2 April 2014 - Case #306
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Ahmed Lazim, Al-Jumhori Teaching Hospital, Mosul (Iraq), for contributing this case.
Case #306
Clinical history:
A 37 year old woman had a biopsy with an unspecified breast malignancy, and underwent a modified radical mastectomy.
Microscopic images:
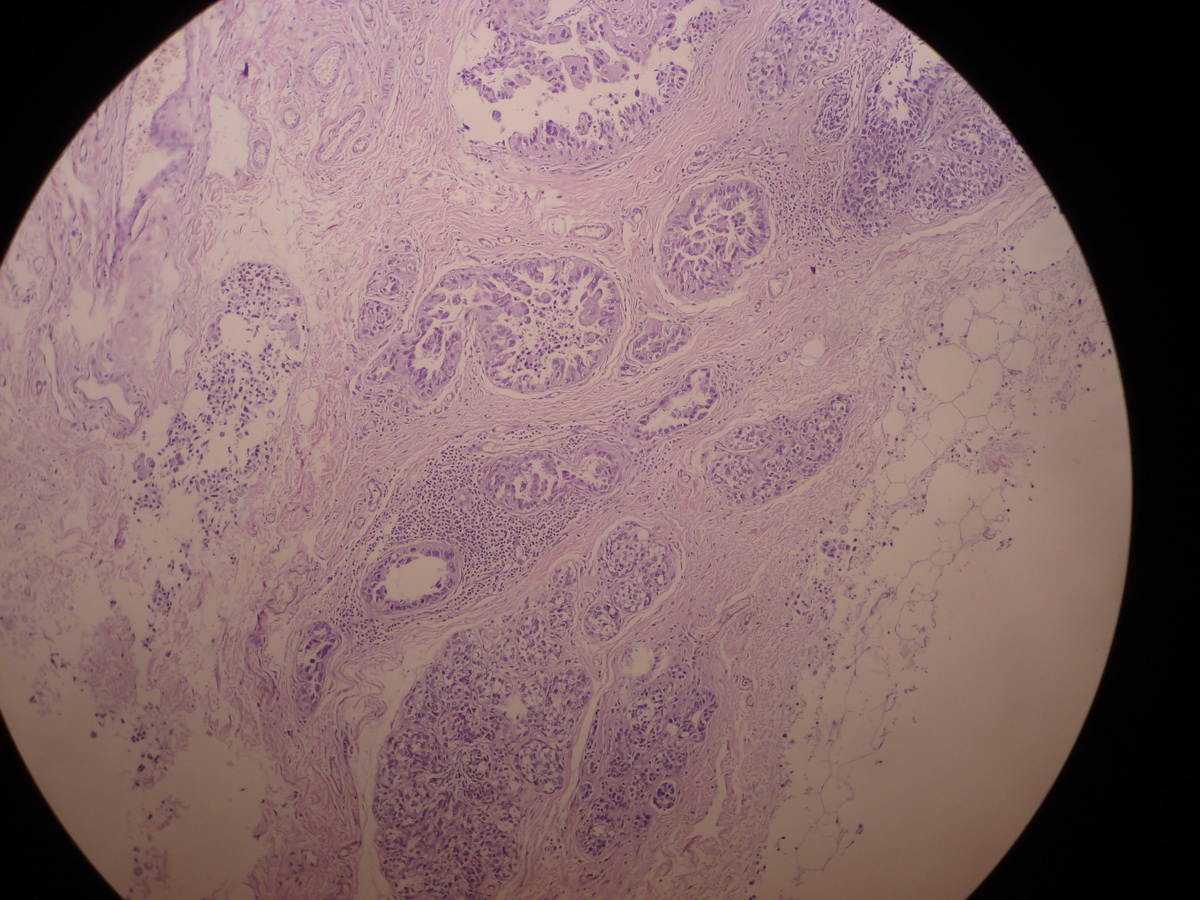
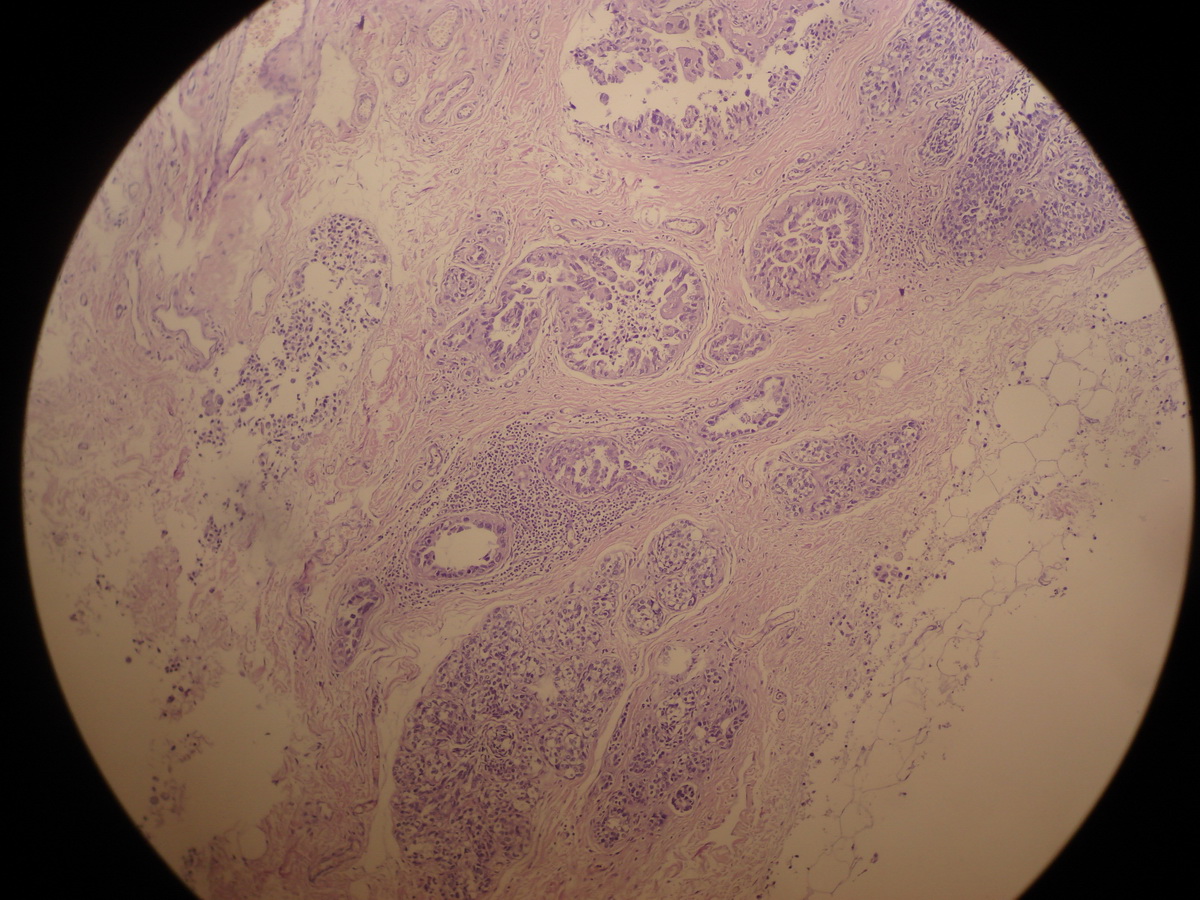

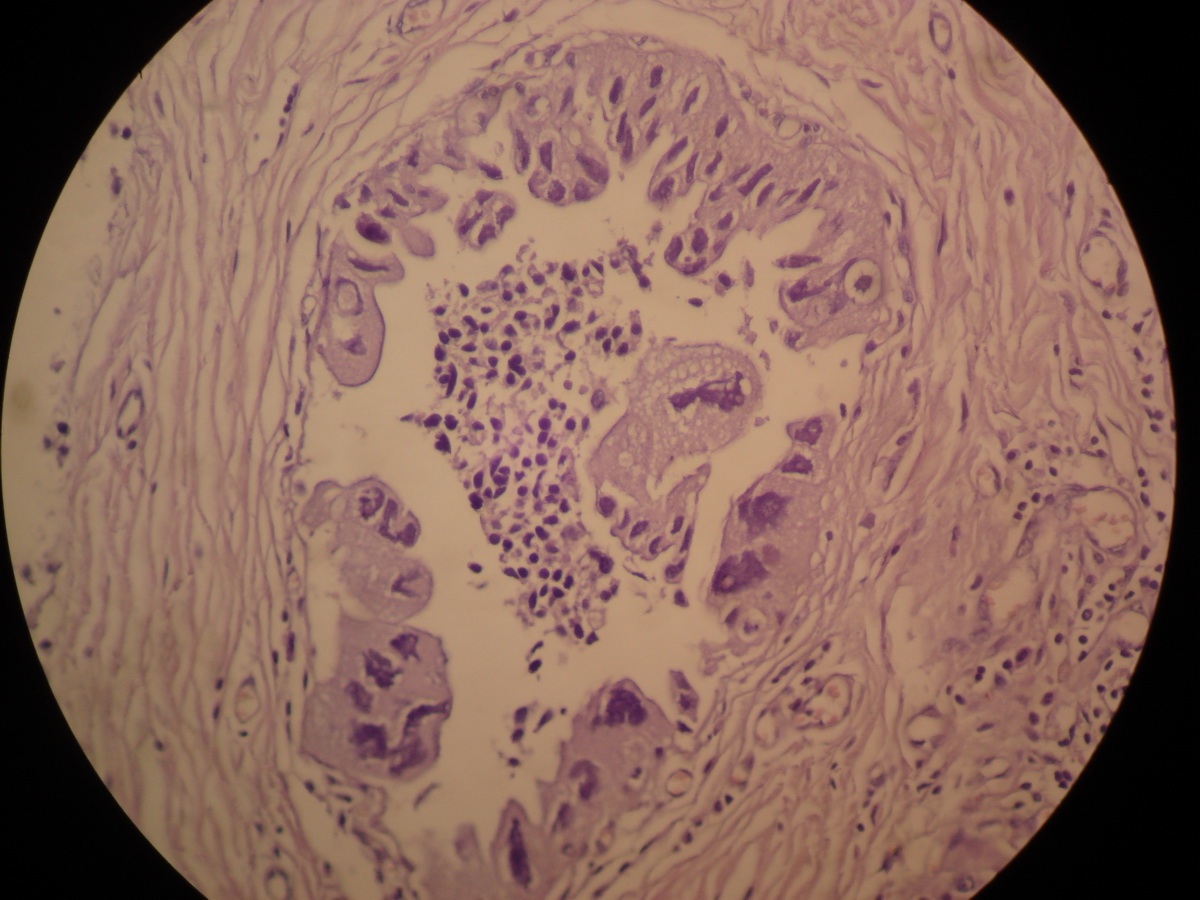
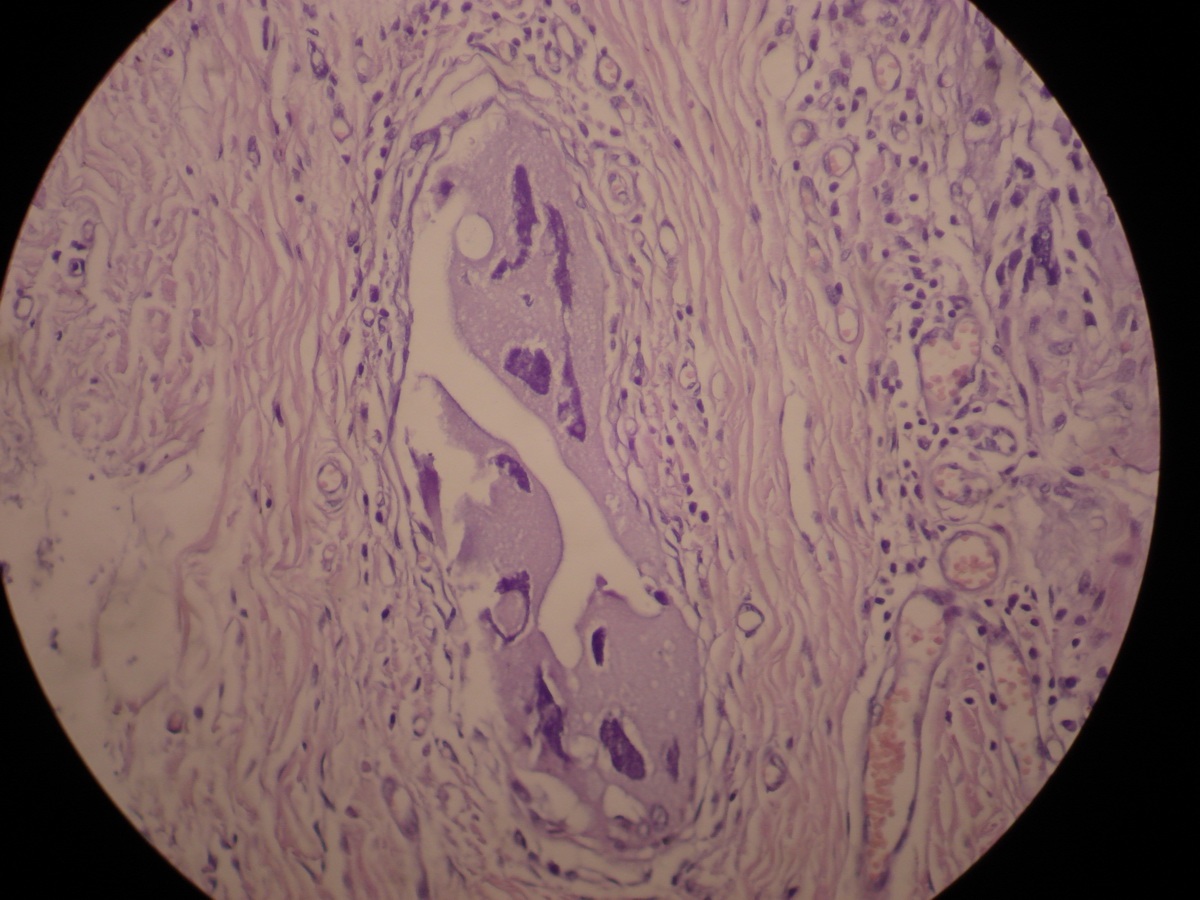

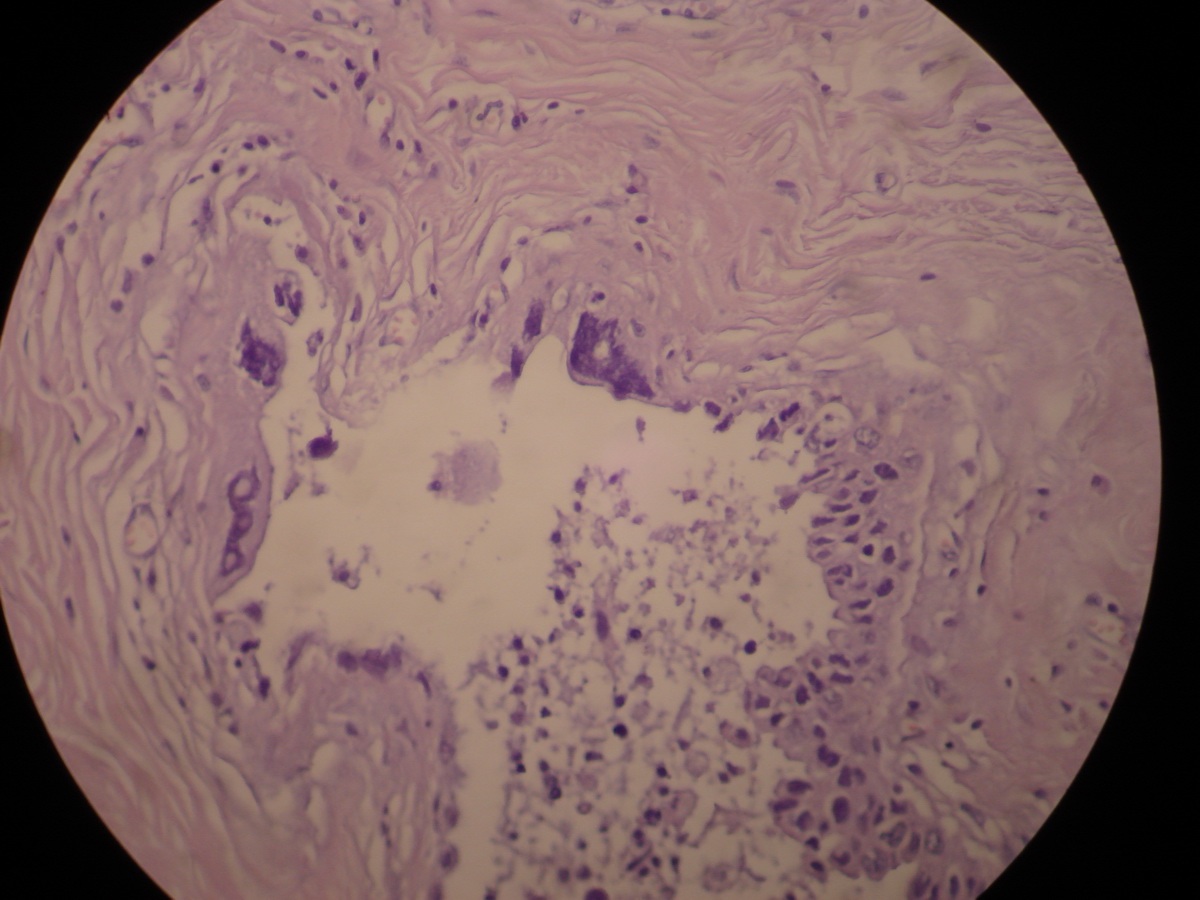
What is your diagnosis?
Diagnosis: Breast cancer with choriocarcinomatous differentiation (multicentric high grade invasive ductal carcinoma not otherwise specified with significant chroriocarcinomatous differentiation)
Discussion:
This rare tumor, with < 50 cases reported, was first described in 1981 (Am J Surg Pathol 1981;5:773). It is considered a variant of breast metaplastic carcinoma and has malignant cells resembling choriocarcinoma, with immunoreactivity for human placental lactogen and human chorionic gonadotropin. The histologic origin of the syncytiotrophoblast-like cells is unknown but they are thought to be a metaplastic process (Arch Pathol Lab Med 2011;135:1097).
Clinically, these tumors are part of a rapidly growing palpable mass indistinguishable from conventional breast carcinoma. Often, there is locally advanced disease. Microscopically, there are markedly pleomorphic, multinucleated choriocarcinomatous cells with abundant eosinophilic cytoplasm and occasional cytoplasmic vacuoles. There often is associated DCIS, invasive ductal carcinoma NOS (often moderately or poorly differentiated) or metaplastic carcinoma with heterologous components or sarcomatoid areas.
The differential diagnosis includes metastatic ovarian choriocarcinoma, which is usually not accompanied by usual type invasive ductal carcinoma or DCIS.
These tumors are usually aggressive, with a poor prognosis. Due to their rarity, an optimal therapeutic approach has not been identified.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Ahmed Lazim, Al-Jumhori Teaching Hospital, Mosul (Iraq), for contributing this case.
Website news:
(1) On March 26, 2014, we broke a daily record with 24,685 visits. For the month of March 2014, we had a monthly record of 586,057 visits, with a record average daily traffic of 18,905 visits. We will keep working hard to make PathologyOutlines.com an important and valuable part of your Pathology practice.
Visit and follow our Blog to see recent updates to the website.
(1) On March 26, 2014, we broke a daily record with 24,685 visits. For the month of March 2014, we had a monthly record of 586,057 visits, with a record average daily traffic of 18,905 visits. We will keep working hard to make PathologyOutlines.com an important and valuable part of your Pathology practice.
Visit and follow our Blog to see recent updates to the website.
Case #306
Clinical history:
A 37 year old woman had a biopsy with an unspecified breast malignancy, and underwent a modified radical mastectomy.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Breast cancer with choriocarcinomatous differentiation (multicentric high grade invasive ductal carcinoma not otherwise specified with significant chroriocarcinomatous differentiation)
Discussion:
This rare tumor, with < 50 cases reported, was first described in 1981 (Am J Surg Pathol 1981;5:773). It is considered a variant of breast metaplastic carcinoma and has malignant cells resembling choriocarcinoma, with immunoreactivity for human placental lactogen and human chorionic gonadotropin. The histologic origin of the syncytiotrophoblast-like cells is unknown but they are thought to be a metaplastic process (Arch Pathol Lab Med 2011;135:1097).
Clinically, these tumors are part of a rapidly growing palpable mass indistinguishable from conventional breast carcinoma. Often, there is locally advanced disease. Microscopically, there are markedly pleomorphic, multinucleated choriocarcinomatous cells with abundant eosinophilic cytoplasm and occasional cytoplasmic vacuoles. There often is associated DCIS, invasive ductal carcinoma NOS (often moderately or poorly differentiated) or metaplastic carcinoma with heterologous components or sarcomatoid areas.
The differential diagnosis includes metastatic ovarian choriocarcinoma, which is usually not accompanied by usual type invasive ductal carcinoma or DCIS.
These tumors are usually aggressive, with a poor prognosis. Due to their rarity, an optimal therapeutic approach has not been identified.