7 June 2012 - Case #244
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Mingyi Chen, University of California-Davis Medical Center, for contributing this case and the discussion.
Advertisement
Case #244
Clinical history:
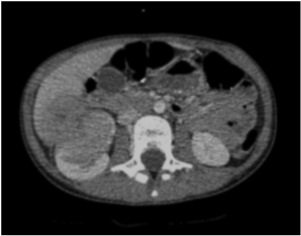
An 11 year old girl with no prior medical history presented with abdominal pain, fever, general fatigue, night sweats and anemia. Computed tomography scan showed a 4 centimeter tumor in the right kidney extending into the liver and multiple 1 - 2 millimeter lung nodules.
The clinical differential diagnosis included lymphoma, Wilm's tumor and an unknown primary with metastasis. A renal biopsy was obtained.
Radiology image:
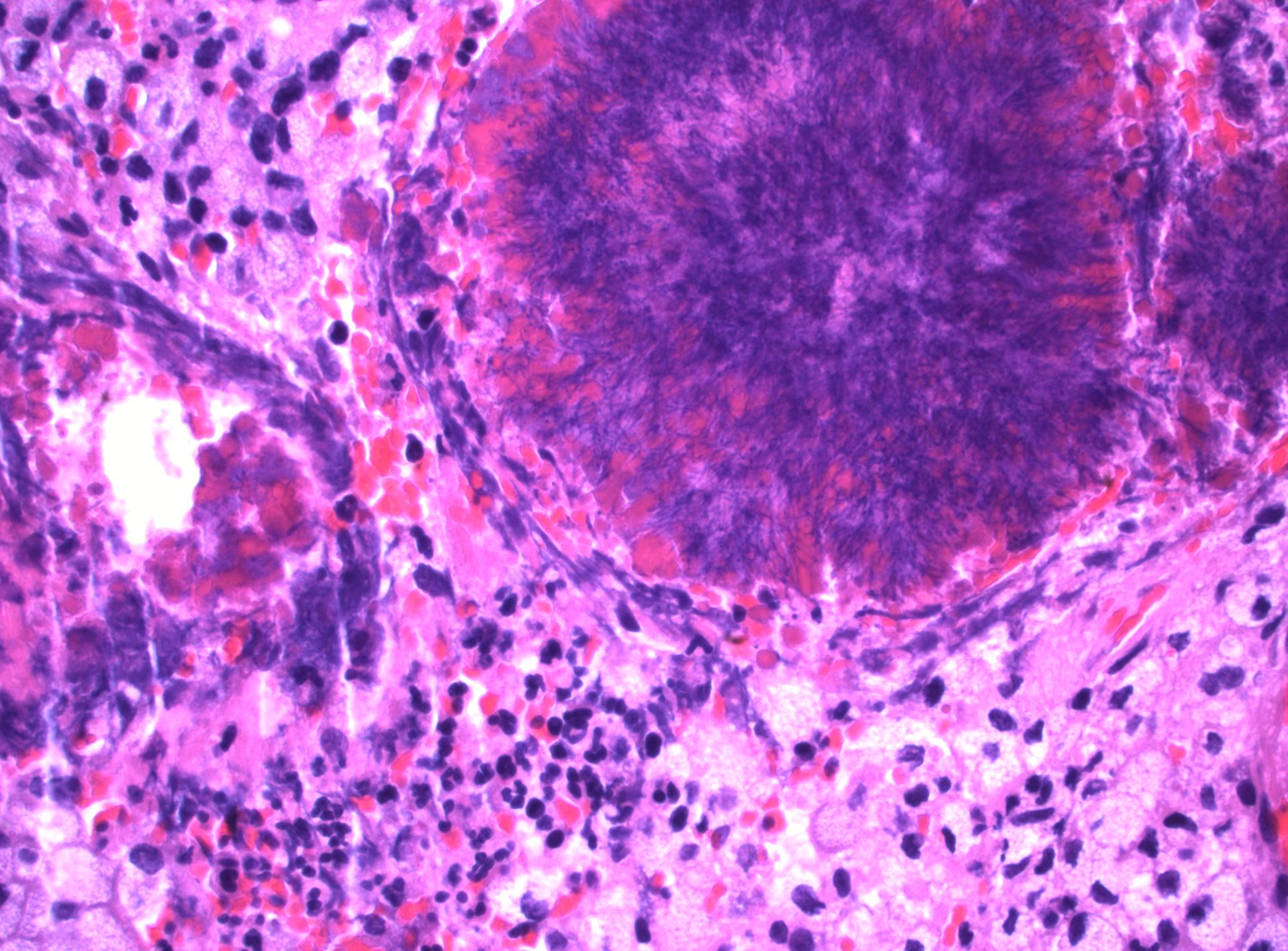
Microscopic image:
What is your diagnosis?
Diagnosis: Renal actinomycosis
Discussion:
The renal biopsy showed marked acute and chronic inflammation with occasional sulfur granules characteristic of Actinomyces species.
Actinomycosis is a chronic suppurative and granulomatous disease of the cervicofacial, thoracic or abdominal areas caused by the Actinomyces species. It is sometimes called the most misdiagnosed disease, because abscesses can mimic malignancy, as in this case. As a result, these abscesses may cause unnecessary surgical resections.
Actinomyces are anaerobic gram positive nonacid fast filamentous bacteria that are normal flora in the mouth and gastrointestinal tract. Actinomycosis is most frequently caused by Actinomyces israelii, part of the normal flora in the vagina, colon and mouth. Infection is established by a breach of the mucosal barrier during dental, GI or other procedures or due to diseases such as diverticulitis or appendicitis.
Actinomyces israelii is also the most common cause of disseminated actinomycosis. Disseminated disease is usually caused by perforation of the gastrointestinal tract, intrauterine devices, aspiration or poor oral hygiene.
This patient was successfully treated with antibiotics postoperatively and without complications. Although renal actinomycosis is rare, it should be included in the differential diagnosis for a renal mass.
References: South Med J 2004;97:316, Am Surg 2000 66:85
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Mingyi Chen, University of California-Davis Medical Center, for contributing this case and the discussion.

Dont miss an issue of the basic pathology research journal
covering all biomedical disciplines in the broad spectrum of pathology.
Sign up for free alerts from Laboratory Investigation by clicking here.
www.LaboratoryInvestigation.org
Website news:
(1) The Ovary-nontumor chapter has now been updated, based on reviews by Mohiedean Ghofrani, M.D. and Shahidul Islam, M.D. The Colon tumor chapter has also been updated, based on reviews by Jela Bandovic, M.D., Shilpa Jain, M.D. and Charanjeet Singh, M.D.
(2) Our Feature Page for the month highlights Diagnostic testing / reagents, and includes Advanced Cell Diagnostics, Inc. (ACD), bioTheranostics, Covance, Epitomics, Horizon Diagnostics, Leica Microsystems and Ventana Medical.
(3) Can you help us motivate students to make education a priority? As you may know, PathologyOutlines.com is the primary sponsor of The Detroit College Promise, a tax exempt nonprofit now in its 4th year of providing scholarships. We have just received a challenge grant of $10,000, contingent on our raising $20,000 in contributions by July 15, 2012. As pathologists, we know the importance of education and motivation, and we hope you are able to make a contribution towards this challenge grant. Every dollar raised is used exclusively for scholarships offered to Detroit Public School students. Click here to make a tax deductible contribution today. Whatever you give will be appreciated and matched 50% by the challenge grant. Thanks for your support!
Visit and follow our Blog to see recent updates to the website.
(1) The Ovary-nontumor chapter has now been updated, based on reviews by Mohiedean Ghofrani, M.D. and Shahidul Islam, M.D. The Colon tumor chapter has also been updated, based on reviews by Jela Bandovic, M.D., Shilpa Jain, M.D. and Charanjeet Singh, M.D.
(2) Our Feature Page for the month highlights Diagnostic testing / reagents, and includes Advanced Cell Diagnostics, Inc. (ACD), bioTheranostics, Covance, Epitomics, Horizon Diagnostics, Leica Microsystems and Ventana Medical.
(3) Can you help us motivate students to make education a priority? As you may know, PathologyOutlines.com is the primary sponsor of The Detroit College Promise, a tax exempt nonprofit now in its 4th year of providing scholarships. We have just received a challenge grant of $10,000, contingent on our raising $20,000 in contributions by July 15, 2012. As pathologists, we know the importance of education and motivation, and we hope you are able to make a contribution towards this challenge grant. Every dollar raised is used exclusively for scholarships offered to Detroit Public School students. Click here to make a tax deductible contribution today. Whatever you give will be appreciated and matched 50% by the challenge grant. Thanks for your support!
Visit and follow our Blog to see recent updates to the website.
Case #244
Clinical history:
An 11 year old girl with no prior medical history presented with abdominal pain, fever, general fatigue, night sweats and anemia. Computed tomography scan showed a 4 centimeter tumor in the right kidney extending into the liver and multiple 1 - 2 millimeter lung nodules.
The clinical differential diagnosis included lymphoma, Wilm's tumor and an unknown primary with metastasis. A renal biopsy was obtained.
Radiology image:
CT scan
Microscopic image:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Renal actinomycosis
Discussion:
The renal biopsy showed marked acute and chronic inflammation with occasional sulfur granules characteristic of Actinomyces species.
Actinomycosis is a chronic suppurative and granulomatous disease of the cervicofacial, thoracic or abdominal areas caused by the Actinomyces species. It is sometimes called the most misdiagnosed disease, because abscesses can mimic malignancy, as in this case. As a result, these abscesses may cause unnecessary surgical resections.
Actinomyces are anaerobic gram positive nonacid fast filamentous bacteria that are normal flora in the mouth and gastrointestinal tract. Actinomycosis is most frequently caused by Actinomyces israelii, part of the normal flora in the vagina, colon and mouth. Infection is established by a breach of the mucosal barrier during dental, GI or other procedures or due to diseases such as diverticulitis or appendicitis.
Actinomyces israelii is also the most common cause of disseminated actinomycosis. Disseminated disease is usually caused by perforation of the gastrointestinal tract, intrauterine devices, aspiration or poor oral hygiene.
This patient was successfully treated with antibiotics postoperatively and without complications. Although renal actinomycosis is rare, it should be included in the differential diagnosis for a renal mass.
References: South Med J 2004;97:316, Am Surg 2000 66:85