2 May 2008 - Case #117
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Debra L. Zynger, M.D., Ava Hosseini, B.A. and Ximing J. Yang, M.D., Ph.D., Northwestern Memorial Hospital, Northwestern University, Chicago, Illinois (USA).
Case #117
Clinical history:
A 70 year old man had laparoscopic robotic assisted radical prostatectomy.
Microscopic images:
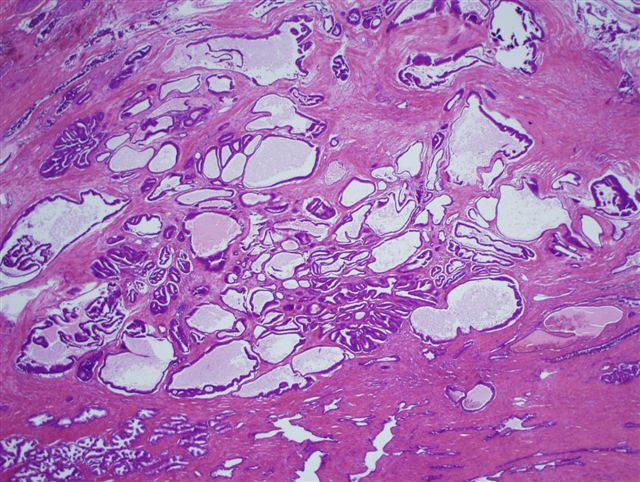
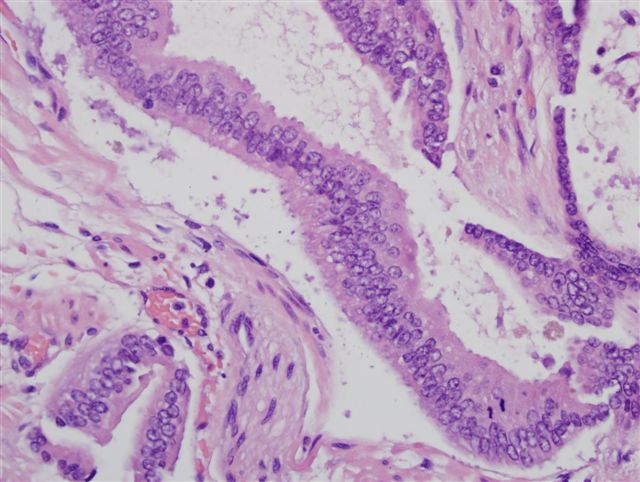
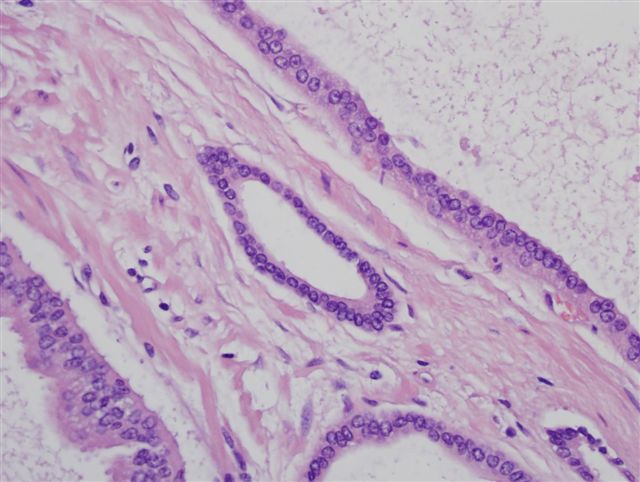

What is your diagnosis?
Diagnosis: Pseudohyperplastic variant of prostatic adenocarcinoma
Immunostains:
Discussion:
The malignant nature of the hyperplastic appearing glands was confirmed with the triple stain, which showed lack of basal cells (i.e., no staining) by p63 and high molecular weight keratin and staining of the hyperplastic cells by AMACR. The normal appearing glands served as controls.
Pseudohyperplastic variant of prostatic adenocarcinoma is a rare variant in which at least 60% of the tumor has architectural features resembling benign hyperplastic glands (Am J Surg Pathol 2000;24:1039). The tumor typically has complex, medium to large sized glands with crowding, papillary infoldings and branching or cystic dilatations. The nuclei are enlarged, and often have prominent nucleoli. There are usually pink amorphous secretions and often crystalloids. At low power, transition to typical, small acinar adenocarcinomas may be a helpful diagnostic clue (Am J Surg Pathol 1998;22:1239). With core needle biopsies, the only diagnostic clue may be a subtle disruption of the normal glandular stromal relationship. Basal cell stains (p63, HMWK) are important to confirm the absence of basal cells and the tumor cells are immunoreactive for AMACR / P504S in 70% of cases (Am J Surg Pathol 2003;27:772).
Pseudohyperplastic variant may be misdiagnosed as benign hyperplasia. In one study, the rate of false negative diagnoses was 1.3% for TURP specimens (Pathol Oncol Res 2003;9:232). The differential diagnosis also includes high grade prostatic intraepithelial neoplasia. Although high grade PIN also shows papillary infoldings with prominent nucleoli, the glands are not as crowded or infiltrative.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Debra L. Zynger, M.D., Ava Hosseini, B.A. and Ximing J. Yang, M.D., Ph.D., Northwestern Memorial Hospital, Northwestern University, Chicago, Illinois (USA).
Website news:
(1) We recently established The Detroit College Promise. This program, modeled on the Kalamazoo Promise, will provide tuition scholarships for Detroit Public School students. We expect that it will dramatically increase the number of Detroit college graduates over time, and transform the City of Detroit into a center of urban brainpower and economic prosperity. Click here for more information.
Visit and follow our Blog to see recent updates to the website.
(1) We recently established The Detroit College Promise. This program, modeled on the Kalamazoo Promise, will provide tuition scholarships for Detroit Public School students. We expect that it will dramatically increase the number of Detroit college graduates over time, and transform the City of Detroit into a center of urban brainpower and economic prosperity. Click here for more information.
Visit and follow our Blog to see recent updates to the website.
Case #117
Clinical history:
A 70 year old man had laparoscopic robotic assisted radical prostatectomy.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Pseudohyperplastic variant of prostatic adenocarcinoma
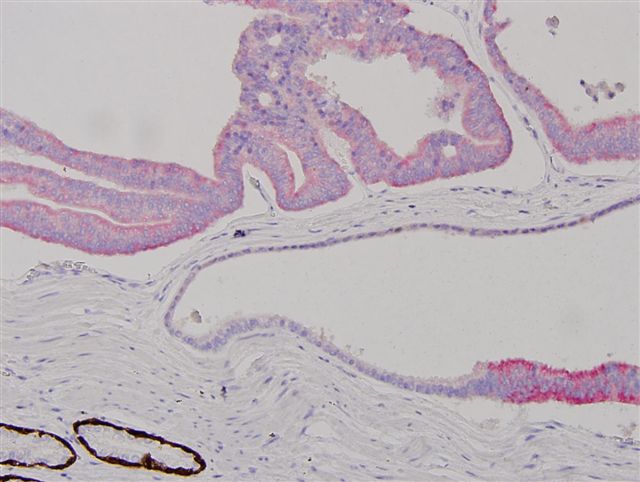
Immunostains:
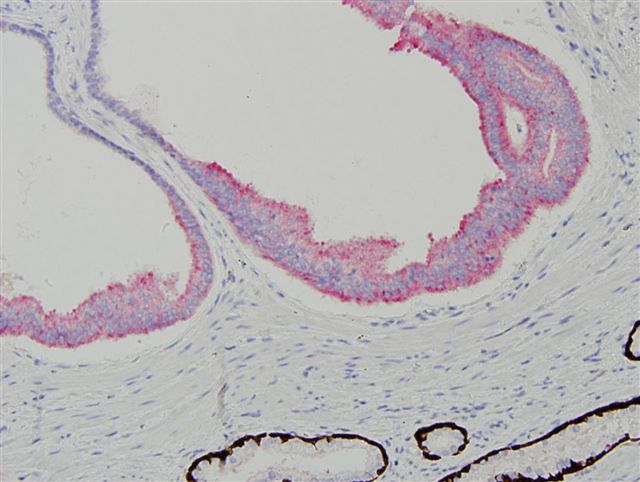
Triple stain (AMACR, p63, HMWK)
Discussion:
The malignant nature of the hyperplastic appearing glands was confirmed with the triple stain, which showed lack of basal cells (i.e., no staining) by p63 and high molecular weight keratin and staining of the hyperplastic cells by AMACR. The normal appearing glands served as controls.
Pseudohyperplastic variant of prostatic adenocarcinoma is a rare variant in which at least 60% of the tumor has architectural features resembling benign hyperplastic glands (Am J Surg Pathol 2000;24:1039). The tumor typically has complex, medium to large sized glands with crowding, papillary infoldings and branching or cystic dilatations. The nuclei are enlarged, and often have prominent nucleoli. There are usually pink amorphous secretions and often crystalloids. At low power, transition to typical, small acinar adenocarcinomas may be a helpful diagnostic clue (Am J Surg Pathol 1998;22:1239). With core needle biopsies, the only diagnostic clue may be a subtle disruption of the normal glandular stromal relationship. Basal cell stains (p63, HMWK) are important to confirm the absence of basal cells and the tumor cells are immunoreactive for AMACR / P504S in 70% of cases (Am J Surg Pathol 2003;27:772).
Pseudohyperplastic variant may be misdiagnosed as benign hyperplasia. In one study, the rate of false negative diagnoses was 1.3% for TURP specimens (Pathol Oncol Res 2003;9:232). The differential diagnosis also includes high grade prostatic intraepithelial neoplasia. Although high grade PIN also shows papillary infoldings with prominent nucleoli, the glands are not as crowded or infiltrative.