
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jamie Shutter, University of South Florida, for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.


July 11-15, 2011
The Snow King Resort
Jackson, Wyoming (USA)
The 28th Annual Summer Update
in Clinical Immunology, Microbiology
and Infectious Disease
Course Topics:
This 24-hour review and update is intended to improve knowledge about the pathogenesis and clinical manifestations of infectious diseases, immunological mechanisms of disease and disease prevention, appropriate approaches to the diagnosis of infections and immunologic disorders, and utilization of the clinical microbiology and immunology laboratory including selection and interpretation of results.
This course will provide a forum for the exchange of ideas dealing with microbial infections as well as immunity to infectious diseases and immunologic disorders. Faculty consists of clinicians involved in patient care, pathologists, and clinical laboratory scientists. Discussion of timely topics by faculty and participants assures that this course will be informative, interesting, and relevant.
Course Directors:
Harry R. Hill MD, Larry G. Reimer MD, July Daly PhD
This course is approved for 24 AMA PRA Category I Credit(s)
Website
Schedule
Hotel
Register
[#2506]
(1) Thanks to Michael Constantinescu, M.D., Overton Brooks VA Medical Center, Louisiana, for writing a new section for the Thyroid Gland chapter on Bethesda Guidelines for Cytology. Thanks to Dr. Larry Bernstein, Triplex Consulting, Connecticut, for writing Cardiac topics for the Clinical Chemistry chapter.
(2) Recent articles posted on our Management Page include: 1993 Medicaid Reform Comes to Florida, by Mick Raich, Vachette Pathology, Dj vu all Over Again, by Mick Raich, Vachette Pathology, and Stories That Will Curl Your Hair Or Close To It!, by Michelle Miller, Vachette Pathology.
Visit and follow our Blog to see recent updates to the website.
Case #202
Clinical history:
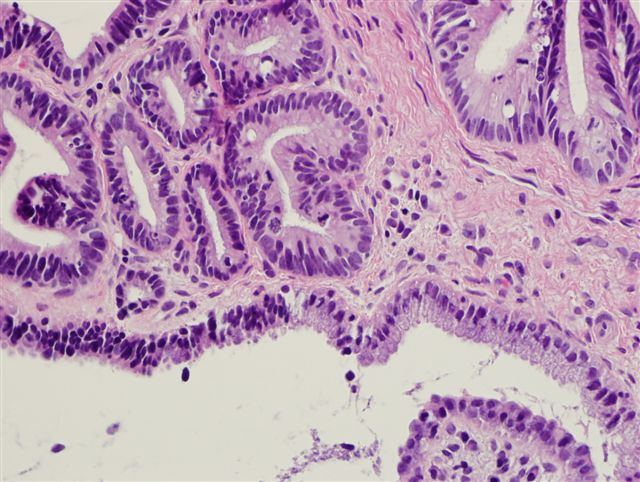
A 30 year old woman had a pap smear diagnosis of HSIL, followed by a cervical biopsy, which is shown below with Ki67 and p16 staining.
Microscopic images:

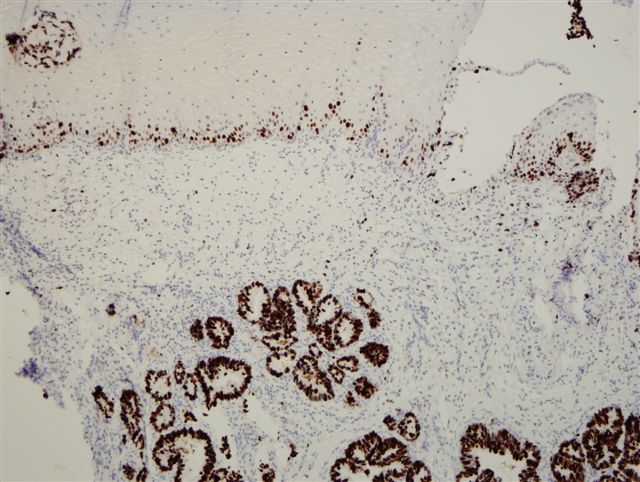

Ki67 (left) and p16 (right) staining
What is your diagnosis?
Diagnosis: Adenocarcinoma in situ (AIS) of the endocervix
Discussion:
The biopsy shows the typical appearance of adenocarcinoma in situ of the endocervix. Low power shows malignant, darkened glands composed of hyperchromatic, enlarged, crowded nuclei with coarse chromatin, small single or multiple nucleoli and frequent mitotic figures. In this case, the surface epithelium is uninvolved but the malignant glands are superficial to a large benign gland.
In pap smears, adenocarcinoma in situ has a higher false negative rate than HSIL and squamous cell carcinoma (Arch Pathol Lab Med 2004;128:153). As a result, the use of p16 may be helpful in difficult cases.
p16 (p16INK4A) is an inhibitor of cyclin dependent kinases and p16 overexpression has been observed in cervical intraepithelial lesions and invasive carcinomas associated with high risk HPV types (Am J Surg Pathol 2004;28:160). p16 distinguishes uterine cervical adenocarcinomas (p16+) from benign lesions (p16 negative) and from endometrioid adenocarcinomas of the uterine corpus (p16 negative) (Am J Surg Pathol 2003;27:187, Virchows Arch 2006;448:597). p16 immunostains and HPV DNA analysis are also helpful in determining if endometrial tumors originate in endometrium (HPV and p16 negative) or from the endocervix (HPV and p16 positive) (Am J Surg Pathol 2009;33:914). In this case, Ki67 staining shows the high proliferative index of the lesion and the basal layer of squamous epithelium serves as a positive internal control.
The differential diagnosis of endocervical adenocarcinoma in situ includes:
- Tubal or tuboendometrial hyperplasia: involves only a single gland or portion of a gland, no significant nuclear atypia
- Invasive adenocarcinoma: infiltrating glands with more atypia, budding and other architectural alterations, desmoplasia, extension of glands beyond normal glandular depth
- Metastatic adenocarcinoma from ovary (serous or clear cell) or other sites (Am J Surg Pathol 2010;34:735)
Treatment consists of loop electrosurgical excision procedure (LEEP), laser therapy, conization or cryotherapy. Follow up is recommended.
