All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Tihana Dzombeta, University of Zagreb, Croatia, for contributing this case.


July 9-13, 2012
The Snow King Resort
Jackson, Wyoming (USA)
The 29th Annual Summer Update
in Clinical Immunology, Microbiology
and Infectious Disease
Course Topics:
This 23.75-hour review and update in the areas of clinical immunology, microbiology, and infectious diseases is intended to improve knowledge about the pathogenesis and clinical manifestations of infectious diseases, immunological mechanisms of disease and disease prevention, appropriate approaches to the diagnosis of infections and immunologic disorders, and utilization of the clinical microbiology and immunology laboratory, including selection and interpretation of results.
This course will provide a forum for the exchange of ideas dealing with microbial infections as well as immunity to infectious diseases and immunologic disorders. Faculty consists of clinicians involved in patient care, pathologists, and clinical laboratory scientists. Discussion of timely topics by faculty and participants assures that this course will be informative, interesting, and relevant.
Course Directors:
Harry R. Hill MD, Larry G. Reimer MD, July Daly PhD and John M. Matsen MD
Special Guests:
Paul G. Quie MD, Frederick A. Meier MD and John M. Matsen MD
Course CME:
This course is approved for 23.75 AMA PRA Category I Credit(s)
Website
Schedule
Hotel
Register
(1) We are constantly looking for Reviewers for each of our 7,000 topics, which we plan to update every 1-2 years. In particular, we are looking for reviewers of Soft Tissue Tumors and various Stains. Visit our newly updated Author Instructions page for more information.
(2) The Table of Contents of our Stains chapter now includes all 360 stains / biomarkers described in the chapter. The CD Markers chapter contains an additional 260 markers. We update these pages regularly, but let us know of any new markers we should include or other changes we should make.
(3) Our Feature Page for the month highlights Lab Accrediation, Education and CME, and includes A2LA, ARUP Laboratories and Clinical and Laboratory Standards Institute (CLSI).
(4) The Kidney tumor - cysts, children, adult benign chapter has now been updated, based on reviews by Mandolin Ziadie, M.D.
Visit and follow our Blog to see recent updates to the website.
Case #238
Clinical history:
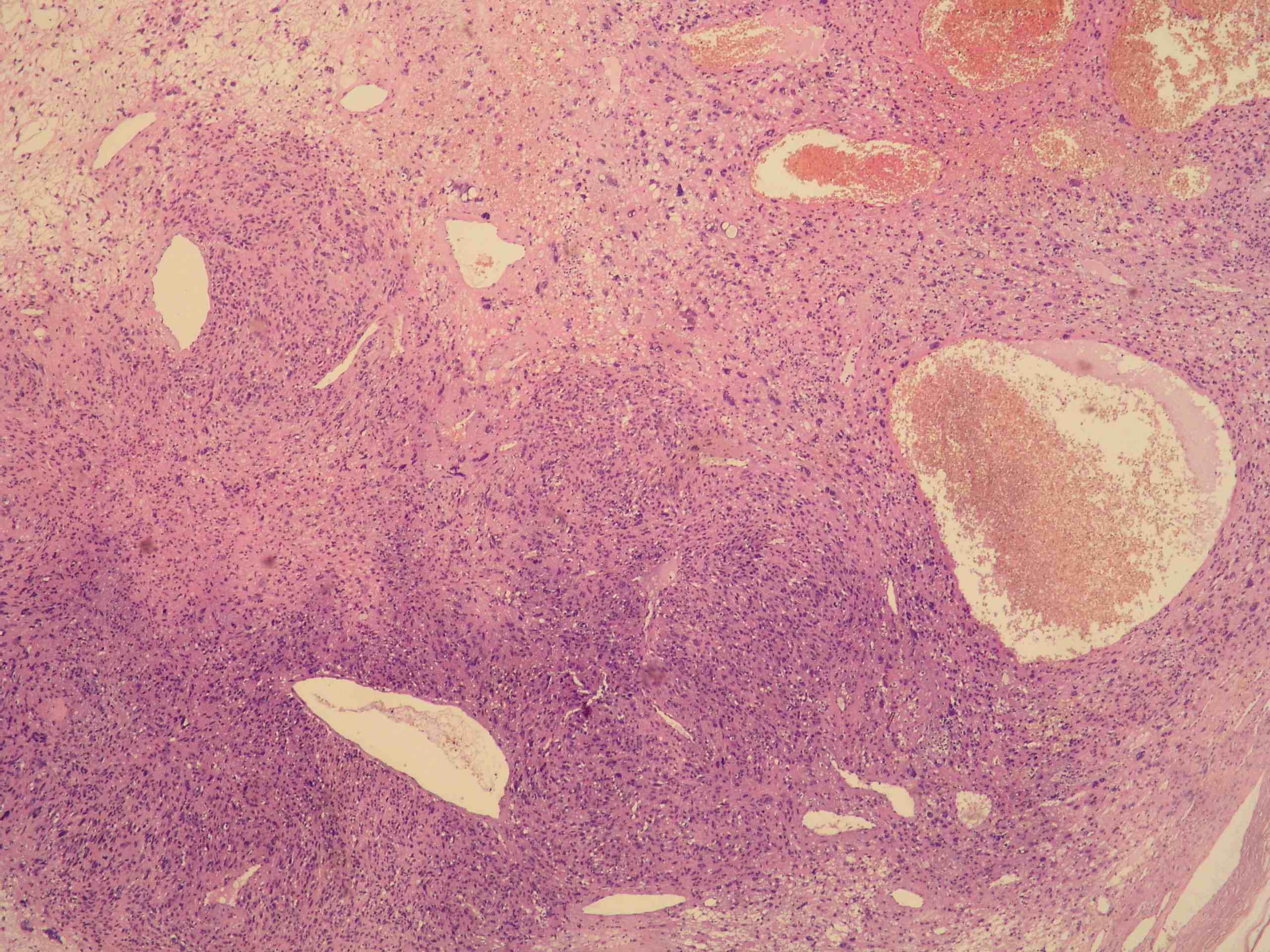
An 81 year old man had a painless tumor of his left great toe, which was excised. Macroscopically, the tumor was well circumscribed, measured 4 x 3 x 2.5 cm and was located in the subcutis.
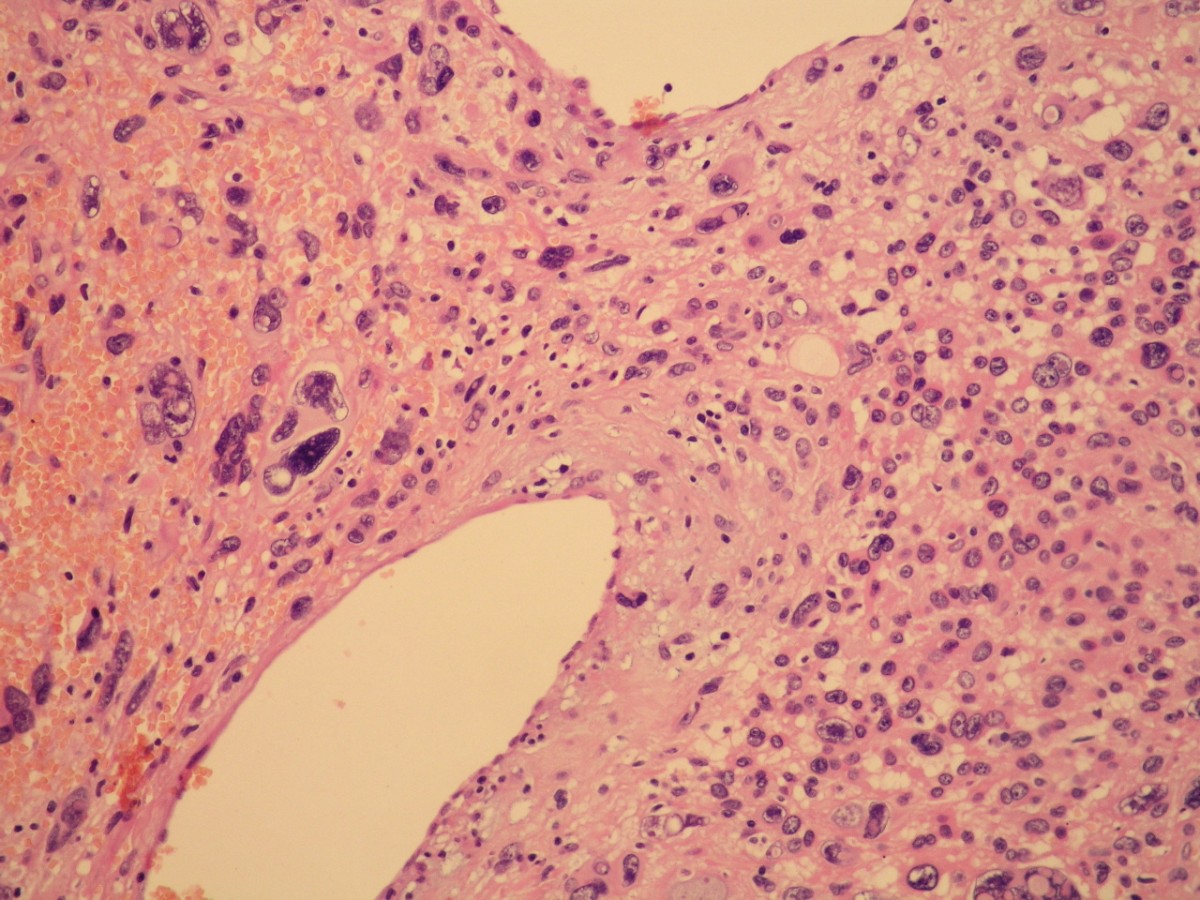
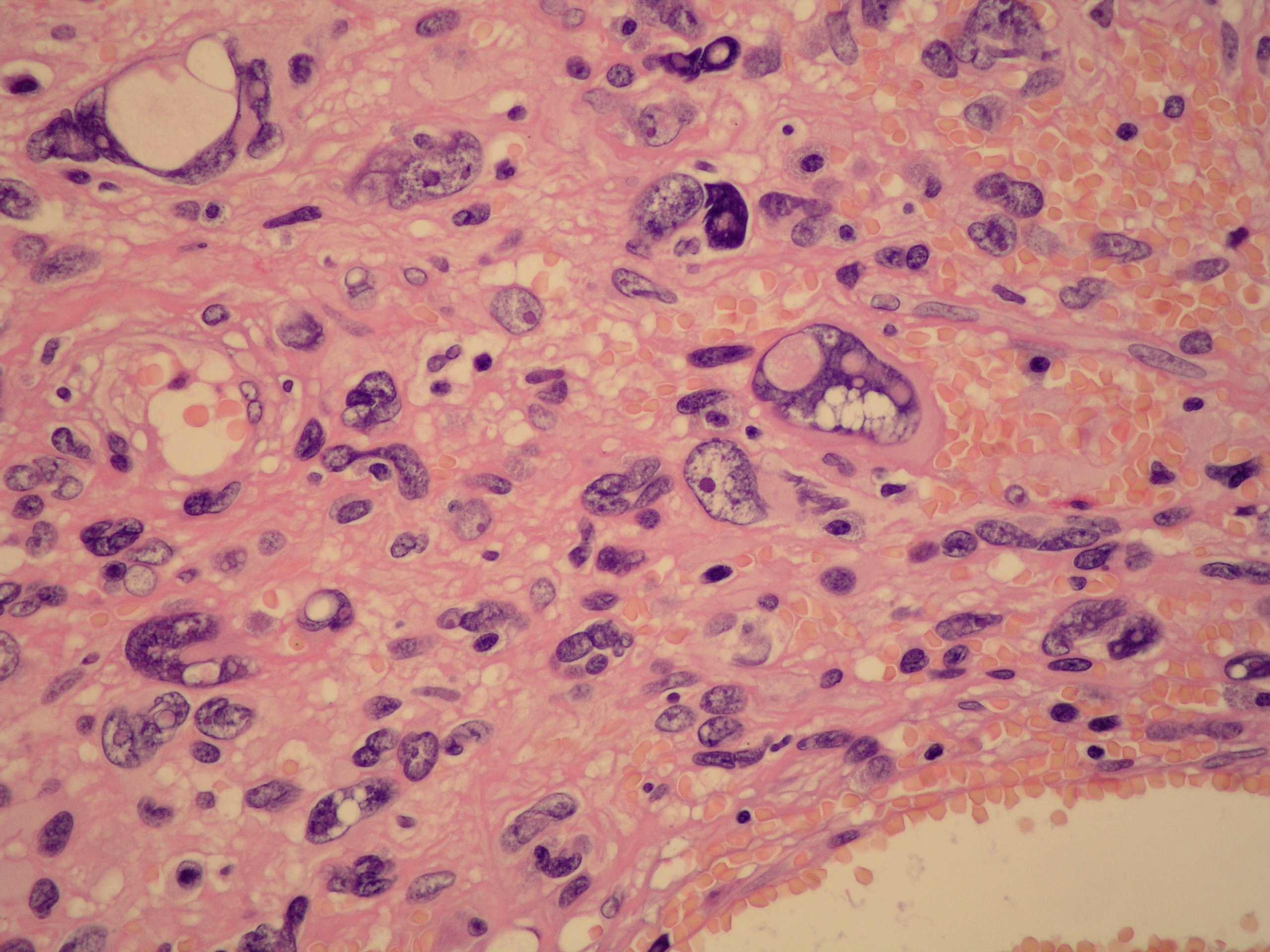
Microscopic images:





What is your diagnosis?
Diagnosis: Symplastic glomus tumor
Immunostains:
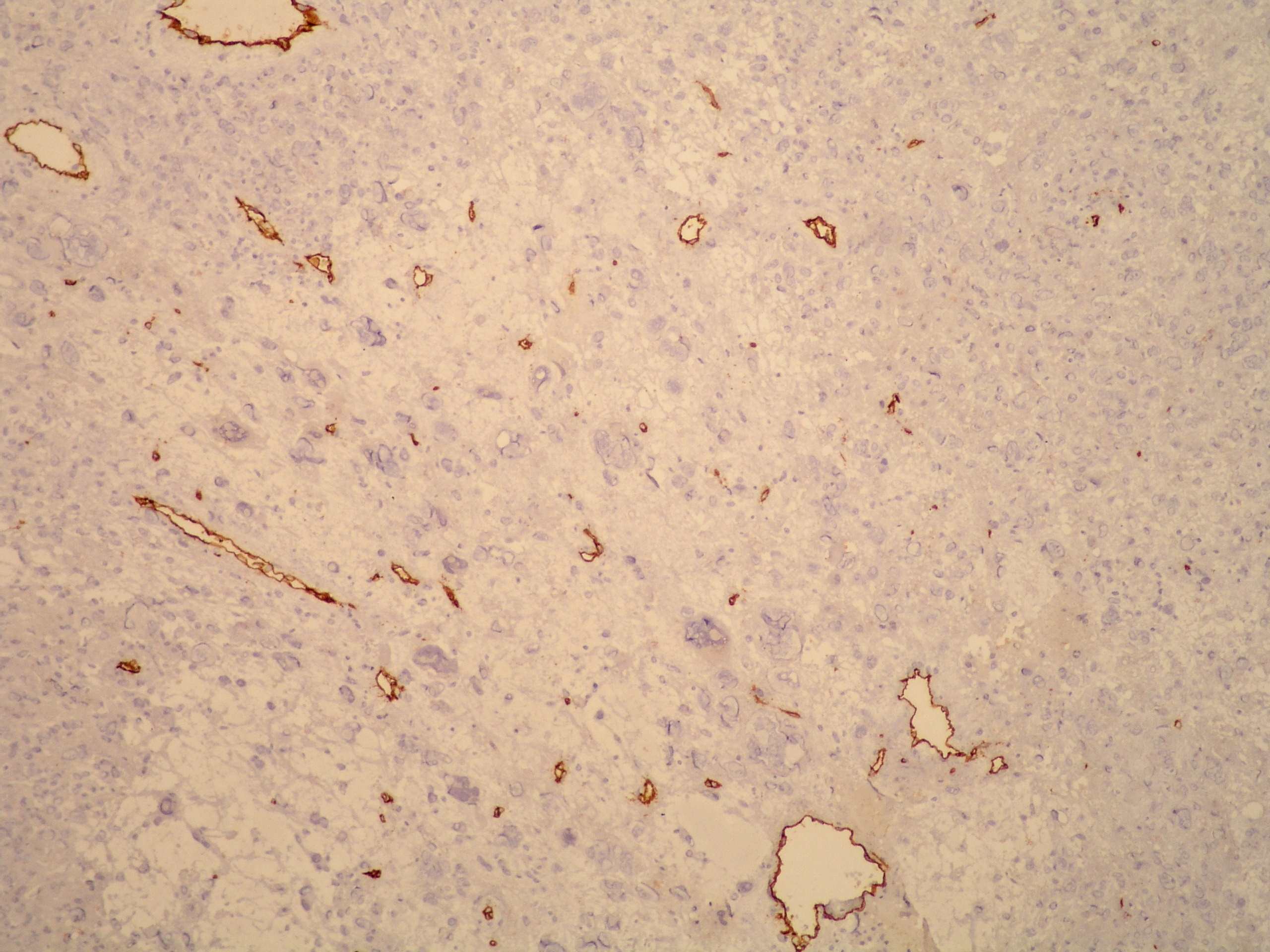
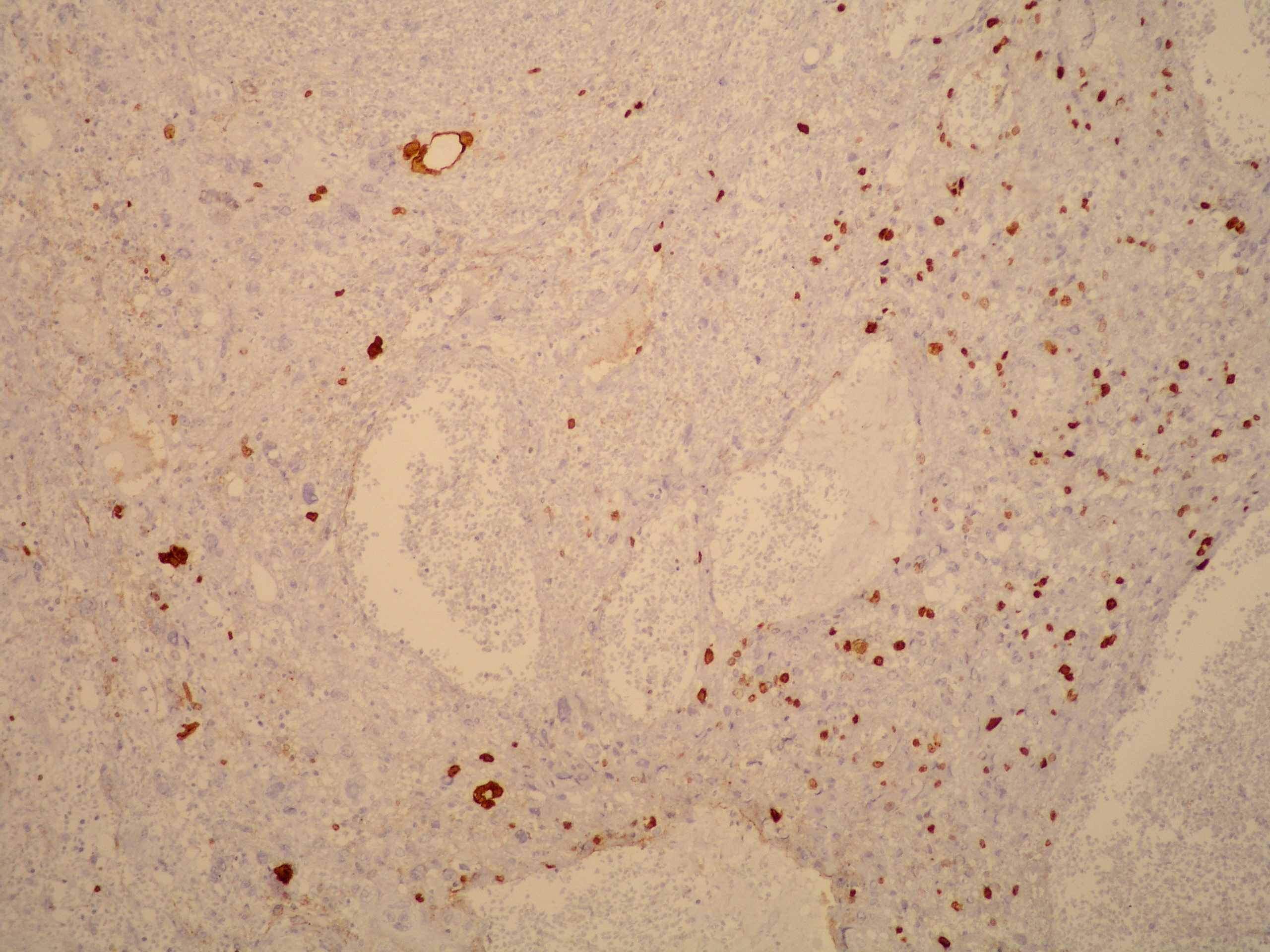
Left to right: CD34, Ki67
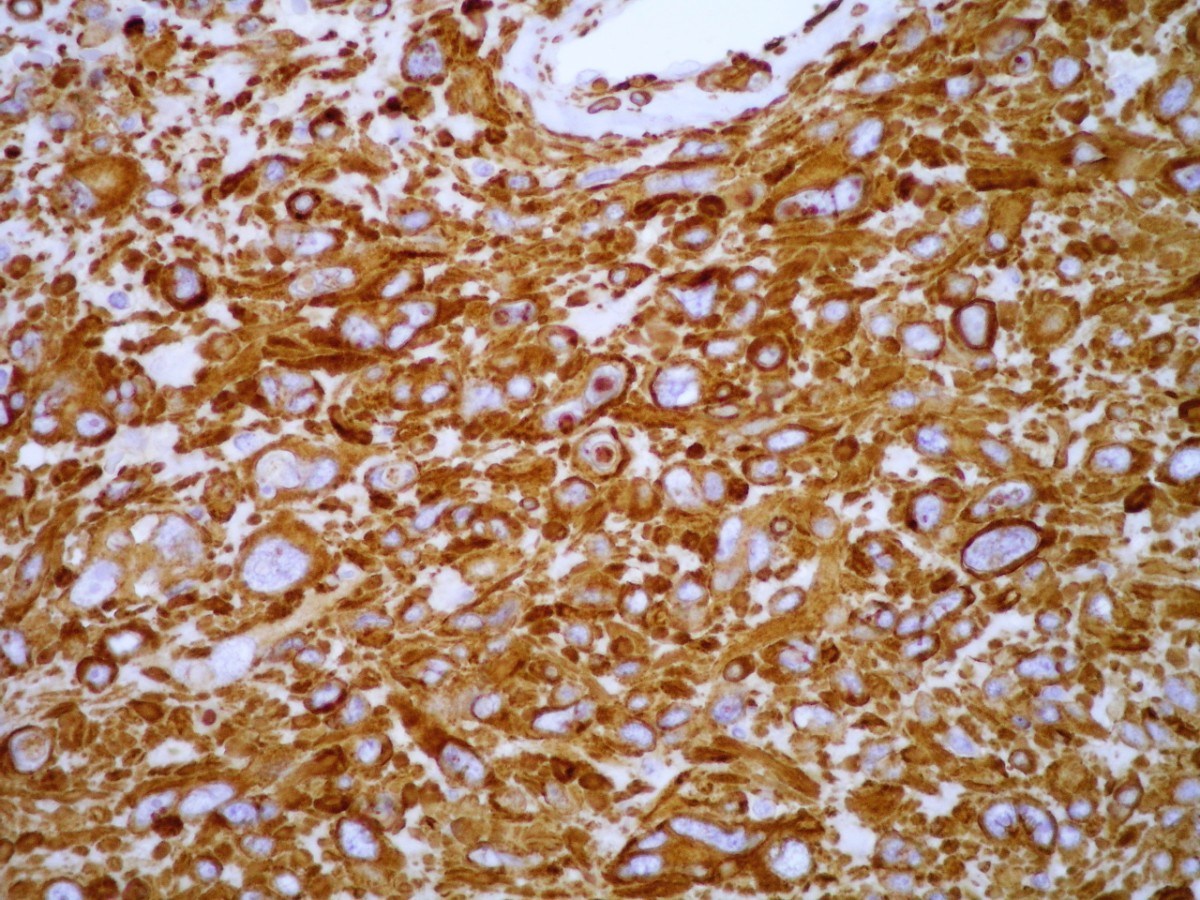
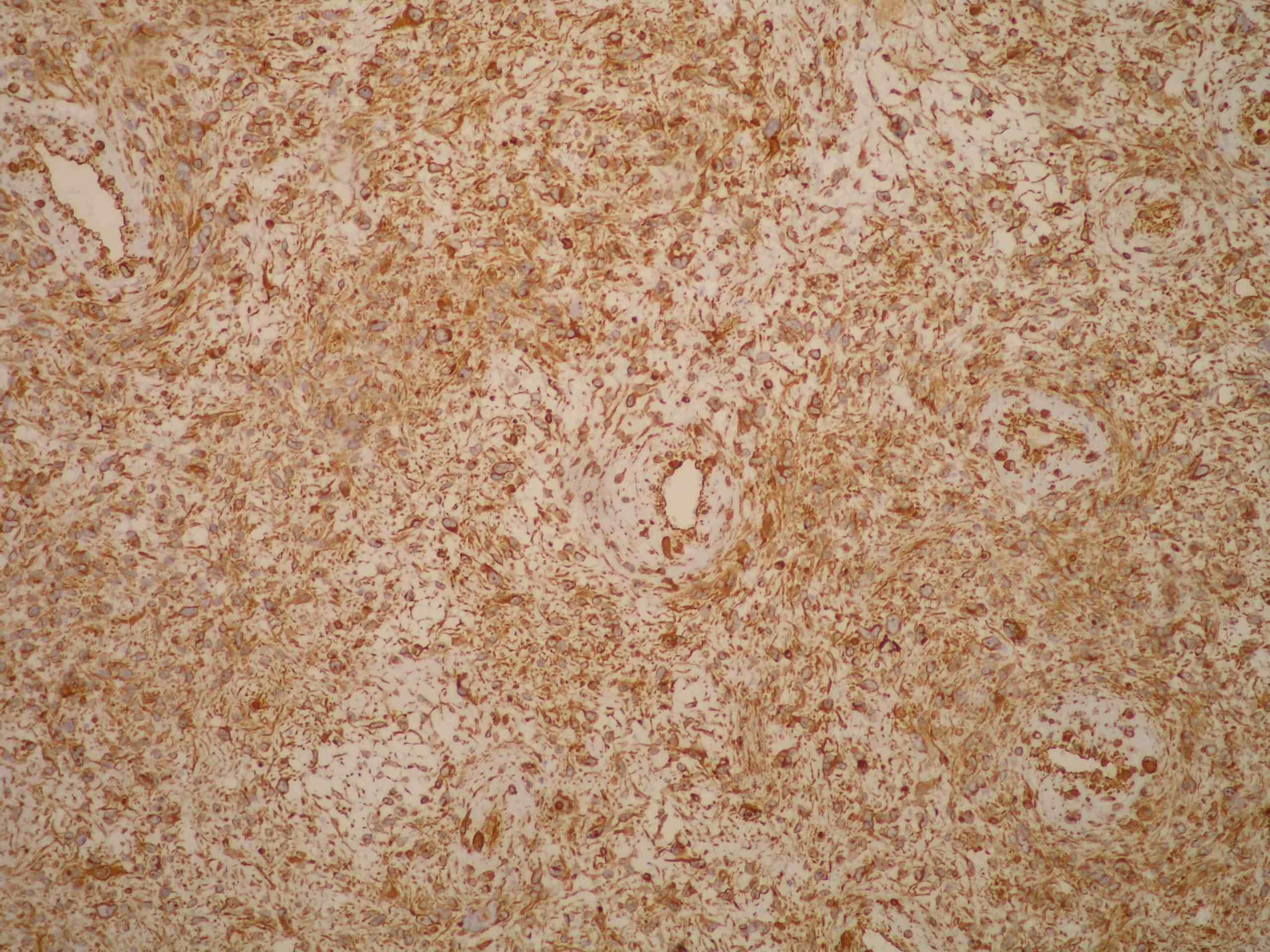
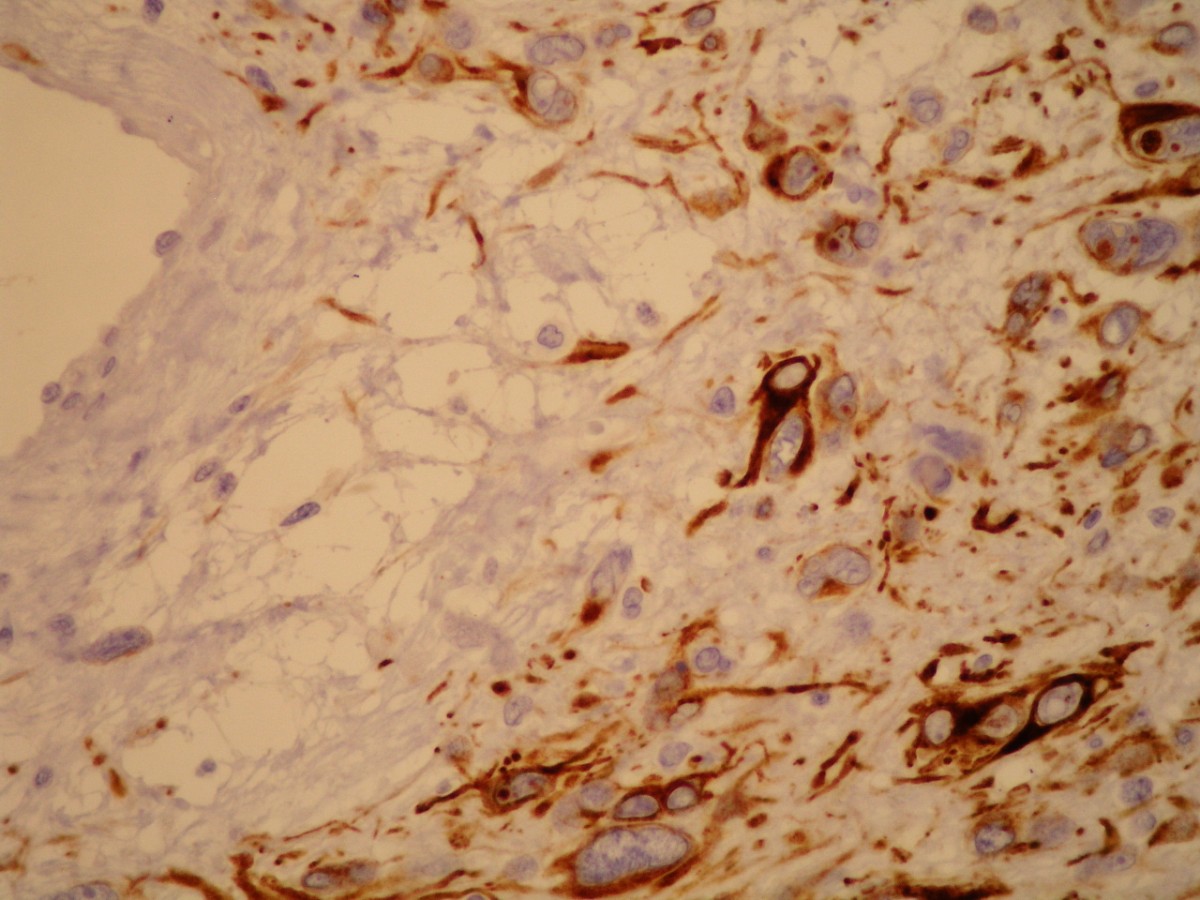
Left to right: smooth muscle actin, vimentin, desmin
Discussion:
The tumor was encapsulated and composed of solid sheets of cells separated by vessels of varying size and lined with normal appearing, CD34+ endothelium. The neoplastic cells showed pronounced nuclear pleomorphism, hyperchromasia and occasional intranuclear inclusions. Mitotic activity was sparse, up to 2 mitoses/50 HPF but the Ki67 proliferative rate was ~25%. There were no atypical mitotic figures but areas of necrosis were present. Tumor cells were diffusely immunoreactive for smooth muscle actin (SMA), vimentin and desmin.
Glomus tumors are neoplasms differentiating toward specialized cells found in the glomus body, a structure involved in thermoregulation (Arch Pathol Lab Med 2008;132:1448, Int J Surg Pathol 2011;19:499). Symplastic glomus tumors, first described in 1995 as epithelioid glomus tumors have marked nuclear atypia but no other criteria for malignancy (Hum Pathol 1995;26:1022). Less than 25 cases have been reported in the English literature (Am J Dermatopathol 2009;31:71).
The differential diagnosis includes malignant glomus tumor, which has metastatic potential (AJ Cutan Pathol 2009;36:1099). A comprehensive study defined malignant glomus tumors as having a deep location and size > 2 cm or atypical mitotic figures, or moderate to high nuclear grade and 5 or more mitotic figures/50 HPF (Am J Surg Pathol 2001;25:1).
Symplastic glomus tumors have benign behavior and excision is curative.