All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. J. J. Sola, Clnica Universidad de Navarra, Pamplona (Spain), for contributing this case.


July 9-13, 2012
The Snow King Resort
Jackson, Wyoming (USA)
The 29th Annual Summer Update
in Clinical Immunology, Microbiology
and Infectious Disease
Course Topics:
This 23.75-hour review and update in the areas of clinical immunology, microbiology, and infectious diseases is intended to improve knowledge about the pathogenesis and clinical manifestations of infectious diseases, immunological mechanisms of disease and disease prevention, appropriate approaches to the diagnosis of infections and immunologic disorders, and utilization of the clinical microbiology and immunology laboratory, including selection and interpretation of results.
This course will provide a forum for the exchange of ideas dealing with microbial infections as well as immunity to infectious diseases and immunologic disorders. Faculty consists of clinicians involved in patient care, pathologists, and clinical laboratory scientists. Discussion of timely topics by faculty and participants assures that this course will be informative, interesting, and relevant.
Course Directors:
Harry R. Hill MD, Larry G. Reimer MD, July Daly PhD and John M. Matsen MD
Special Guests:
Paul G. Quie MD, Frederick A. Meier MD and John M. Matsen MD
Course CME:
This course is approved for 23.75 AMA PRA Category I Credit(s)
Website
Schedule
Hotel
Register
Case #240
Clinical history:
A 46 year old woman had a chronic history of abdominal discomfort. Five years ago, an ileal biopsy showed nonspecific chronic erosive inflammation and Crohn disease was clinically diagnosed. After a CT scan showed tumoral enlargement of the ileal wall, her terminal ileum was resected.
Gross images:


Microscopic images:

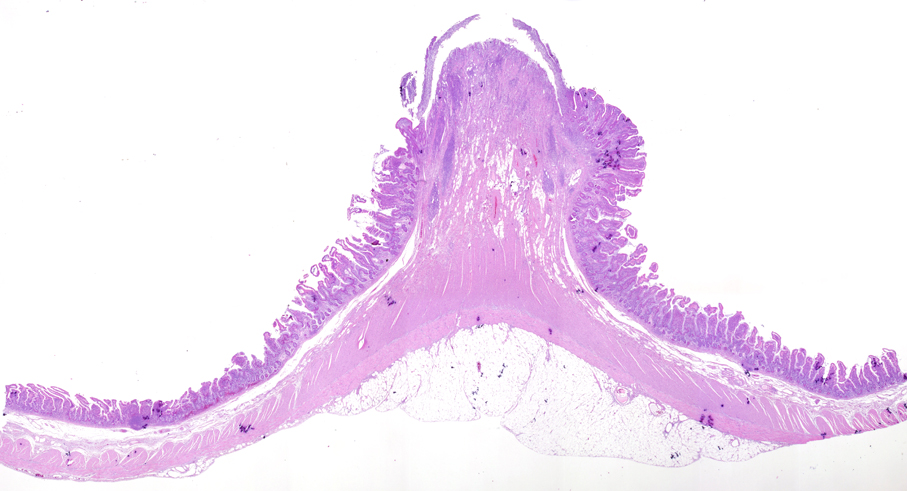
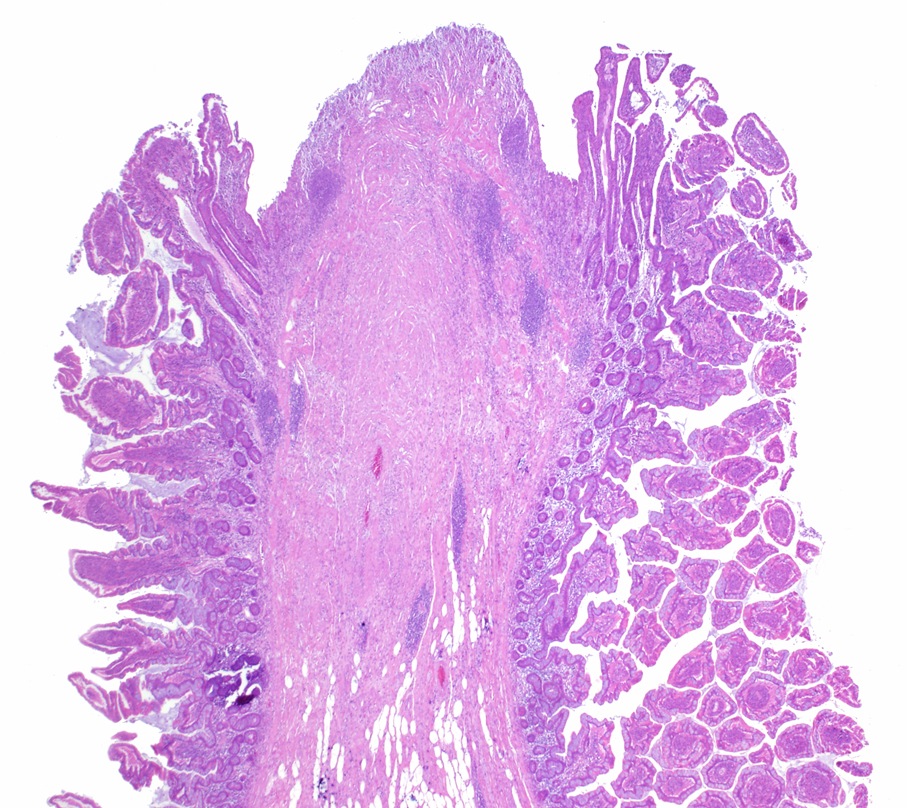

H&E
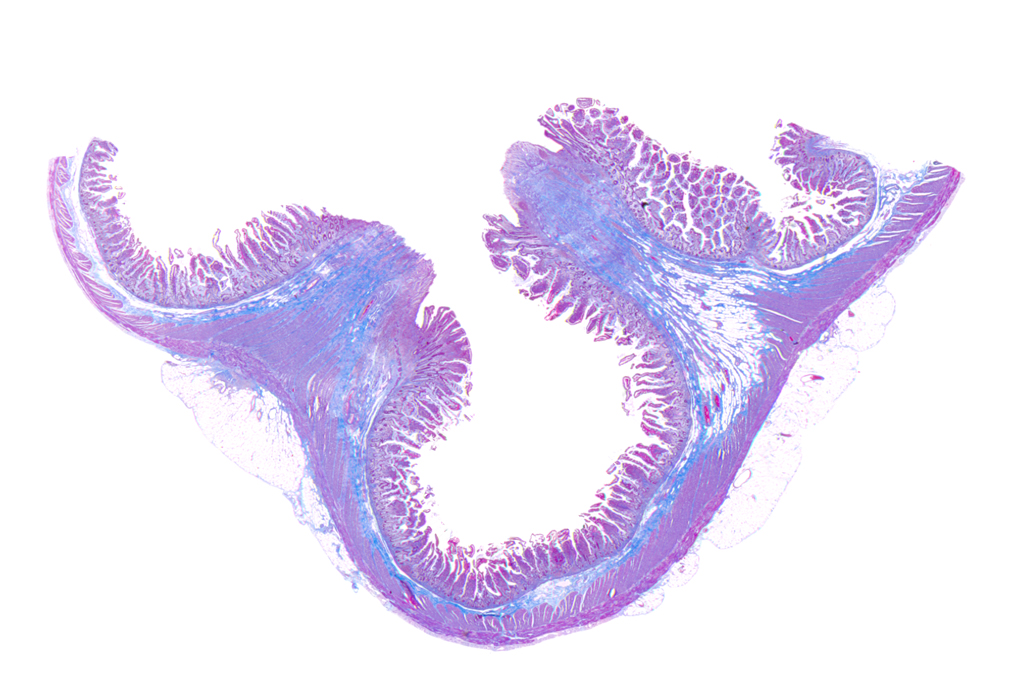

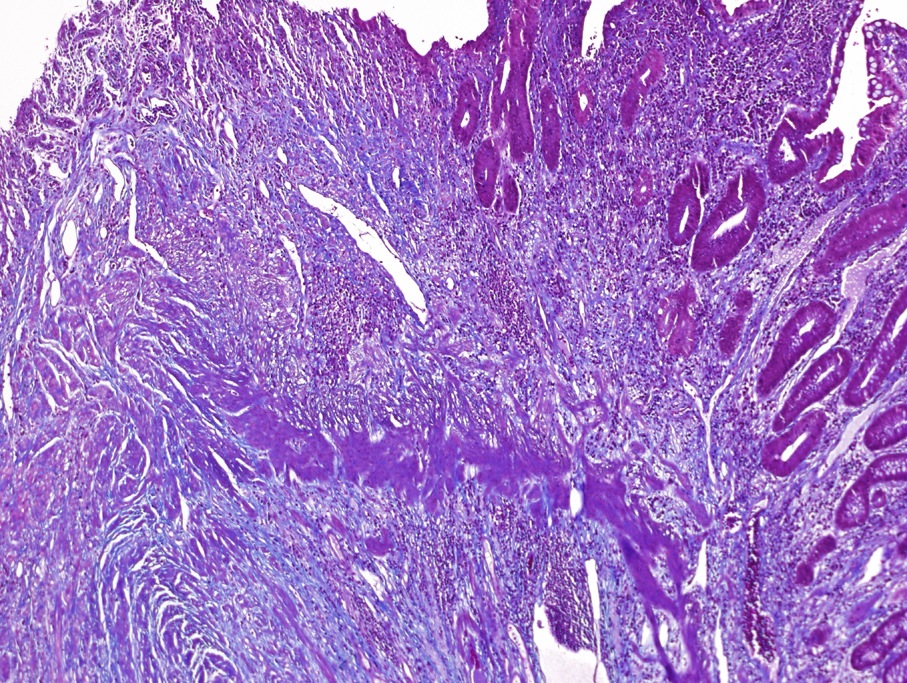
Trichrome
What is your diagnosis?
Diagnosis: Small bowel diaphragm disease
Discussion:
Diaphragm disease was first described in 1988, based on a review of small bowel resections to assess whether they exhibited any pathology related to nonsteroidal anti-inflammatory drugs / NSAIDs (J Clin Pathol 1988;41:516). A characteristic finding was the segmentation of the ileum by the formation of incomplete mucosal diaphragms, defined as thin circumferential membranes resembling the plica circularis, and composed of mucosa and submucosa with accompanying fibrosis. Other common gross features included ulceration, strictures and perforation. Histologically, these specimens also show neuromuscular and vascular hamartoma-like changes, eosinophilic enteritis and acute inflammation (Am J Clin Pathol 2008;130:518).
The differential diagnosis includes cryptogenic multifocal ulcerous stenosing enteritis (CMUSE), defined as small intestinal strictures and ulcerations of unknown origin (World J Gastroenterol 2011;17:2873). It is characterized as an atypical vasculitis presenting with unexplained stricture and ulceration of the small bowel in young and middle aged patients but without systemic inflammation. Of note, CMUSE can be treated with steroids.
Patients with diaphragm disease are often treated with surgery or endoscopic balloon dilation (Colorectal Dis 2012;14:804, Gastrointest Endosc 2006;64:1014). Cessation of NSAID use is recommended.
In this case, after the pathological diagnosis, a history of chronic low dose aspirin was discovered.