8 September 2011 - Case #216
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Bassma M. El Sabaa, Alexandria Faculty of Medicine, Egypt.

Case #216
Clinical history:
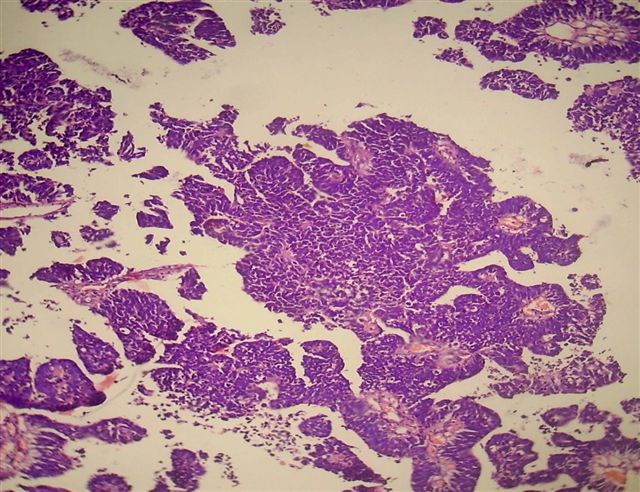
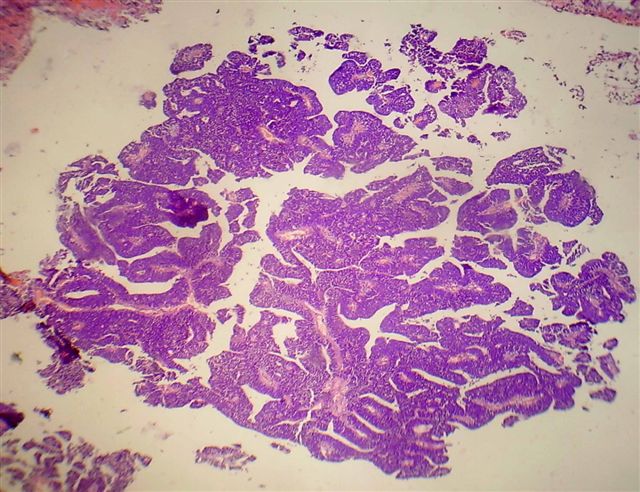
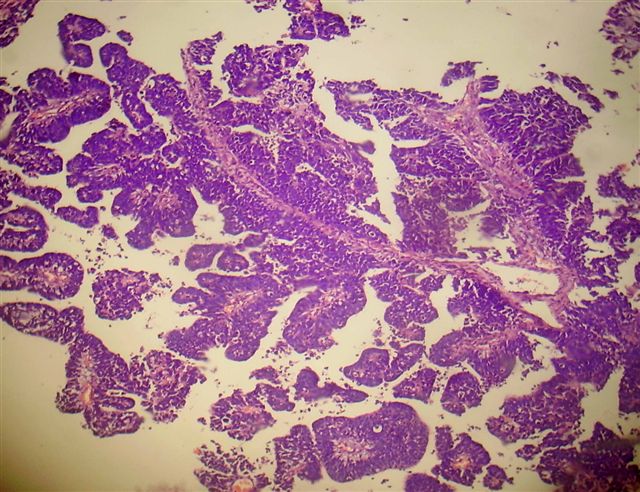
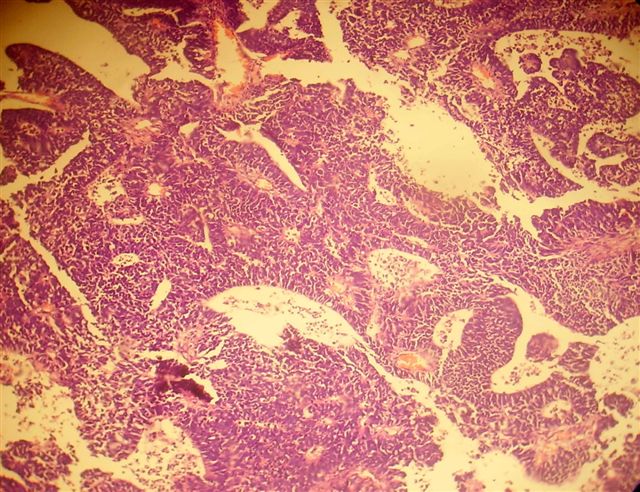
A 28 month old girl had a 2 month history of squinting, vomiting and ataxia. MRI showed lesions in the fourth ventricle and the left cerebellar hemisphere, which were excised.
Microscopic images:

What is your diagnosis?
Diagnosis: Medulloepithelioma
Immunostains:
Discussion:
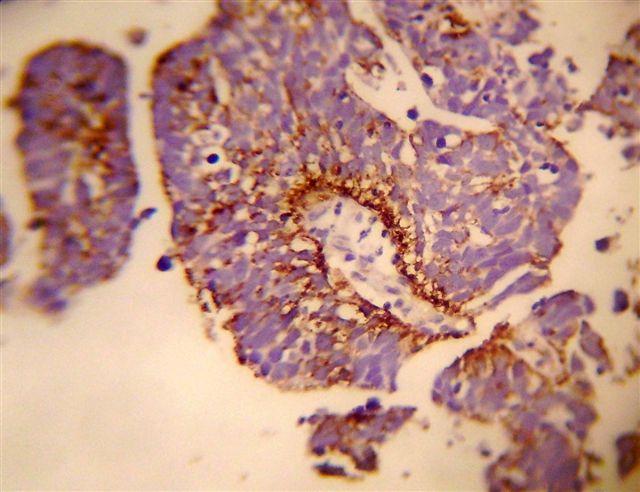
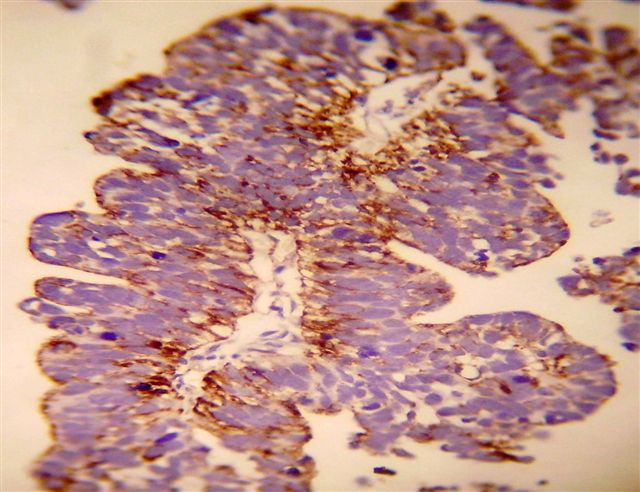
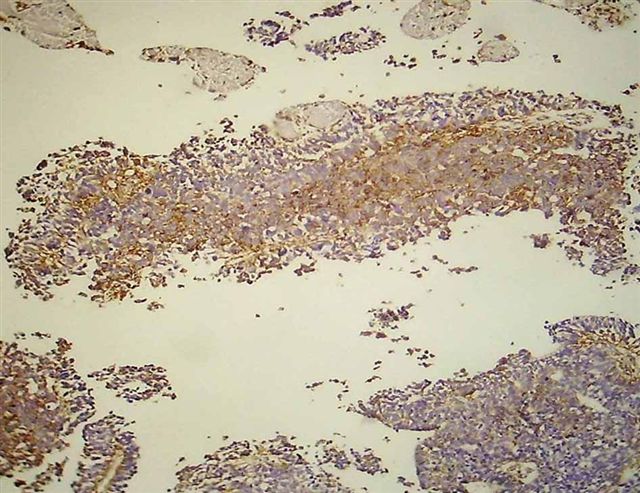
Immunostains were negative for cytokeratin, EMA and GFAP and positive for nestin and vimentin.
Medulloepithelioma is a rare, high grade (WHO grade IV), neoplasm containing epithelium resembling the embryonic neural tube. Most cases occur in the first 5 years of life, either supra or infratentorially. It may also occur in the ciliary body / optic disc or elsewhere in the body (Hum Pathol 2011;42:2047). Tumors are typically large, causing increased intracranial pressure or mass type symptoms (Burger: Tumors of the Central Nervous System, 1st Edition, 2007).
Grossly, tumors are typically solid, gray-tan and soft, with variable cystic changes, hemorrhage, fibrosis or calcification. Classic histologic features are glands or tubules of primitive appearing epithelium that resembles the epithelium of the developing brain, with pseudostratification, small cytoplasmic blebs and mitotic figures. The outer surface has a well defined basement membrane, and the internal side has an ill defined pseudomembrane. Other regions may have more undifferentiated tumor.
The basement membrane is strongly positive for PAS, type IV collagen and nestin. Tumor cells are immunoreactive for vimentin but negative for keratin, S100, GFAP and synaptophysin (Pediatr Pathol Lab Med 1997;17:913).
The differential diagnosis includes:
Most patients die within 1 year of diagnosis, although long term survival has been reported (J Neurosurg Pediatr 2008;2:339). In the above case, the patient received chemotherapy and is alive and well one year postdiagnosis.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Bassma M. El Sabaa, Alexandria Faculty of Medicine, Egypt.
Website news:
(1) Visit us at CAP '11 at Booth #328, towards the back near the posters, left hand side (as you enter).
(2) Our Feature Page for September 2011 highlights Antibodies, and includes Biogenex, Covance, Epitomics and Leica Microsystems.
(3) We are looking for a reviewer for our new CNS-nontumor chapter. Sections include normal / embryology, malformations, infections, demyelinating disorders, dementia, stroke / hemorrhage. Email us if interested.
(4) In August 2011, we had record traffic of 307,303 visits. Thanks to all of our supporters.
Visit and follow our Blog to see recent updates to the website.
(1) Visit us at CAP '11 at Booth #328, towards the back near the posters, left hand side (as you enter).
(2) Our Feature Page for September 2011 highlights Antibodies, and includes Biogenex, Covance, Epitomics and Leica Microsystems.
(3) We are looking for a reviewer for our new CNS-nontumor chapter. Sections include normal / embryology, malformations, infections, demyelinating disorders, dementia, stroke / hemorrhage. Email us if interested.
(4) In August 2011, we had record traffic of 307,303 visits. Thanks to all of our supporters.
Visit and follow our Blog to see recent updates to the website.
Case #216
Clinical history:
A 28 month old girl had a 2 month history of squinting, vomiting and ataxia. MRI showed lesions in the fourth ventricle and the left cerebellar hemisphere, which were excised.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Medulloepithelioma
Immunostains:
Nestin+
Vimentin+
Discussion:
Immunostains were negative for cytokeratin, EMA and GFAP and positive for nestin and vimentin.
Medulloepithelioma is a rare, high grade (WHO grade IV), neoplasm containing epithelium resembling the embryonic neural tube. Most cases occur in the first 5 years of life, either supra or infratentorially. It may also occur in the ciliary body / optic disc or elsewhere in the body (Hum Pathol 2011;42:2047). Tumors are typically large, causing increased intracranial pressure or mass type symptoms (Burger: Tumors of the Central Nervous System, 1st Edition, 2007).
Grossly, tumors are typically solid, gray-tan and soft, with variable cystic changes, hemorrhage, fibrosis or calcification. Classic histologic features are glands or tubules of primitive appearing epithelium that resembles the epithelium of the developing brain, with pseudostratification, small cytoplasmic blebs and mitotic figures. The outer surface has a well defined basement membrane, and the internal side has an ill defined pseudomembrane. Other regions may have more undifferentiated tumor.
The basement membrane is strongly positive for PAS, type IV collagen and nestin. Tumor cells are immunoreactive for vimentin but negative for keratin, S100, GFAP and synaptophysin (Pediatr Pathol Lab Med 1997;17:913).
The differential diagnosis includes:
- Choroid plexus carcinoma: papillary epithelium, S100+, cytokeratin+
- Immature teratoma: has other fetal appearing tissues, PLAP+, possibly AFP+ or CEA+
- Ependymoblastoma: has rosettes with a lumen but without an outer or inner membrane
Most patients die within 1 year of diagnosis, although long term survival has been reported (J Neurosurg Pediatr 2008;2:339). In the above case, the patient received chemotherapy and is alive and well one year postdiagnosis.