12 March 2014 - Case #303
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Raul Gonzalez, Vanderbilt University Medical Center, and Dr. Don Xu, University of California, San Diego, for contributing these cases.
Case #303
Case #1 (contributed by Dr. Raul Gonzalez)
A 50 year old man presented with upper GI bleeding and friable duodenal mucosa on endoscopy.



Case #2 (contributed by Dr. Don Xu)
A 47 year old man with a history of chronic arthralgias for 2 years presented with fevers, abdominal pain, and weight loss. He was found to have microcytic anemia and mesenteric and retroperitoneal lymphadenopathy. The pictures of duodenal biopsy are shown.

What is your diagnosis?
Diagnosis: Whipple's disease
Discussion:
Both cases showed blunted villi and expansion of the lamina propria by foamy histiocytes. Periodic acid Schiff (PAS) stain revealed numerous microorganisms within macrophages. In case #1, unstained slides were sent to an outside institution for Tropheryma whipplei immunostain, which was positive. In case #2, PCR study confirmed Tropheryma whipplei infection.
Whipple's disease is a rare systemic infection due to Tropheryma whippelii, a gram positive intracellular actinomycete, first described in 1907 by Dr. George Hoyt Whipple (World J Gastroenterol 2009;15:2078, Wikipedia: George Whipple [Accessed 25 March 2024]). Dr. Whipple won the Nobel Prize (jointly) in 1934 for another discovery, that liver given as food to dogs reversed the anemia, leading to treatment of pernicious anemia (The Noble Prize: George H. Whipple [Accessed 25 March 2024]). He was friends of Dr. Allen Whipple, a surgeon who described the Whipple procedure and the Whipple's triad of insulinoma (Wikipedia: Allen Whipple [Accessed 25 March 2024]).
Whipple's disease, also called intestinal lipodystrophy, typically affects white men ages 30 - 49 years, in the proximal intestine and mesenteric lymph nodes. Patients typically present with malabsorption (diarrhea, weight loss, abdominal pain), and occasionally polyarthritis, lymphadenopathy, hyperpigmentation and CNS complaints. Histology, in addition to the above features, shows dilated lymphatics or fat vacuoles. It may show multinucleated giant cells. EM shows rod-like organisms.
The differential diagnosis includes:
Treatment is with antibiotics, which must be continued for at least a year, or there is a high rate of relapse.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Raul Gonzalez, Vanderbilt University Medical Center, and Dr. Don Xu, University of California, San Diego, for contributing these cases.
Website news:
(1) Thanks to Baylor College of Medicine (who posted ad #4000) and the 3,999 other advertisers we've had since PathologyOutlines.com started in August 2001. For many years, pathologists were very skeptical about our website - how could it possibly be free? By now, most pathologists recognize that it is, in fact, a free, no registration website, paid for by advertising of pathology related jobs, conferences and fellowships. We also have advertising on our Home page, our Chapters, Management page, Case of the Week and other emails. We also have an affiliate relationship with Amazon, meaning that they pay us ~ 5% of the purchase price of anything bought on Amazon.com, if you enter Amazon through our website (by clicking on a link or banner). We also promote books of various publishers, and receive money when visitors click on Google ads. We do NOT allow popup ads, or other obnoxious ads. The free website model has worked very well for us.
(2) We have (finally) converted all 6,700+ topics on our website to topic format, with completion of the Eye chapter. The next big task is converting to a template based system that will also adapt to tablets and smart phones. This is (still) under development, but we hope to get it started soon.
(3) In February 2014, we again had record traffic, with a daily average of 18,323 visits. This surpassed the prior record of 17,502 visits per day in October 2013. Thanks for your support, and we welcome your suggestions on how to make PathologyOutlines.com even more useful to the Pathology community.
(4) We're back from USCAP, where we had a great show talking to existing and new prospective reviewers, and getting feedback from our visitors. We'll let you know about any new ideas we are working on.
Visit and follow our Blog to see recent updates to the website.
(1) Thanks to Baylor College of Medicine (who posted ad #4000) and the 3,999 other advertisers we've had since PathologyOutlines.com started in August 2001. For many years, pathologists were very skeptical about our website - how could it possibly be free? By now, most pathologists recognize that it is, in fact, a free, no registration website, paid for by advertising of pathology related jobs, conferences and fellowships. We also have advertising on our Home page, our Chapters, Management page, Case of the Week and other emails. We also have an affiliate relationship with Amazon, meaning that they pay us ~ 5% of the purchase price of anything bought on Amazon.com, if you enter Amazon through our website (by clicking on a link or banner). We also promote books of various publishers, and receive money when visitors click on Google ads. We do NOT allow popup ads, or other obnoxious ads. The free website model has worked very well for us.
(2) We have (finally) converted all 6,700+ topics on our website to topic format, with completion of the Eye chapter. The next big task is converting to a template based system that will also adapt to tablets and smart phones. This is (still) under development, but we hope to get it started soon.
(3) In February 2014, we again had record traffic, with a daily average of 18,323 visits. This surpassed the prior record of 17,502 visits per day in October 2013. Thanks for your support, and we welcome your suggestions on how to make PathologyOutlines.com even more useful to the Pathology community.
(4) We're back from USCAP, where we had a great show talking to existing and new prospective reviewers, and getting feedback from our visitors. We'll let you know about any new ideas we are working on.
Visit and follow our Blog to see recent updates to the website.
Case #303
Case #1 (contributed by Dr. Raul Gonzalez)
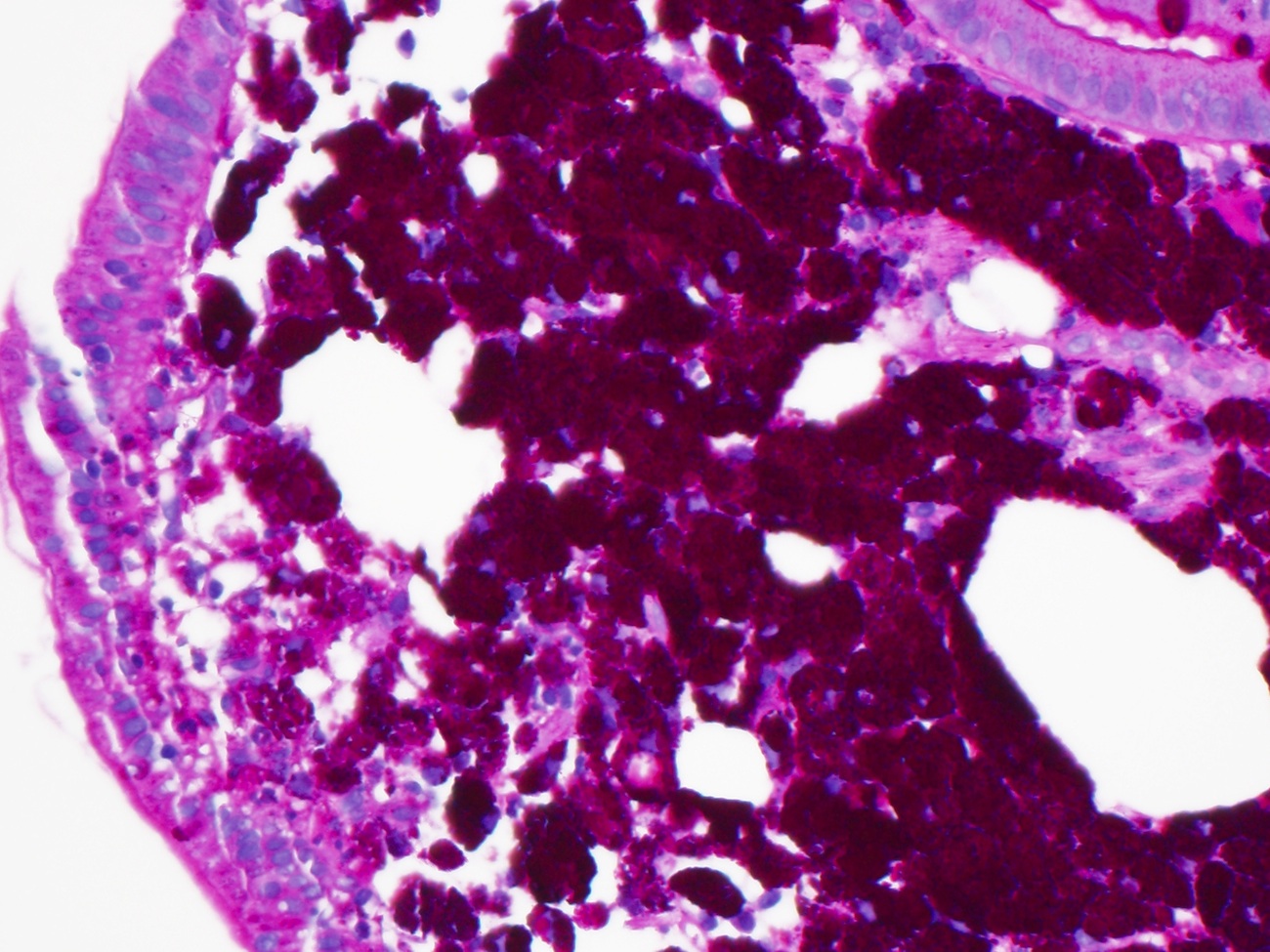
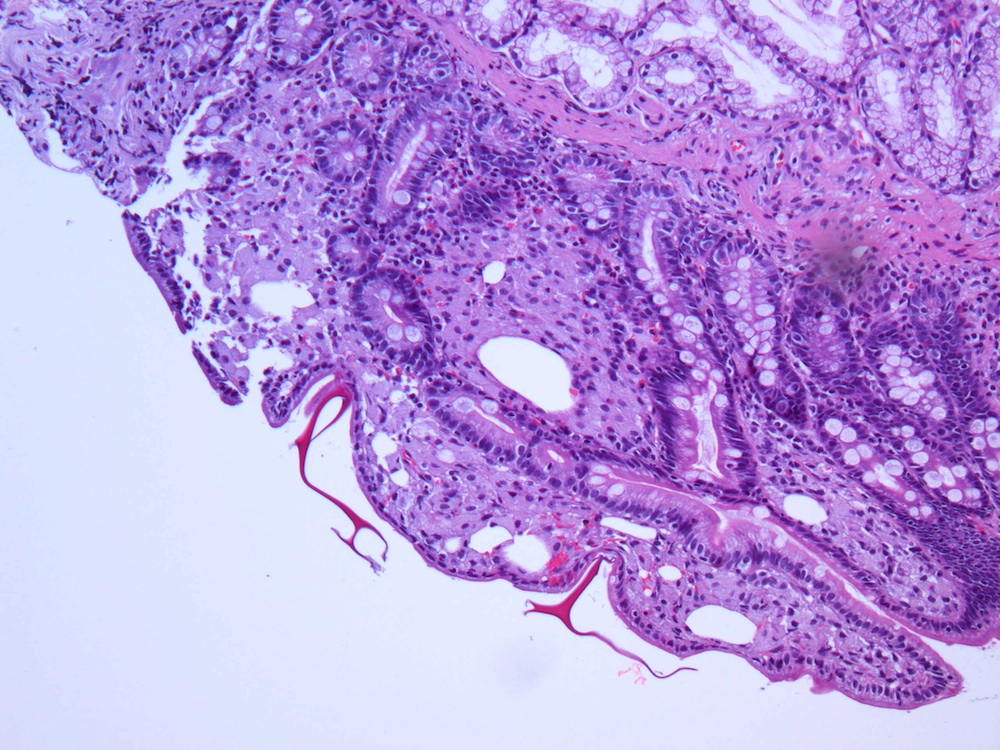
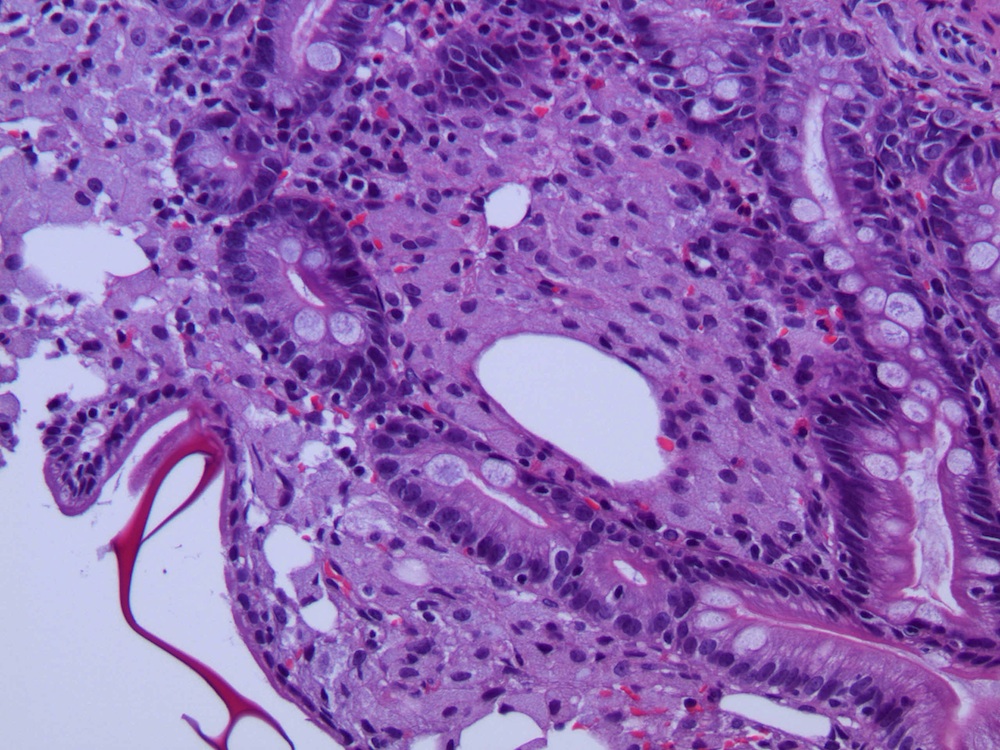
A 50 year old man presented with upper GI bleeding and friable duodenal mucosa on endoscopy.
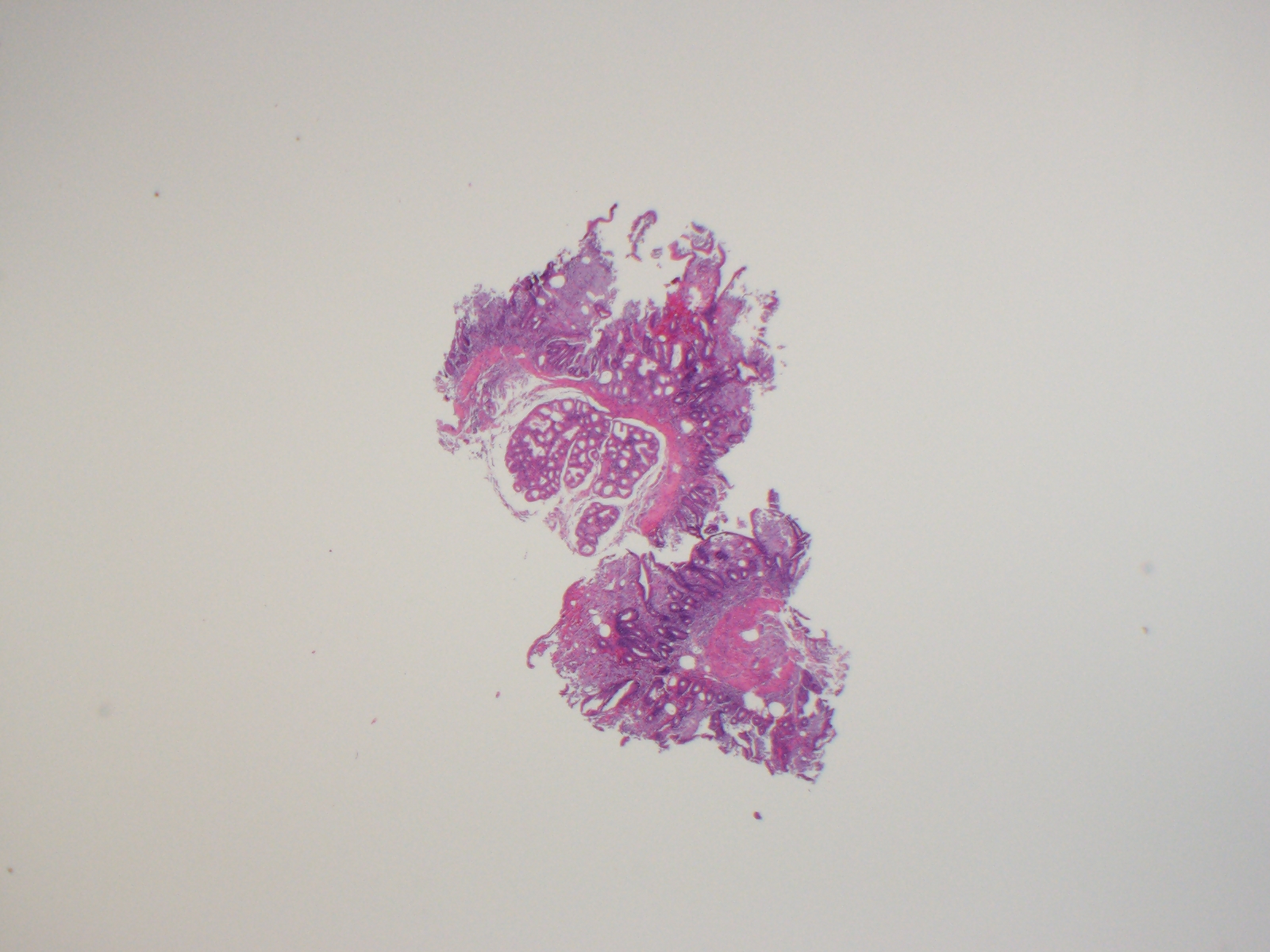
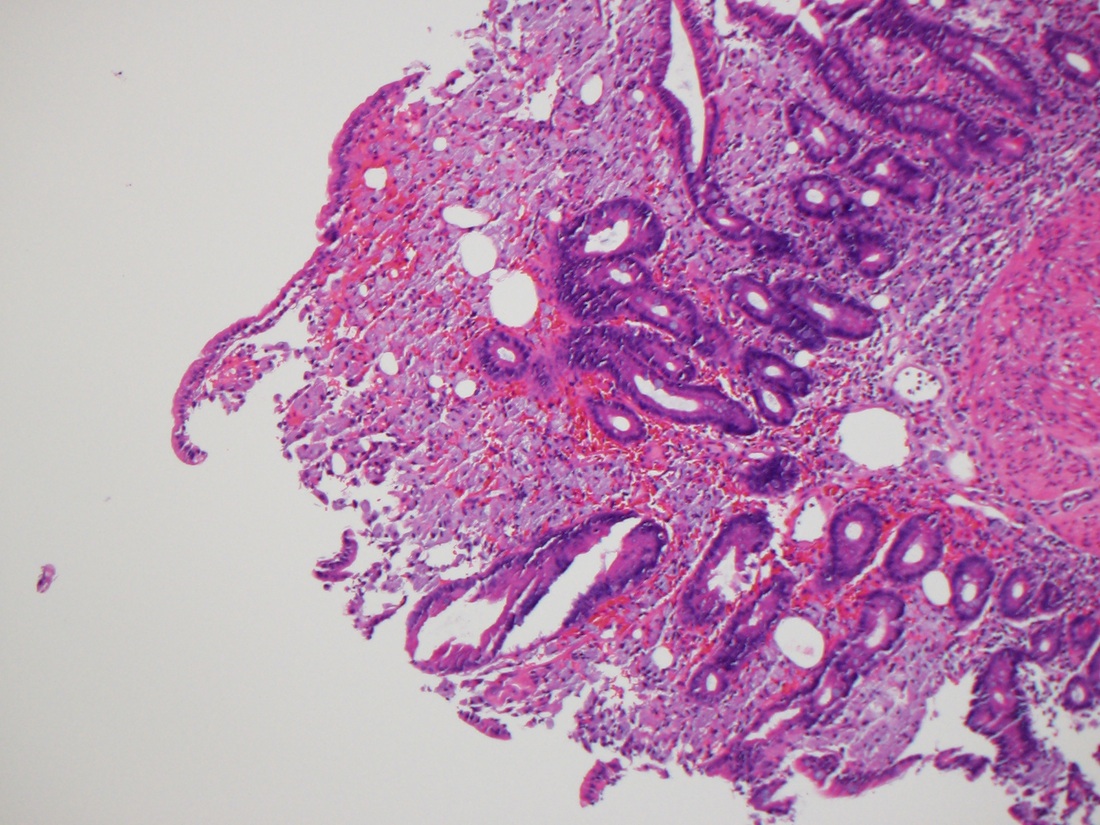
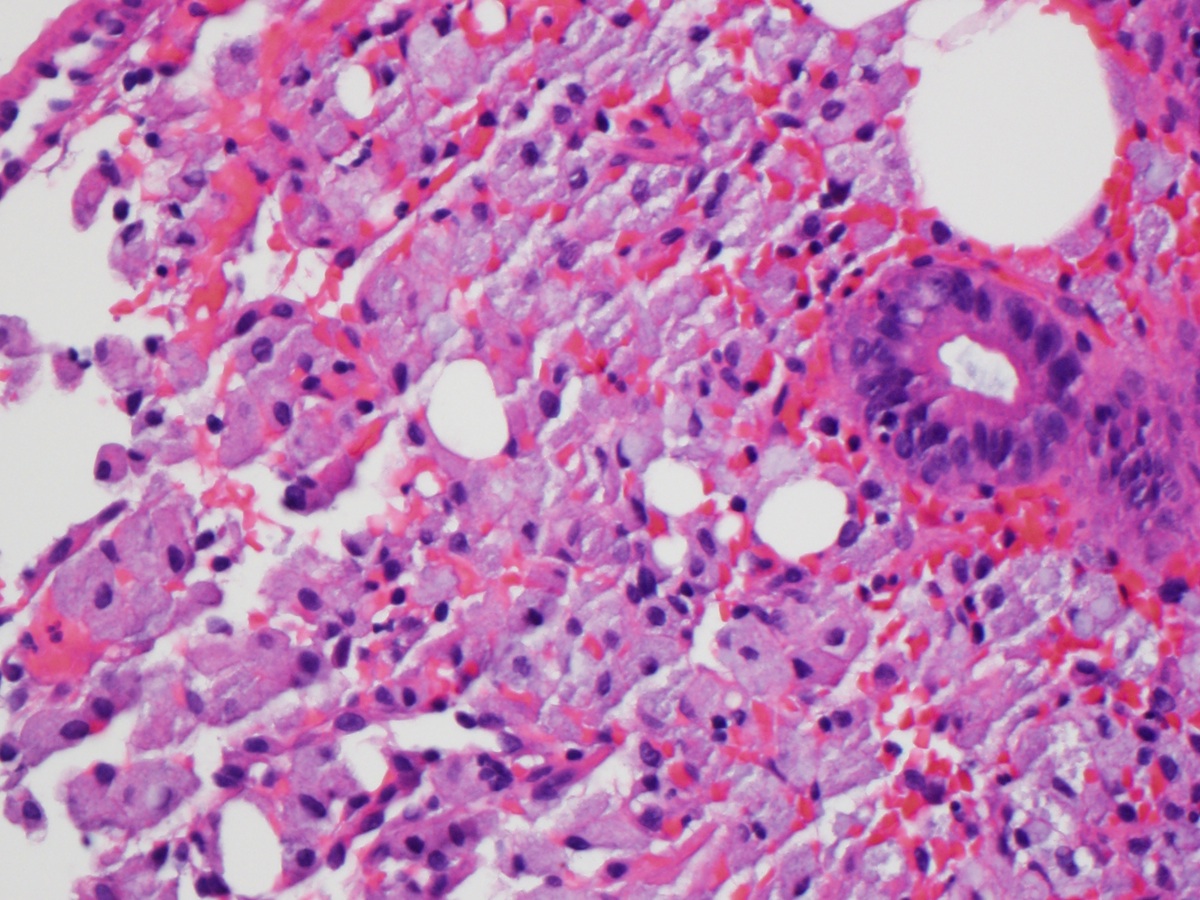
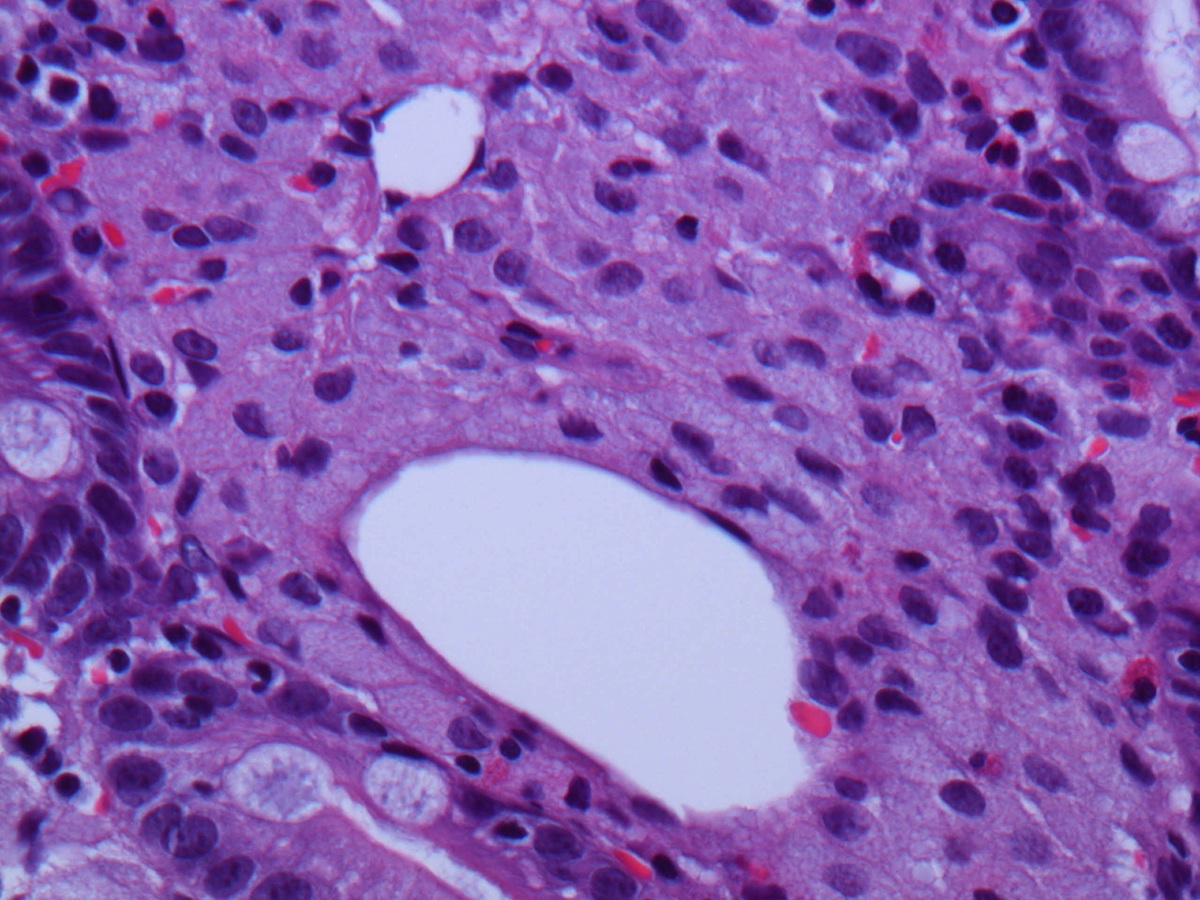
H&E
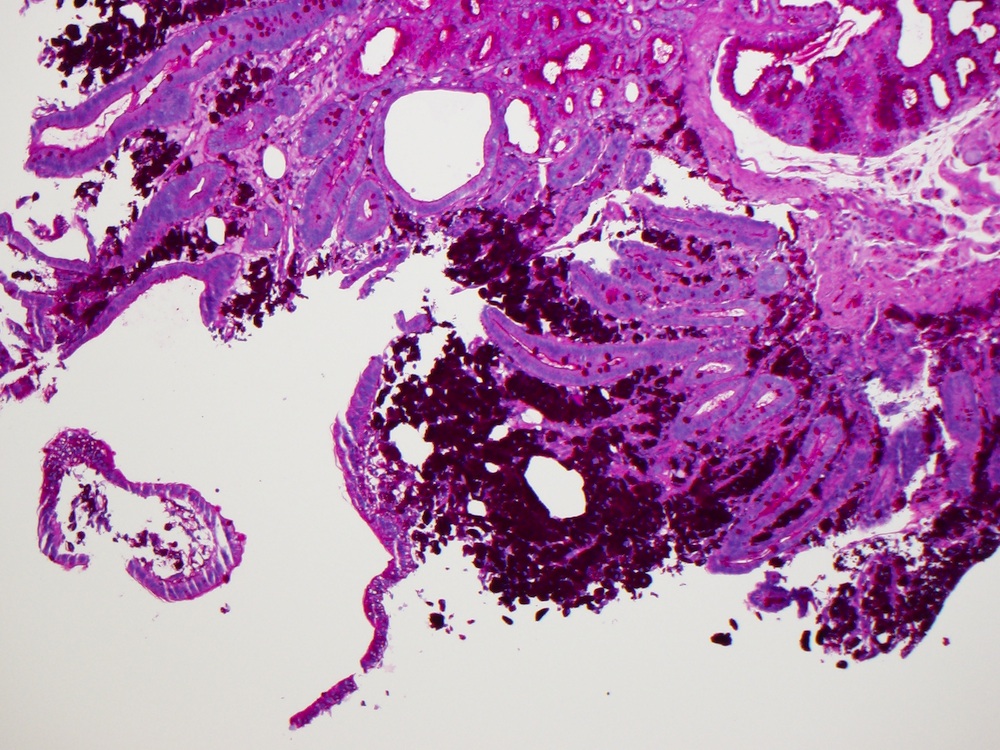
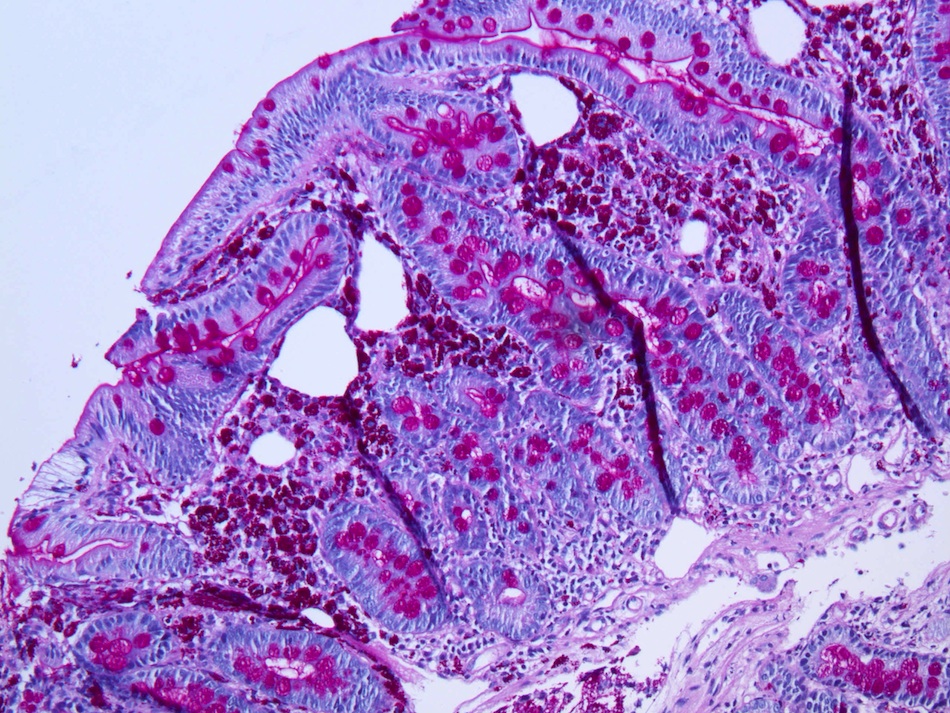
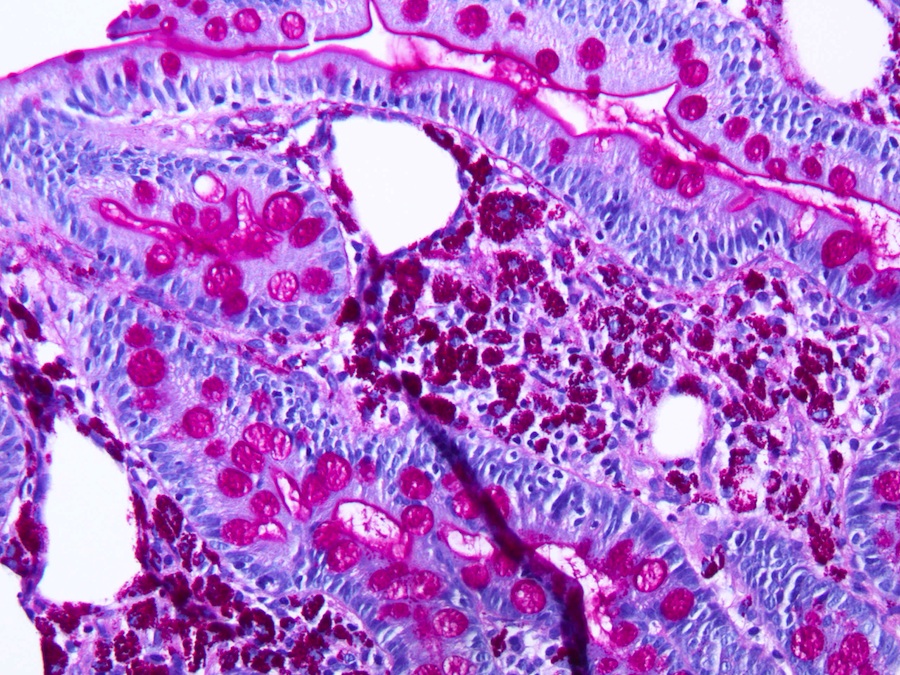
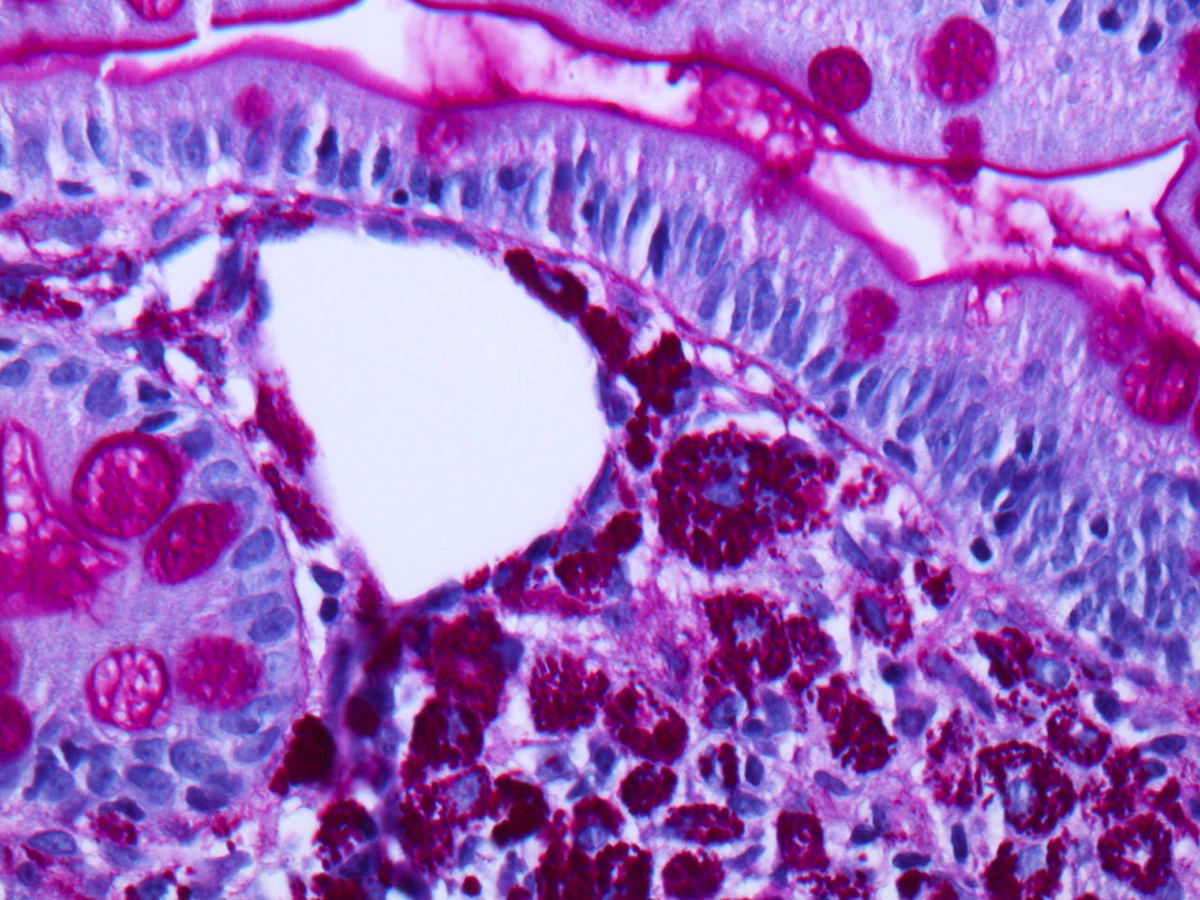
PAS stain
Case #2 (contributed by Dr. Don Xu)
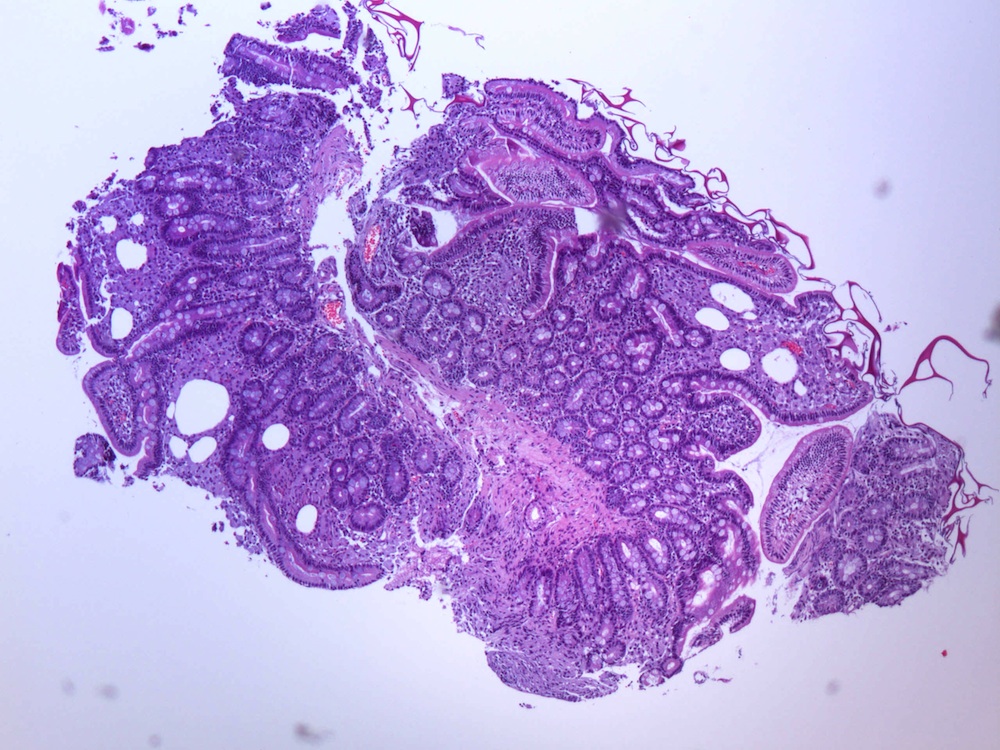
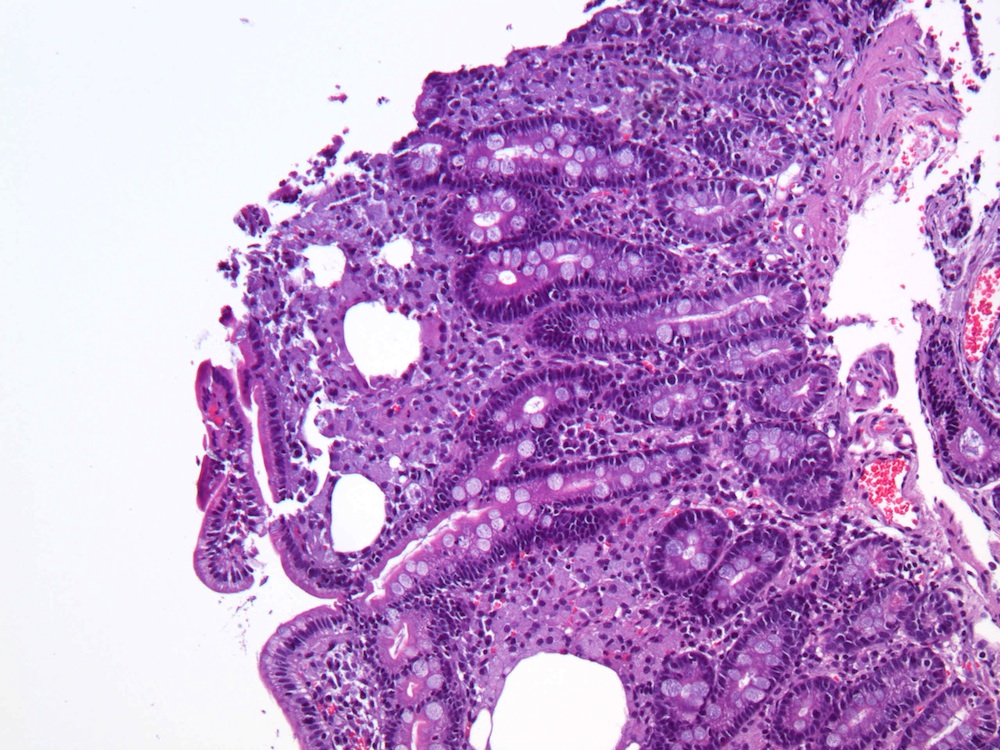
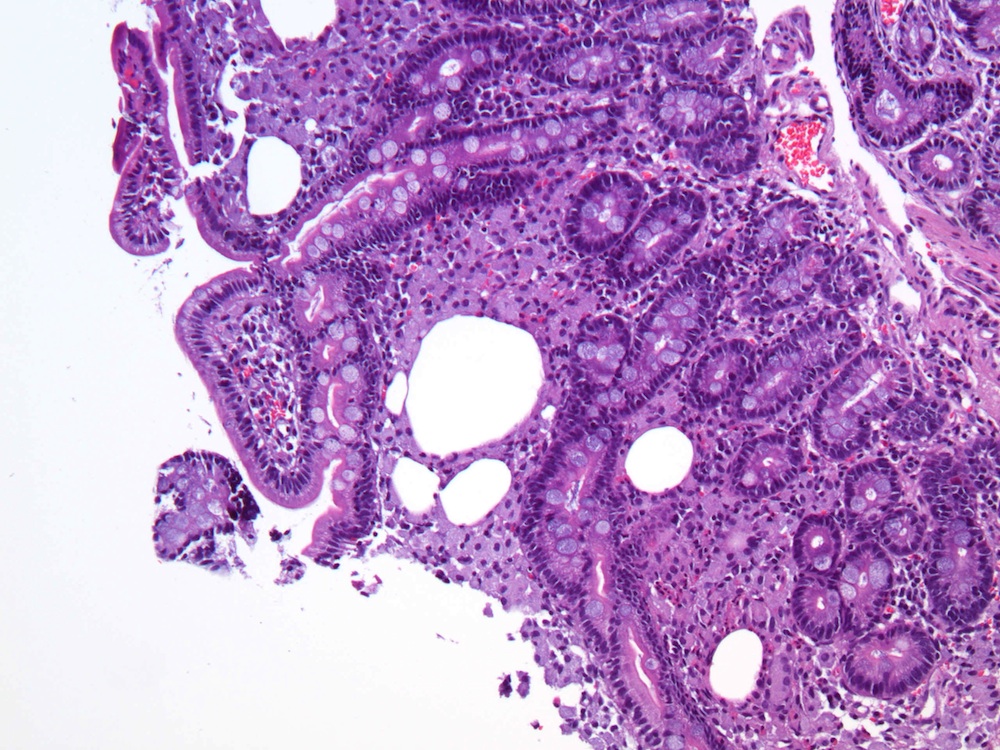
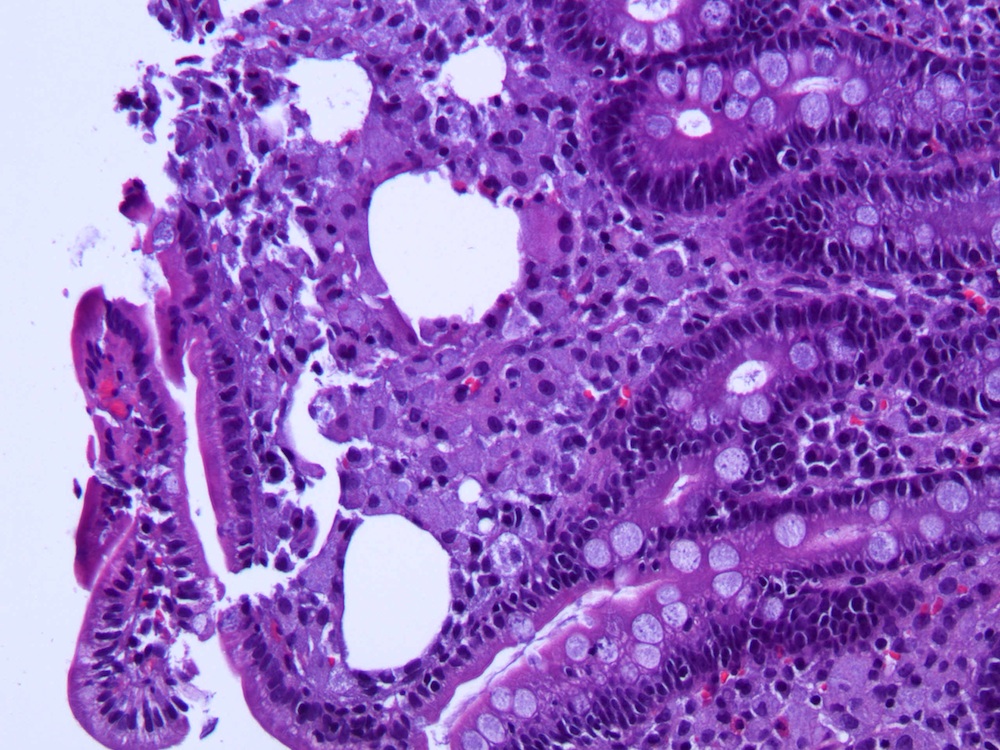
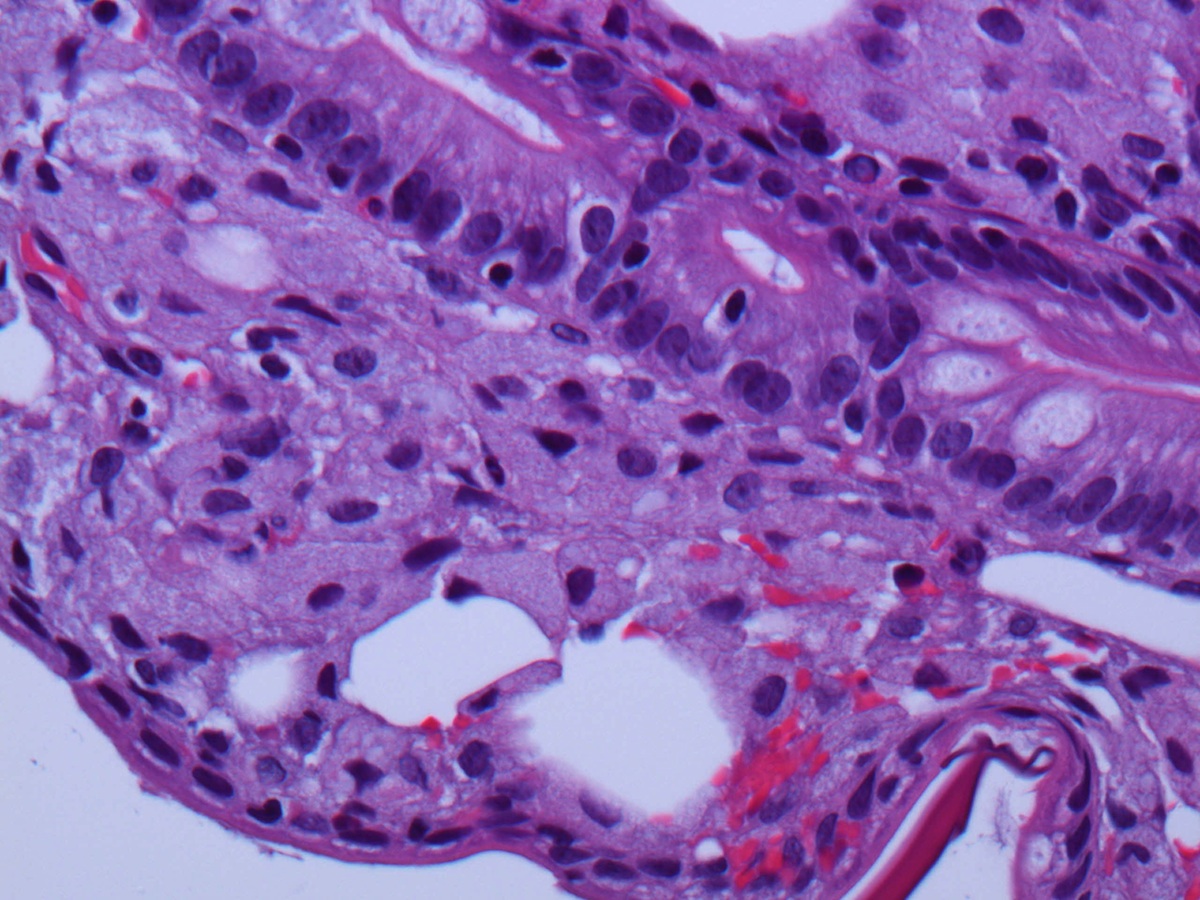
A 47 year old man with a history of chronic arthralgias for 2 years presented with fevers, abdominal pain, and weight loss. He was found to have microcytic anemia and mesenteric and retroperitoneal lymphadenopathy. The pictures of duodenal biopsy are shown.
H&E
PAS stain
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Whipple's disease
Discussion:
Both cases showed blunted villi and expansion of the lamina propria by foamy histiocytes. Periodic acid Schiff (PAS) stain revealed numerous microorganisms within macrophages. In case #1, unstained slides were sent to an outside institution for Tropheryma whipplei immunostain, which was positive. In case #2, PCR study confirmed Tropheryma whipplei infection.
Whipple's disease is a rare systemic infection due to Tropheryma whippelii, a gram positive intracellular actinomycete, first described in 1907 by Dr. George Hoyt Whipple (World J Gastroenterol 2009;15:2078, Wikipedia: George Whipple [Accessed 25 March 2024]). Dr. Whipple won the Nobel Prize (jointly) in 1934 for another discovery, that liver given as food to dogs reversed the anemia, leading to treatment of pernicious anemia (The Noble Prize: George H. Whipple [Accessed 25 March 2024]). He was friends of Dr. Allen Whipple, a surgeon who described the Whipple procedure and the Whipple's triad of insulinoma (Wikipedia: Allen Whipple [Accessed 25 March 2024]).
Whipple's disease, also called intestinal lipodystrophy, typically affects white men ages 30 - 49 years, in the proximal intestine and mesenteric lymph nodes. Patients typically present with malabsorption (diarrhea, weight loss, abdominal pain), and occasionally polyarthritis, lymphadenopathy, hyperpigmentation and CNS complaints. Histology, in addition to the above features, shows dilated lymphatics or fat vacuoles. It may show multinucleated giant cells. EM shows rod-like organisms.
The differential diagnosis includes:
- Histoplasmosis: faint blue dot-like inclusions surrounded by a clear halo, PAS or silver stain shows budding yeast
- Mycobacterium avium-intracellulare infection: immunocompromised patients, patchy infection, no lipid vacuoles, PAS shows faintly positive bacillary forms
- Mineral oil ingestion
Treatment is with antibiotics, which must be continued for at least a year, or there is a high rate of relapse.