10 August 2011 - Case #213
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Professor David Cohen, Herzliya Medical Center (Israel).

CancerTYPE ID is a standardized, objective molecular test based on the differential expression of 92 genes, that classifies tumors by matching the gene expression pattern of a patients tumor tissue to a database of known tumor types and histological subtypes.
CancerTYPE IDs database includes 2,206 tumors from multiple tumor banks, selected to provide broader and deeper representation of the heterogeneity of tumors. The 92-gene assay does not overlap with IHC markers, providing complementary data to standard tumor diagnosis.
CancerTYPE ID uses real-time reverse transcription polymerase chain reaction (RT-PCR). A very low copy number of RNA molecules can be detected, thus reducing the sample tissue required for testing. Testing is conducted and results are generated at bioTheranostics' CAP-accredited, CLIA-certified laboratory.
Advertisement
Case #213
Clinical history:
A 48 year old man had prolonged diarrhea, with a clinical impression of inflammatory bowel disease or microscopic colitis. A colonic biopsy was obtained.
Microscopic images:

What is your diagnosis?
Diagnosis: Intestinal spirochetosis
Discussion:
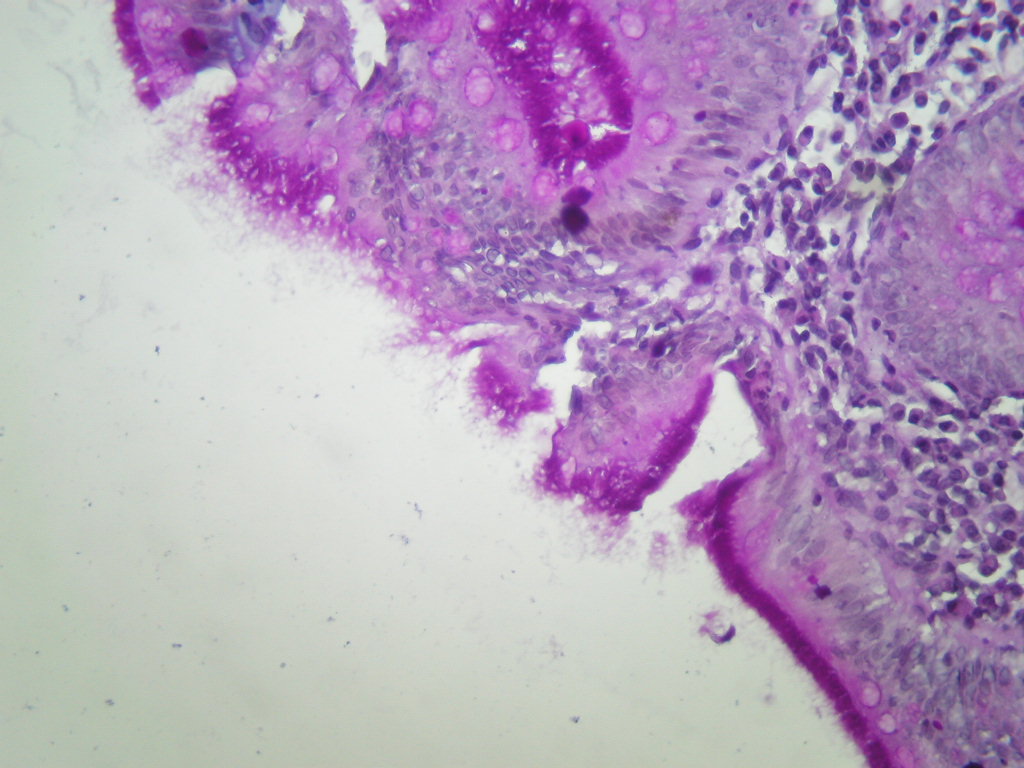
Sections show colonic mucosal biopsies with a lamina propria that is mildly expanded by inflammatory cells including eosinophils and mononuclear inflammatory cells. The mucosal glands appear normal under low power but on high power the luminal surface shows a blue fringe, which is strongly positive with PAS where filamentous organisms are present.
Intestinal spirochetosis is colonization of the colon by relatively nonpathogenic spirochetes. It is seen in 3 - 10% of normal patients, and is associated with anal intercourse, HIV and lower socioeconomic conditions (Ger Med Sci 2010;8:Doc01). It may occur in children, who often have abdominal symptoms (Pediatr Dev Pathol 2010;13:471, Am J Clin Pathol 2003;120:828). Intestinal spirochetosis may cause persistent diarrhea, possibly due to blunting and destruction of microvilli (Am J Clin Pathol 1986;86:679).
As in this case, histology shows an accentuation of the luminal border by spirochetes, which produce a blue line on H&E between the microvilli of the covering epithelium (Pathologe 2003;24:192). The spirochetes are accentuated by silver stains (Warthin-Starry, Dieterle), as well as PAS, Giemsa and Alcian blue (pH 2.5). There is usually minimal inflammation present.
Electron microscopy shows long coiled bacteria adherent to the microvilli (Ger Med Sci 2010;8:Doc01).
Symptomatic patients are treated with metronidazole.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Professor David Cohen, Herzliya Medical Center (Israel).
CancerTYPE ID is a standardized, objective molecular test based on the differential expression of 92 genes, that classifies tumors by matching the gene expression pattern of a patients tumor tissue to a database of known tumor types and histological subtypes.
CancerTYPE IDs database includes 2,206 tumors from multiple tumor banks, selected to provide broader and deeper representation of the heterogeneity of tumors. The 92-gene assay does not overlap with IHC markers, providing complementary data to standard tumor diagnosis.
CancerTYPE ID uses real-time reverse transcription polymerase chain reaction (RT-PCR). A very low copy number of RNA molecules can be detected, thus reducing the sample tissue required for testing. Testing is conducted and results are generated at bioTheranostics' CAP-accredited, CLIA-certified laboratory.
Website news:
(1) As we begin our 11th year, we thank you for your support. This year, we plan to increase the frequency of chapter updates, add more images and videos. Let us know if you have any other comments or suggestions.
(2) We are looking for reviewers for part / all of these chapters: Coagulation, Salivary Glands, Stains, Uterus; also Fallopian Tubes, Lung-tumor, Ureters, Urethra, Vagina, Vulva.
(3) We have updated the Skin-nontumor chapter based on reviews by Ha Kirsten Do, M.D., IUPUI; Mowafak Hamodat, MB.CH.B, MSc., FRCPC, Eastern Health, St. Johns (Canada); Nat Pernick, M.D., PathologyOutlines.com, Inc. and Cecilia Rosales, M.D., Baylor College. Over the next several months, we will be adding more images and references to these topics.
Visit and follow our Blog to see recent updates to the website.
(1) As we begin our 11th year, we thank you for your support. This year, we plan to increase the frequency of chapter updates, add more images and videos. Let us know if you have any other comments or suggestions.
(2) We are looking for reviewers for part / all of these chapters: Coagulation, Salivary Glands, Stains, Uterus; also Fallopian Tubes, Lung-tumor, Ureters, Urethra, Vagina, Vulva.
(3) We have updated the Skin-nontumor chapter based on reviews by Ha Kirsten Do, M.D., IUPUI; Mowafak Hamodat, MB.CH.B, MSc., FRCPC, Eastern Health, St. Johns (Canada); Nat Pernick, M.D., PathologyOutlines.com, Inc. and Cecilia Rosales, M.D., Baylor College. Over the next several months, we will be adding more images and references to these topics.
Visit and follow our Blog to see recent updates to the website.
Case #213
Clinical history:
A 48 year old man had prolonged diarrhea, with a clinical impression of inflammatory bowel disease or microscopic colitis. A colonic biopsy was obtained.
Microscopic images:
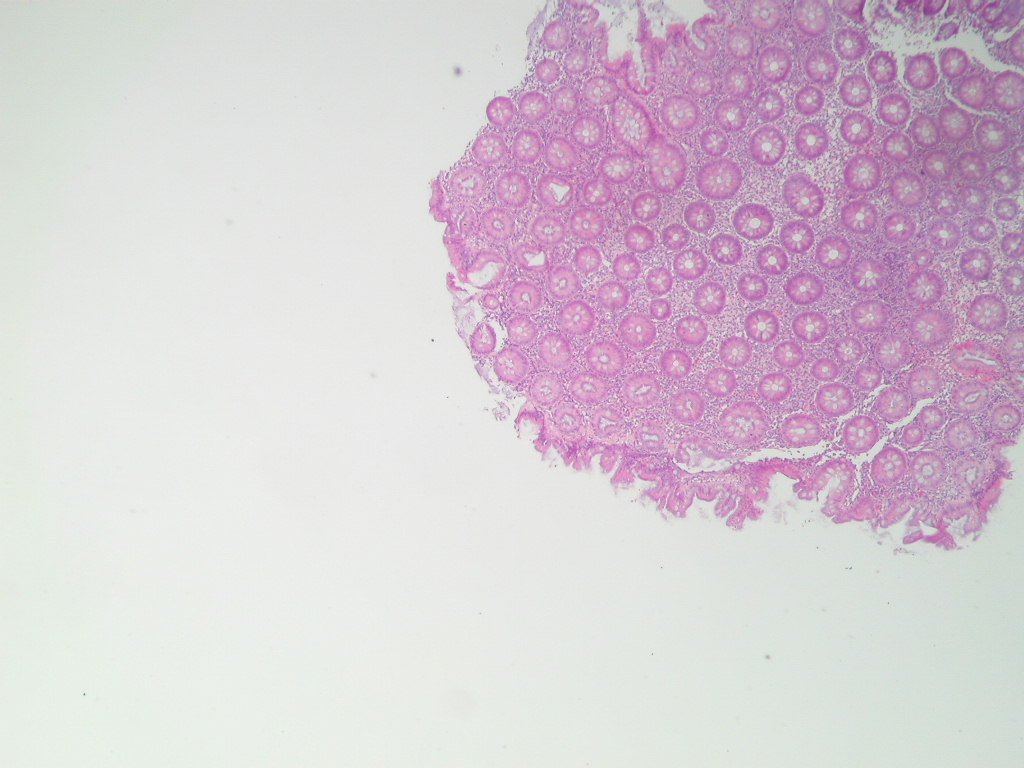
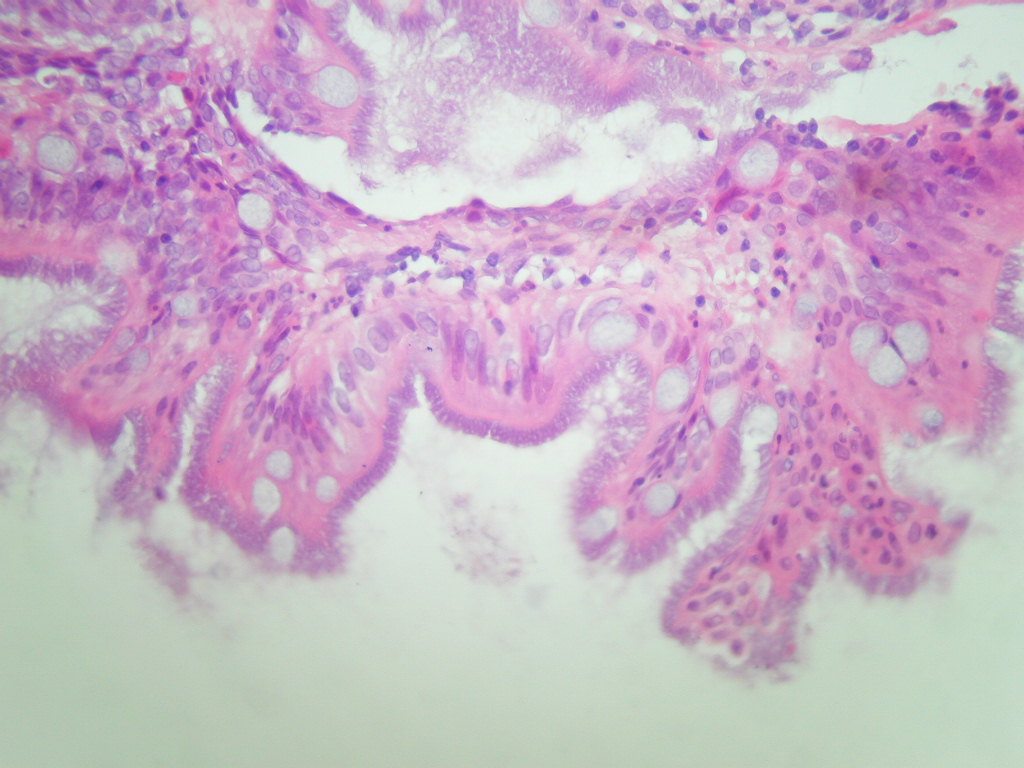
H&E
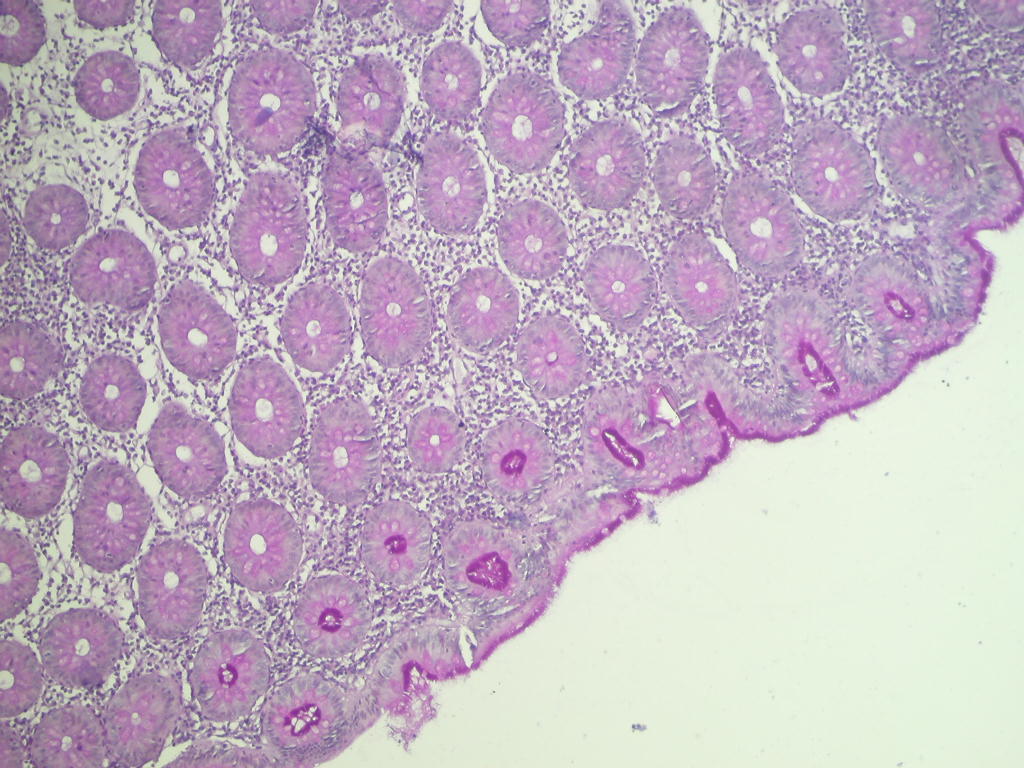
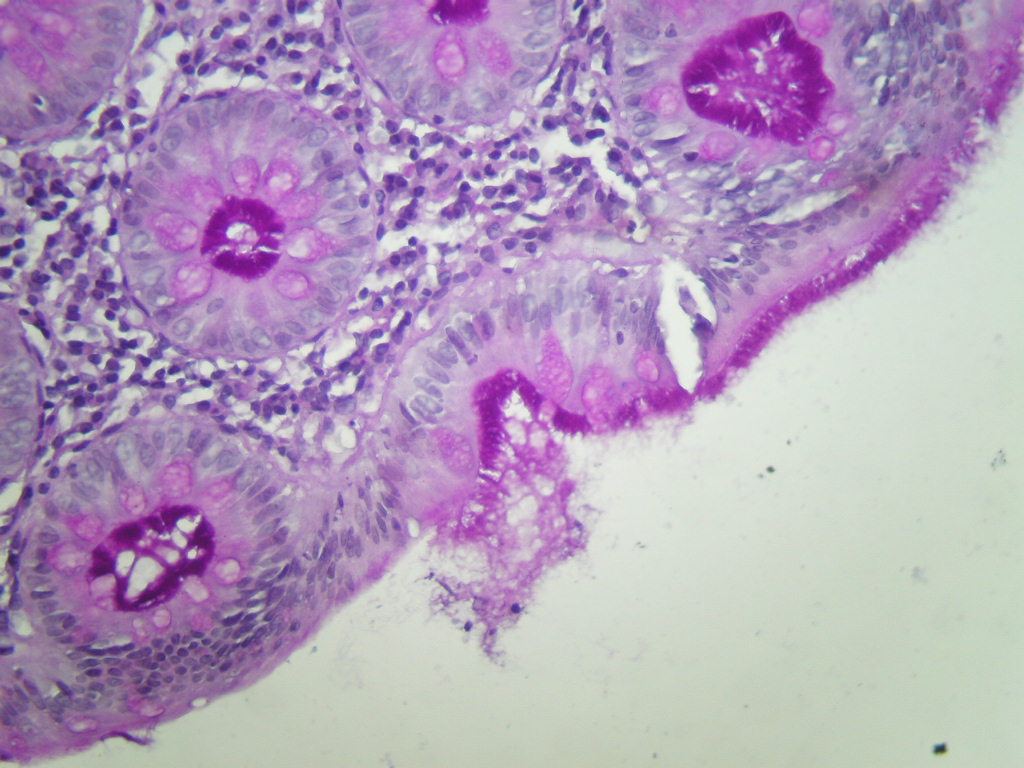
PAS
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Intestinal spirochetosis
Discussion:
Sections show colonic mucosal biopsies with a lamina propria that is mildly expanded by inflammatory cells including eosinophils and mononuclear inflammatory cells. The mucosal glands appear normal under low power but on high power the luminal surface shows a blue fringe, which is strongly positive with PAS where filamentous organisms are present.
Intestinal spirochetosis is colonization of the colon by relatively nonpathogenic spirochetes. It is seen in 3 - 10% of normal patients, and is associated with anal intercourse, HIV and lower socioeconomic conditions (Ger Med Sci 2010;8:Doc01). It may occur in children, who often have abdominal symptoms (Pediatr Dev Pathol 2010;13:471, Am J Clin Pathol 2003;120:828). Intestinal spirochetosis may cause persistent diarrhea, possibly due to blunting and destruction of microvilli (Am J Clin Pathol 1986;86:679).
As in this case, histology shows an accentuation of the luminal border by spirochetes, which produce a blue line on H&E between the microvilli of the covering epithelium (Pathologe 2003;24:192). The spirochetes are accentuated by silver stains (Warthin-Starry, Dieterle), as well as PAS, Giemsa and Alcian blue (pH 2.5). There is usually minimal inflammation present.
Electron microscopy shows long coiled bacteria adherent to the microvilli (Ger Med Sci 2010;8:Doc01).
Symptomatic patients are treated with metronidazole.