13 November 2013 - Case #291
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Mitra Mehrad, M.D., Barnes-Jewish Hospital, Missouri (USA) for contributing this case.
Case #291
Clinical history:
A 47 year old woman with sinusitis and nasal polyps underwent endoscopic sinus surgery.
Microscopic images:
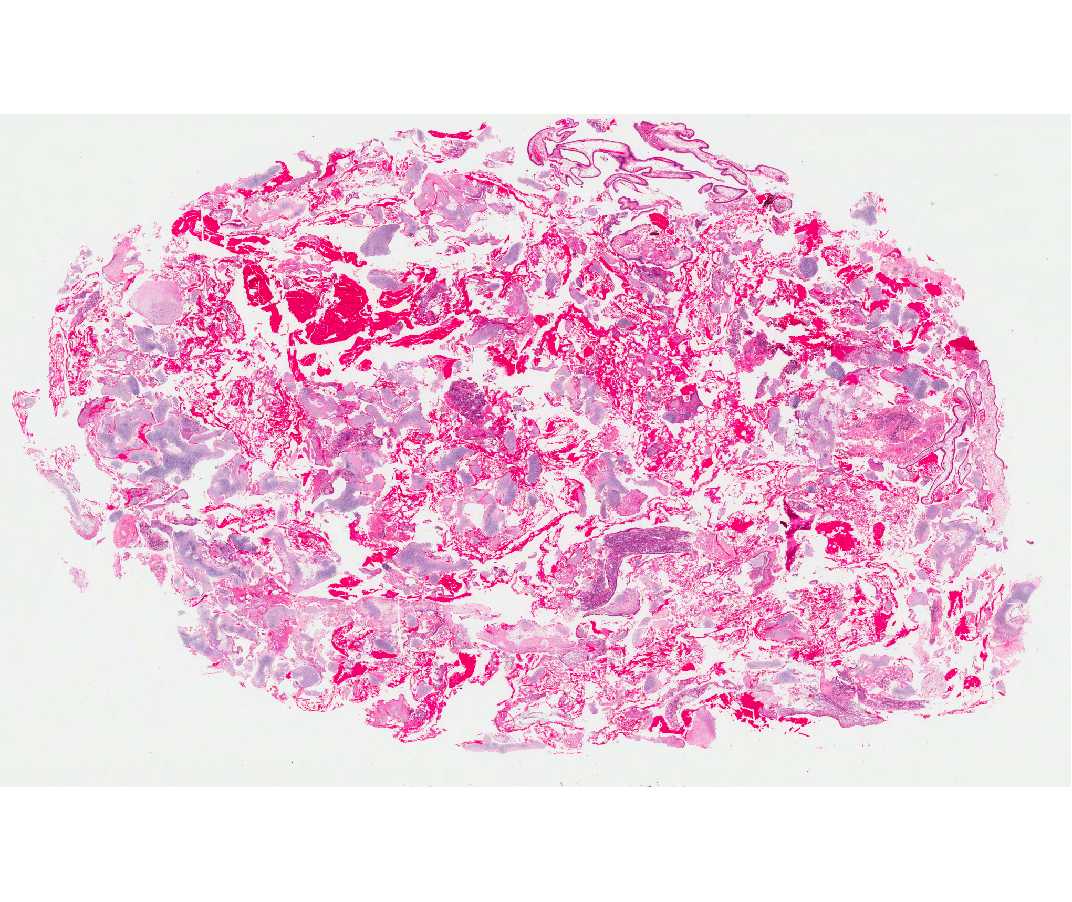
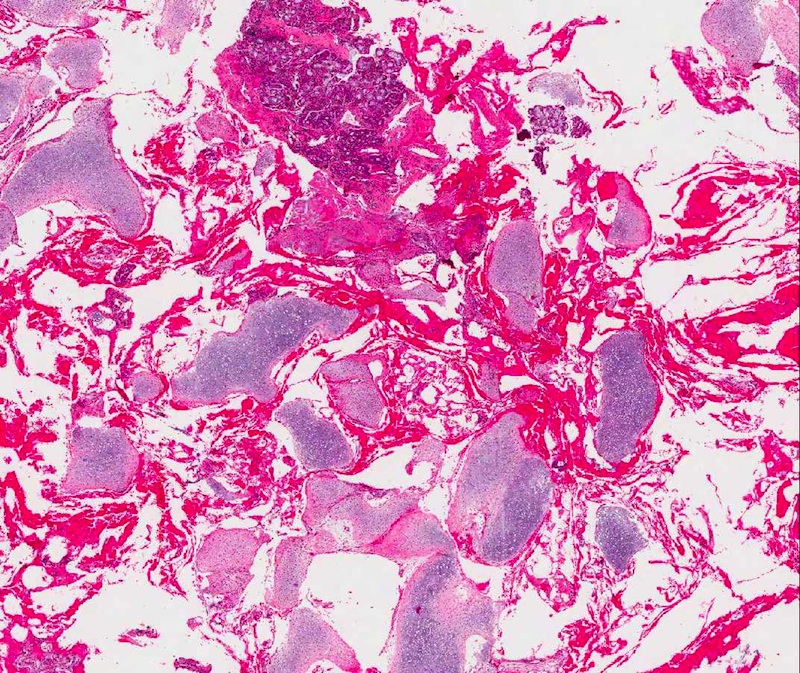
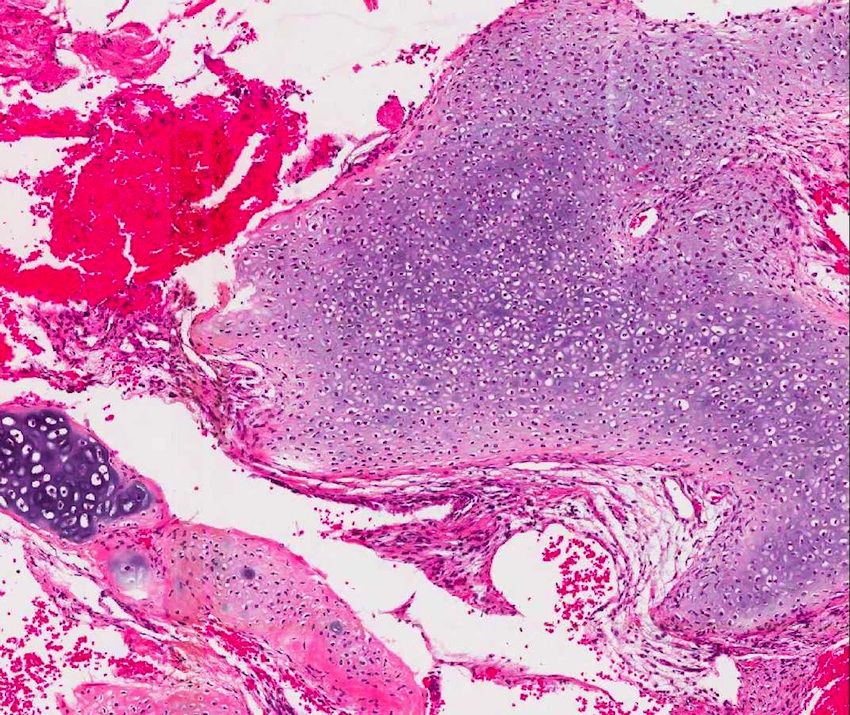

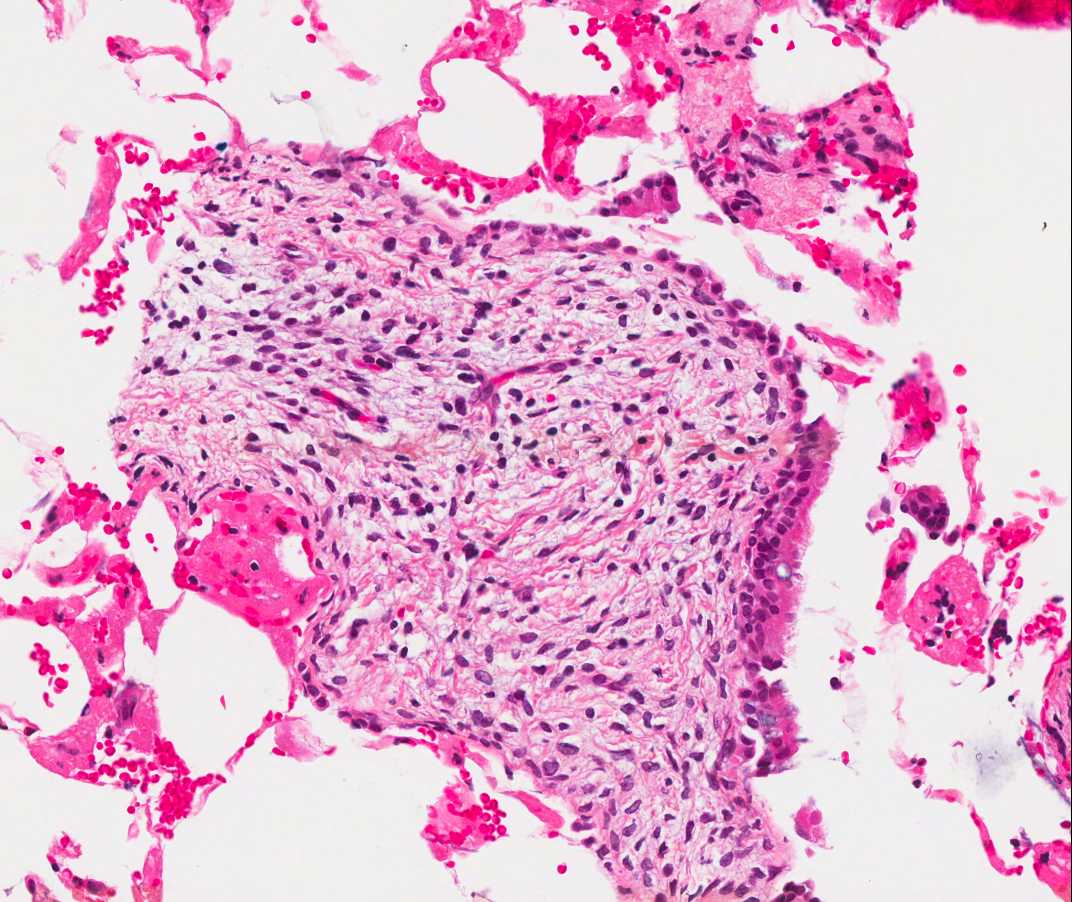
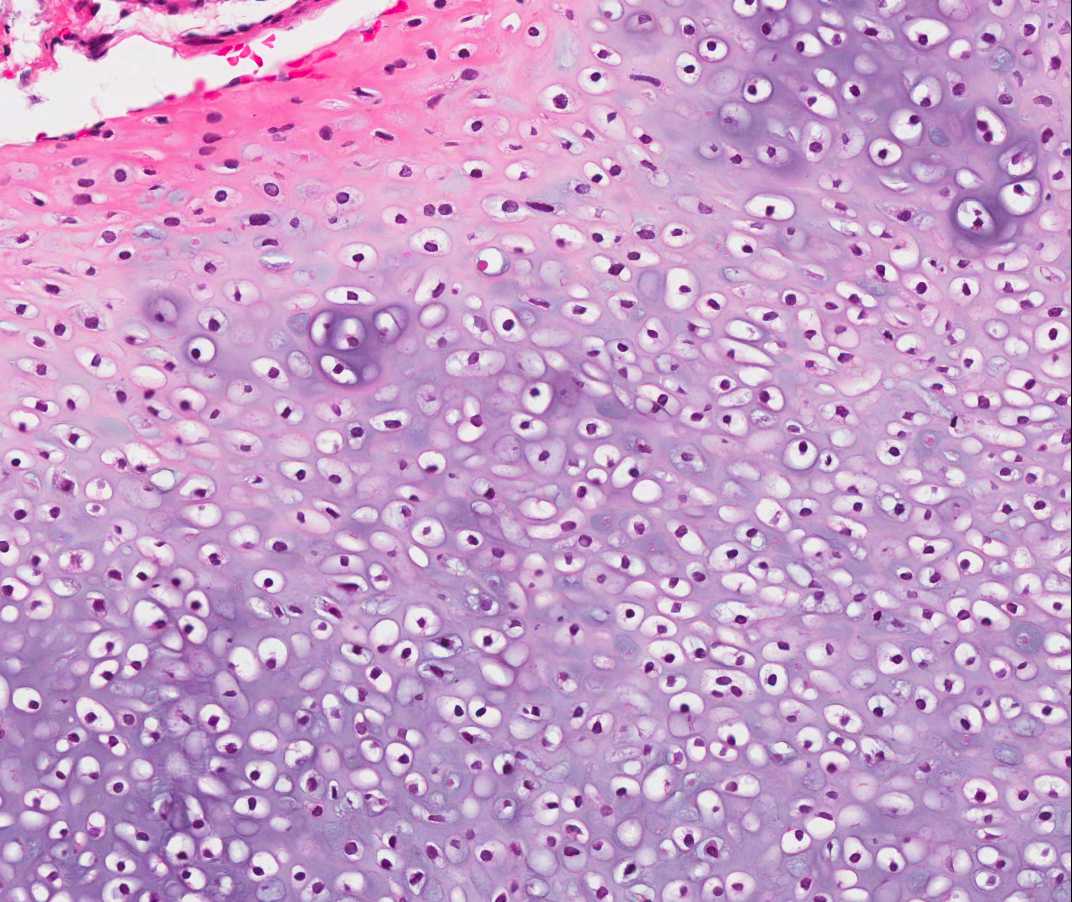
What is your diagnosis?
Diagnosis: Nasal chondromesenchymal hamartoma
Discussion:
Nasal chondromesenchymal hamartoma is a rare, often cystic lesion that typically fills the nasal cavity and extends into the ethmoid sinuses. It was first reported in 1998 at Barnes-Jewish Hospital, where this Case of the Week originated (Am J Surg Pathol 1998;22:425). It is considered an upper respiratory tract analogue of chest wall mesenchymal hamartoma. Although benign, it may erode the cribriform plate and have an intracranial component. It is more common in men (66%) and typically affects children, with a mean age of 14 months. Reports in adults are uncommon (Arch Pathol Lab Med 2005;129:1444). It is occasionally associated with pleuropulmonary blastoma (Int J Pediatr Otorhinolaryngol 2010;74:1240).
Histologically, as in this case, there is well demarcated mature cartilage, myxoid stroma and spindle cells. There may also be focal osteoclast-like giant cells, aneurysmal bone cyst-like formations and collagen fibers (Arch Pathol Lab Med 2001;125:400). Electron microscopy shows fibroblastic and myofibroblastic differentiation.
The differential diagnosis includes:
Surgical resection is usually curative, although it may be technically difficult because of the extent of disease. The first case of malignant transformation was recently reported (Histol Histopathol 2013;28:337).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Mitra Mehrad, M.D., Barnes-Jewish Hospital, Missouri (USA) for contributing this case.
Website news:
(1) In October 2013, we had record traffic of 542,590 visits, averaging 17,502 visits per day (total of 1.5 million page views, 11.9 million "hits"). Thanks for your support and your suggestions!
(2) We now list Conferences by subspecialty and by location on our Conferences page.
(3) New stains recently added to the Stains and Molecular Markers chapter include FOXL2, IDH1 and ISL1.
(4) Our Feature Page for November highlights Consumable Lab Products / Clinical Lab Analyzers and includes Leica Biosystems, Sakura Finetek USA and Ventana Medical.
(5) We posted a new section, Personnel Management, in our Laboratory Administration chapter, written by Richard Horowitz, M.D. I personally found these topics helpful in managing our business and recommend them to everyone involved in management in some way.
Visit and follow our Blog to see recent updates to the website.
(1) In October 2013, we had record traffic of 542,590 visits, averaging 17,502 visits per day (total of 1.5 million page views, 11.9 million "hits"). Thanks for your support and your suggestions!
(2) We now list Conferences by subspecialty and by location on our Conferences page.
(3) New stains recently added to the Stains and Molecular Markers chapter include FOXL2, IDH1 and ISL1.
(4) Our Feature Page for November highlights Consumable Lab Products / Clinical Lab Analyzers and includes Leica Biosystems, Sakura Finetek USA and Ventana Medical.
(5) We posted a new section, Personnel Management, in our Laboratory Administration chapter, written by Richard Horowitz, M.D. I personally found these topics helpful in managing our business and recommend them to everyone involved in management in some way.
Visit and follow our Blog to see recent updates to the website.
Case #291
Clinical history:
A 47 year old woman with sinusitis and nasal polyps underwent endoscopic sinus surgery.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Nasal chondromesenchymal hamartoma
Discussion:
Nasal chondromesenchymal hamartoma is a rare, often cystic lesion that typically fills the nasal cavity and extends into the ethmoid sinuses. It was first reported in 1998 at Barnes-Jewish Hospital, where this Case of the Week originated (Am J Surg Pathol 1998;22:425). It is considered an upper respiratory tract analogue of chest wall mesenchymal hamartoma. Although benign, it may erode the cribriform plate and have an intracranial component. It is more common in men (66%) and typically affects children, with a mean age of 14 months. Reports in adults are uncommon (Arch Pathol Lab Med 2005;129:1444). It is occasionally associated with pleuropulmonary blastoma (Int J Pediatr Otorhinolaryngol 2010;74:1240).
Histologically, as in this case, there is well demarcated mature cartilage, myxoid stroma and spindle cells. There may also be focal osteoclast-like giant cells, aneurysmal bone cyst-like formations and collagen fibers (Arch Pathol Lab Med 2001;125:400). Electron microscopy shows fibroblastic and myofibroblastic differentiation.
The differential diagnosis includes:
- Aneurysmal bone cyst: uncommon in nasal cavity; grows rapidly at other sites; expanding osteolytic lesion of blood-filled spaces of variable size separated by connective tissue septa with osteoclast giant cells and variable reactive bone; typically no cartilage, prominent giant cells with 10 - 20 nuclei that aggregate in groups of 6 - 12 cells; also metaplastic woven bone and lamellar bone lined by osteoblasts and occasionally osteoclasts
- Chondroblastoma: typically teenage boys with epiphyseal tumor
- Chondromyxoid fibroma: ages 15 - 25, affects metaphysis of long tubular bones, small bones of feet or any bone, skull base; atypia is common, including large, hyperchromatic nuclei
- Fibrous dysplasia: medulla of diaphysis or metaphysis of craniofacial bones, femur, ribs are most common; mean age 32 years; curvilinear trabeculae (Chinese letters) of metaplastic woven bone (never matures) in hypocellular, fibroblastic stroma
- Osteochondromyxoma: also occurs in nasal region; sheets and lobules of bland cells in myxomatous, cartilaginous, osseous and hyaline fibrous matrix; erodes bone and frequently extends into soft tissue; lacks giant cells and aneurysmal bone cyst type reaction
Surgical resection is usually curative, although it may be technically difficult because of the extent of disease. The first case of malignant transformation was recently reported (Histol Histopathol 2013;28:337).