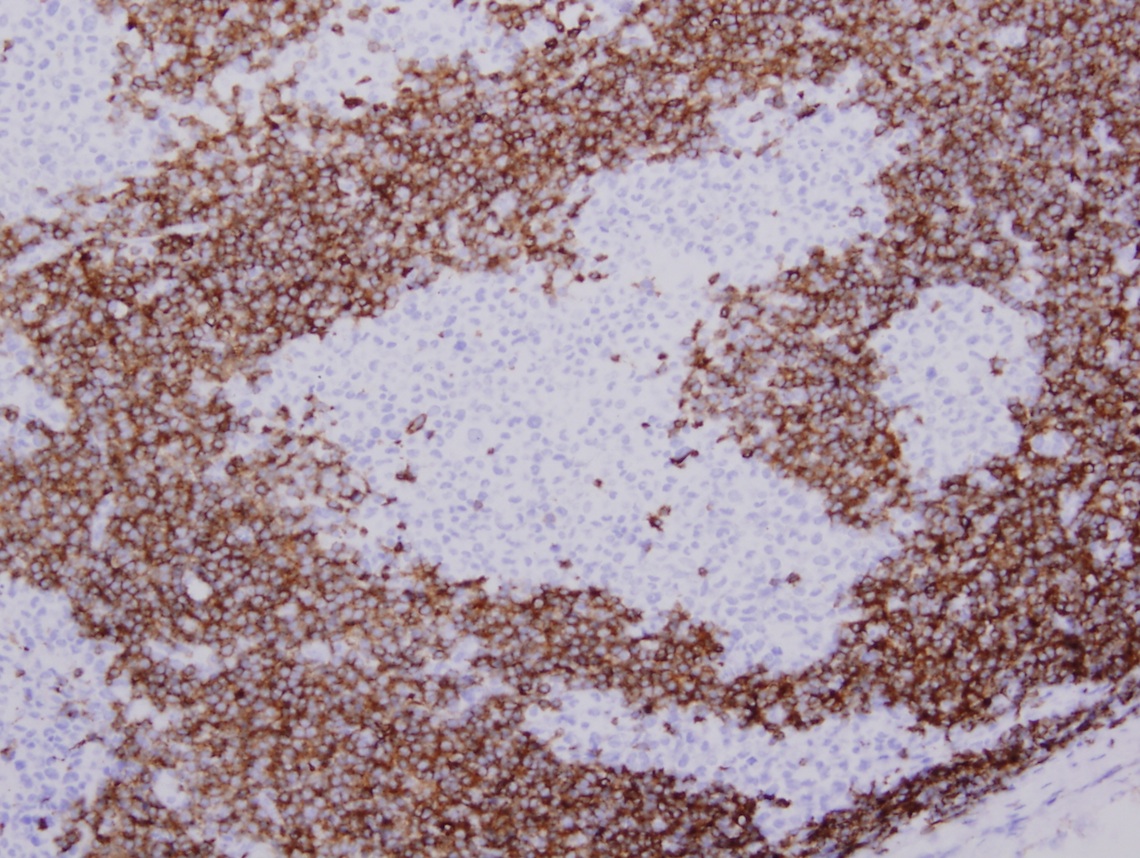
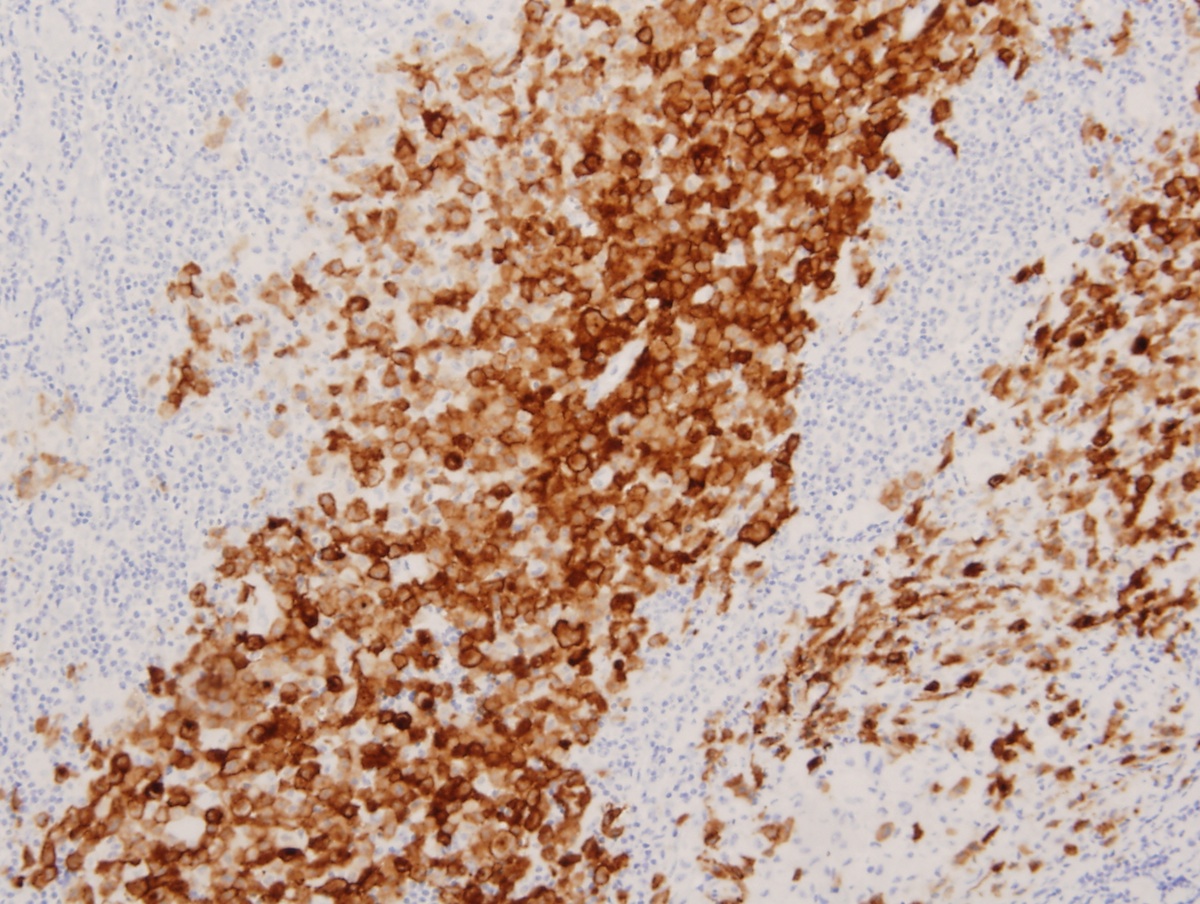
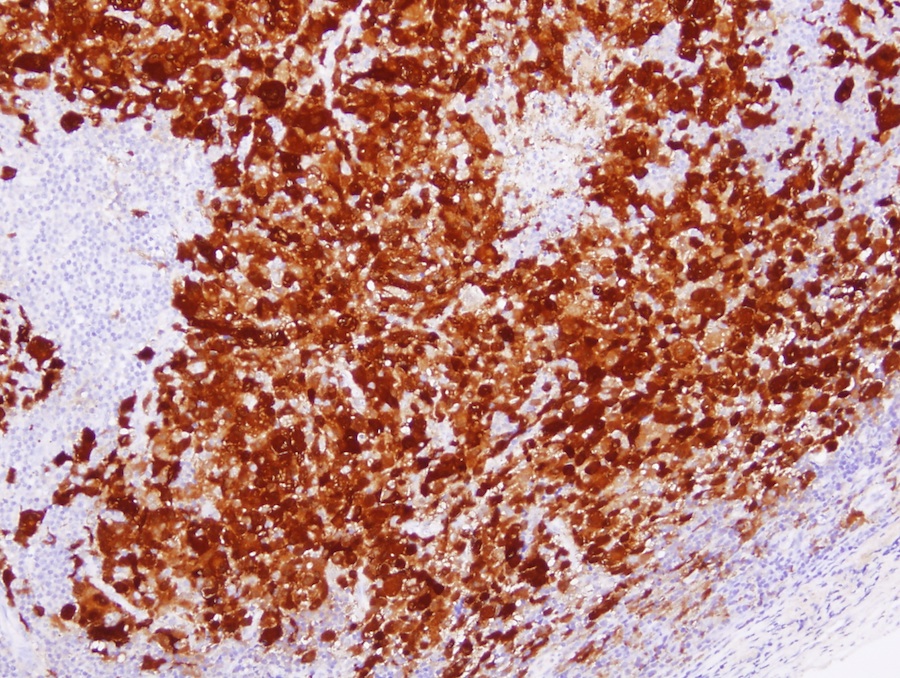
Immunostains:

Discussion:
Langerhans cell sarcoma is a rare tumor with markedly malignant cytological features that originates from Langerhans cells (IARC: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue, 4th Edition 2008). This case appears to be an example of transdifferentiation, first described by Jaffe et al. in which histiocytic / dendritic cell sarcomas may be transformed from lymphoproliferative diseases (N Am J Med Sci 2013;5:386, Blood 2008;111:5433, Am J Surg Pathol 2013;37:978). In this case, both the Langerhans cell sarcoma and CLL are clonally related, and contain the BRAF V600E mutation.
Langerhans cell sarcoma (LCS) is often an extranodal tumor with skin and bone involvement but it may present with multiorgan involvement including lymph node, lung, liver and spleen. As with Langerhans cell histiocytosis (LCH), it is a clonal proliferation of Langerhans cells, which are 12 - 15 microns in diameter with abundant, pale eosinophilic cytoplasm, irregular and elongated nuclei with prominent nuclear grooves and folds, fine chromatin and indistinct nucleoli. Langerhans cells are immunoreactive to CD1a, langerin and S100. However, LCS compared with LCH has more cytological atypia, a higher proliferation rate and a more aggressive clinical course (Diagn Pathol 2012;7:128).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Weiwei Chen, State University of New York (SUNY) at Buffalo (USA), for contributing this case.

Leica Biosystems is now offering 23 New Ready-to-Use Antibodies from Cell Marque designed to access protocols on the BOND platform.
Providing menu gap solutions with a "click-and-go" system for convenience and precision.
Website news:
(1) We have now posted the Pathology Jobs Report for the first quarter of 2014, available from the Jobs page or by clicking here. Learn what specialties are hot, and what employers are looking for.
Visit and follow our Blog to see recent updates to the website.
(1) We have now posted the Pathology Jobs Report for the first quarter of 2014, available from the Jobs page or by clicking here. Learn what specialties are hot, and what employers are looking for.
Visit and follow our Blog to see recent updates to the website.
Case #314
Clinical history:
A 68 year old woman presented with a history of CLL and papillary thyroid carcinoma. She was recently found to have progressively enlarging right inguinal lymph nodes. One of the lymph nodes was biopsied.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Synchronous Langerhans cell sarcoma and small lymphocytic lymphoma / chronic lymphocytic leukemia
Immunostains:
CD1a
CD5
CD20
CD23
Langerin
S100
Discussion:
Langerhans cell sarcoma is a rare tumor with markedly malignant cytological features that originates from Langerhans cells (IARC: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue, 4th Edition 2008). This case appears to be an example of transdifferentiation, first described by Jaffe et al. in which histiocytic / dendritic cell sarcomas may be transformed from lymphoproliferative diseases (N Am J Med Sci 2013;5:386, Blood 2008;111:5433, Am J Surg Pathol 2013;37:978). In this case, both the Langerhans cell sarcoma and CLL are clonally related, and contain the BRAF V600E mutation.
Langerhans cell sarcoma (LCS) is often an extranodal tumor with skin and bone involvement but it may present with multiorgan involvement including lymph node, lung, liver and spleen. As with Langerhans cell histiocytosis (LCH), it is a clonal proliferation of Langerhans cells, which are 12 - 15 microns in diameter with abundant, pale eosinophilic cytoplasm, irregular and elongated nuclei with prominent nuclear grooves and folds, fine chromatin and indistinct nucleoli. Langerhans cells are immunoreactive to CD1a, langerin and S100. However, LCS compared with LCH has more cytological atypia, a higher proliferation rate and a more aggressive clinical course (Diagn Pathol 2012;7:128).