4 November 2011 - Case #222
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Drs. Andrea L. Wiens and Eyas M. Hattab, Indiana University School of Medicine (USA).
CancerTYPE ID is a standardized, objective molecular test based on the differential expression of 92 genes, that classifies tumors by matching the gene expression pattern of a patients tumor tissue to a database of known tumor types and histological subtypes.
CancerTYPE IDs database includes 2,206 tumors from multiple tumor banks, selected to provide broader and deeper representation of the heterogeneity of tumors. The 92-gene assay does not overlap with IHC markers, providing complementary data to standard tumor diagnosis.
CancerTYPE ID uses real-time reverse transcription polymerase chain reaction (RT-PCR). A very low copy number of RNA molecules can be detected, thus reducing the sample tissue required for testing. Testing is conducted and results are generated at bioTheranostics' CAP-accredited, CLIA-certified laboratory.
For more information, click here.Advertisement
Case #222
Clinical history:
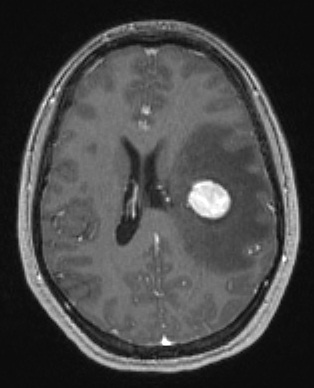
An 18 year old woman, ~19 weeks pregnant, presented with a new onset seizure, and was found to have a left frontal mass within the white matter, ~4 cm beneath the cortical surface by imaging. She underwent craniotomy and surgical resection.
Radiology image:
Microscopic images:

What is your diagnosis?
Diagnosis: Alveolar soft part sarcoma
Immunostains:

Discussion:
Alveolar soft part sarcoma (ASPS) is an exceedingly rare soft tissue sarcoma which occurs primarily in children and young adults. This patient had a prior diagnosis of ASPS of the tongue at age 8 which was treated with surgery and chemotherapy. Within one year of her initial diagnosis, she developed over 20 pulmonary nodules. She recently presented to the emergency department after a focal seizure, which resulted in transient right upper extremity numbness, right facial droop and dysphasia. Neuroimaging (axial T1 with contrast) revealed a 1.8 cm mass in the left frontal-parietal lobe region (posterior corona radiata) with associated vasogenic edema and a 6 mm left to right midline shift. Imaging findings were felt to be consistent with metastatic disease. The brain mass was surgically resected.
ASPS is a slow growing, painless malignancy of uncertain histogenesis which is frequently metastatic at presentation but has an overall indolent course with long term survival (Goldblum: Enzinger and Weiss's Soft Tissue Tumors, 5th Edition, 2008). ASPS commonly arises in deep soft tissues of the lower extremities of adults, while in children it is more common in the head and neck region, particularly in the orbit and tongue. Metastases are most common to regional lymph nodes with hematogeneous spread to the lungs and brain. Intracranial metastases have been reported to be observed only in the presence of extracranial metastatic disease and never in the absence of pulmonary metastatic disease (Cancer 2001;91:585).
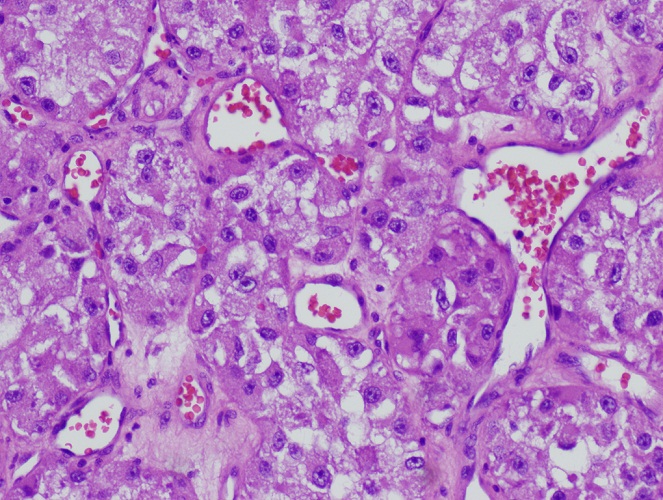
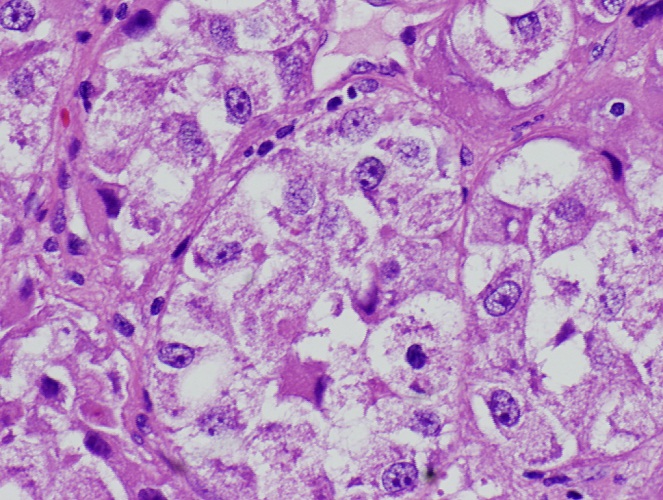
Classic histologic features of ASPS include an alveolar growth pattern characterized by dense fibrous septae of variable thickness which divide the tumor cells into large, variably sized clusters. These clusters are further divided by delicate vasculature into smaller nests of polygonal tumor cells with abundant finely granular eosinophilic to cleared cytoplasm and large nuclei with prominent nucleoli. Tumor cells may contain characteristic intracytoplasmic periodic acid-Schiff (PAS) positive, diastase resistant rod shaped crystals. PAS staining also reveals abundant intracytoplasmic glycogen.
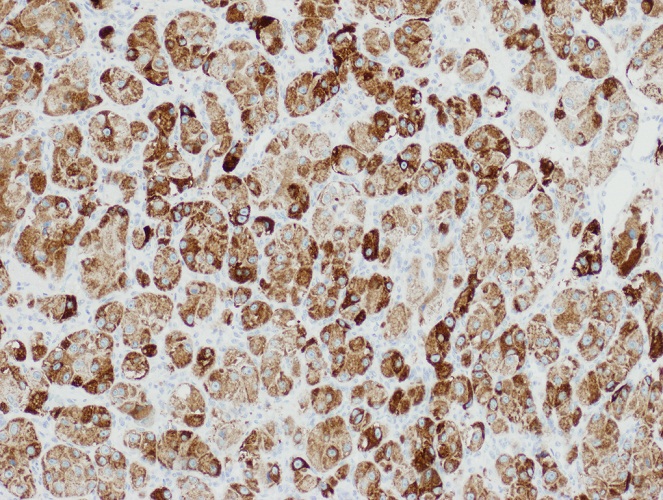
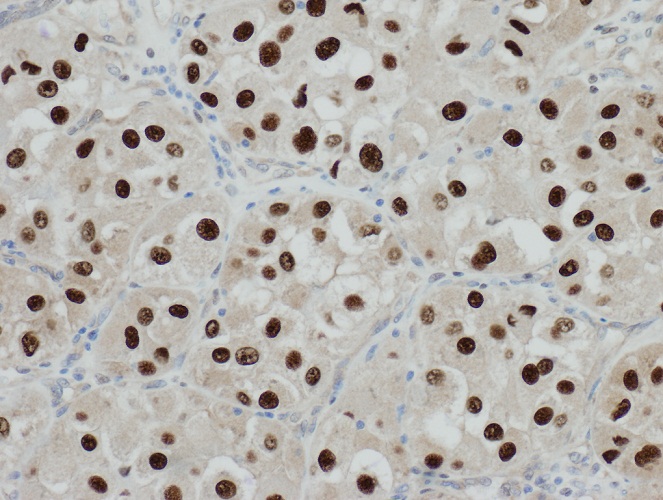
Immunohistochemically, tumor cells demonstrate aberrant nuclear positivity for TFE3 due to a defining chromosomal translocation [der(17)t(X;17)(p11.2;q25)] resulting in a fusion of the TFE3 gene from Xp11.2 to the ASPL gene on 17q25 (Oncogene 2001;20:48). The ASPL::TFE3 fusion protein localizes to the nucleus and acts as an aberrant transcription factor. Tumor cells also tend to demonstrate positive cytoplasmic staining for MyoD1, rather than nuclear staining, a feature which at first was thought to support a myogenic origin of the tumor but has not been substantiated by further investigations (Arch Pathol Lab Med 1999;123:503).
The differential diagnosis of ASPS includes:
Standard treatment is surgical resection, and tumor size and resection margin status are 2 of the most important factors for prognosis. Smaller tumors (< 5 cm) and tumors with negative resection margins (absence of tumor within 1 mm from margin) have better overall survival and local recurrence free survival (Ann Surg Oncol 2010;17:3229). Surgical resection of solitary brain metastases can result in a continued indolent course of disease and prolonged survival (J Neurooncol 1995;25:161).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Drs. Andrea L. Wiens and Eyas M. Hattab, Indiana University School of Medicine (USA).
CancerTYPE ID is a standardized, objective molecular test based on the differential expression of 92 genes, that classifies tumors by matching the gene expression pattern of a patients tumor tissue to a database of known tumor types and histological subtypes.
CancerTYPE IDs database includes 2,206 tumors from multiple tumor banks, selected to provide broader and deeper representation of the heterogeneity of tumors. The 92-gene assay does not overlap with IHC markers, providing complementary data to standard tumor diagnosis.
CancerTYPE ID uses real-time reverse transcription polymerase chain reaction (RT-PCR). A very low copy number of RNA molecules can be detected, thus reducing the sample tissue required for testing. Testing is conducted and results are generated at bioTheranostics' CAP-accredited, CLIA-certified laboratory.
For more information, click here.
Website news:
(1) We are looking for more cases of the weeks. We are also looking for authors with expertise in AP computer systems and LIS systems, to add content to these pages. Click here for more information.
(2) Our Feature Page for November 2011 highlights Consumable Lab Products / Clinical Lab Analyzers, and includes Biogenex, Leica Microsystems, Sakura Finetek USA and Ventana Medical.
(3) Last month, we again had record traffic, with 359,051 visits (85 million "hits"). We continue to update topics daily. We update each chapter as we get topics back from reviewers, so the topics in a chapter are not all updated at the same time.
Visit and follow our Blog to see recent updates to the website.
(1) We are looking for more cases of the weeks. We are also looking for authors with expertise in AP computer systems and LIS systems, to add content to these pages. Click here for more information.
(2) Our Feature Page for November 2011 highlights Consumable Lab Products / Clinical Lab Analyzers, and includes Biogenex, Leica Microsystems, Sakura Finetek USA and Ventana Medical.
(3) Last month, we again had record traffic, with 359,051 visits (85 million "hits"). We continue to update topics daily. We update each chapter as we get topics back from reviewers, so the topics in a chapter are not all updated at the same time.
Visit and follow our Blog to see recent updates to the website.
Case #222
Clinical history:
An 18 year old woman, ~19 weeks pregnant, presented with a new onset seizure, and was found to have a left frontal mass within the white matter, ~4 cm beneath the cortical surface by imaging. She underwent craniotomy and surgical resection.
Radiology image:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Alveolar soft part sarcoma
Immunostains:
MyoD1
PASD
TFE3
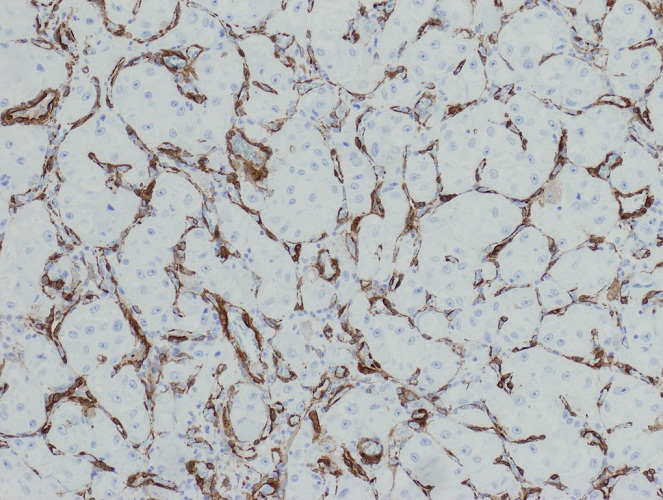
Vimentin
Discussion:
Alveolar soft part sarcoma (ASPS) is an exceedingly rare soft tissue sarcoma which occurs primarily in children and young adults. This patient had a prior diagnosis of ASPS of the tongue at age 8 which was treated with surgery and chemotherapy. Within one year of her initial diagnosis, she developed over 20 pulmonary nodules. She recently presented to the emergency department after a focal seizure, which resulted in transient right upper extremity numbness, right facial droop and dysphasia. Neuroimaging (axial T1 with contrast) revealed a 1.8 cm mass in the left frontal-parietal lobe region (posterior corona radiata) with associated vasogenic edema and a 6 mm left to right midline shift. Imaging findings were felt to be consistent with metastatic disease. The brain mass was surgically resected.
ASPS is a slow growing, painless malignancy of uncertain histogenesis which is frequently metastatic at presentation but has an overall indolent course with long term survival (Goldblum: Enzinger and Weiss's Soft Tissue Tumors, 5th Edition, 2008). ASPS commonly arises in deep soft tissues of the lower extremities of adults, while in children it is more common in the head and neck region, particularly in the orbit and tongue. Metastases are most common to regional lymph nodes with hematogeneous spread to the lungs and brain. Intracranial metastases have been reported to be observed only in the presence of extracranial metastatic disease and never in the absence of pulmonary metastatic disease (Cancer 2001;91:585).
Classic histologic features of ASPS include an alveolar growth pattern characterized by dense fibrous septae of variable thickness which divide the tumor cells into large, variably sized clusters. These clusters are further divided by delicate vasculature into smaller nests of polygonal tumor cells with abundant finely granular eosinophilic to cleared cytoplasm and large nuclei with prominent nucleoli. Tumor cells may contain characteristic intracytoplasmic periodic acid-Schiff (PAS) positive, diastase resistant rod shaped crystals. PAS staining also reveals abundant intracytoplasmic glycogen.
Immunohistochemically, tumor cells demonstrate aberrant nuclear positivity for TFE3 due to a defining chromosomal translocation [der(17)t(X;17)(p11.2;q25)] resulting in a fusion of the TFE3 gene from Xp11.2 to the ASPL gene on 17q25 (Oncogene 2001;20:48). The ASPL::TFE3 fusion protein localizes to the nucleus and acts as an aberrant transcription factor. Tumor cells also tend to demonstrate positive cytoplasmic staining for MyoD1, rather than nuclear staining, a feature which at first was thought to support a myogenic origin of the tumor but has not been substantiated by further investigations (Arch Pathol Lab Med 1999;123:503).
The differential diagnosis of ASPS includes:
- Granular cell tumor: S100+; MyoD1 and TFE3 negative, no crystals with PASD
- Alveolar rhabdomyosarcoma: positive muscle markers; p63 staining of Z bands (Mod Pathol 2011;24:1320)
- Paraganglioma: zellballen pattern; positive neuroendocrine markers (Fletcher: Diagnostic Histopathology of Tumors, 3rd Edition, 2007)
- Metastatic renal cell carcinoma: EMA+, CD10+
Standard treatment is surgical resection, and tumor size and resection margin status are 2 of the most important factors for prognosis. Smaller tumors (< 5 cm) and tumors with negative resection margins (absence of tumor within 1 mm from margin) have better overall survival and local recurrence free survival (Ann Surg Oncol 2010;17:3229). Surgical resection of solitary brain metastases can result in a continued indolent course of disease and prolonged survival (J Neurooncol 1995;25:161).