
22 April 2008 - Case #116
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Keloth E. Pradeep, Wrexham Maelor Hospital, United Kingdom, for contributing this case.
Case #116
Clinical history:
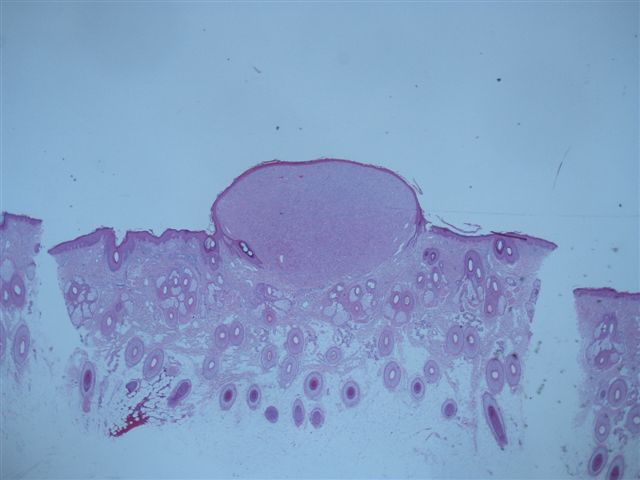
A 60 year old man had a pearly papular lesion of the scalp.
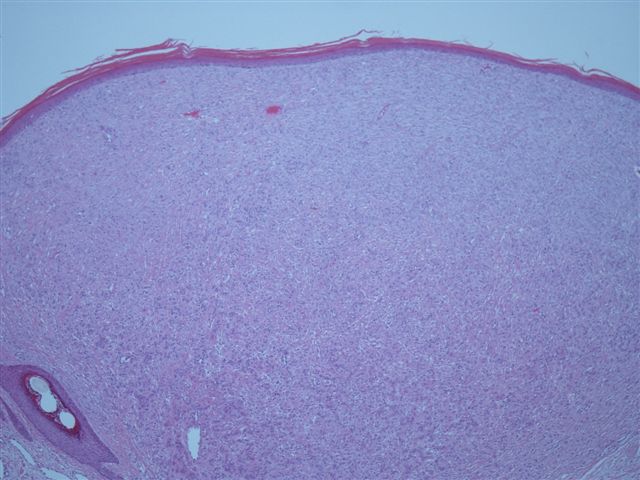
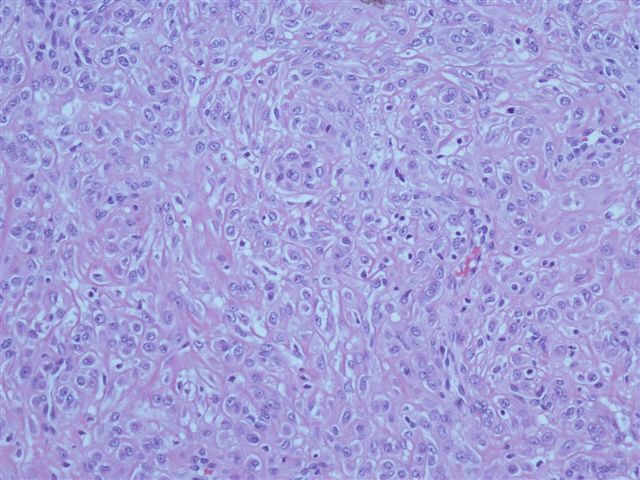
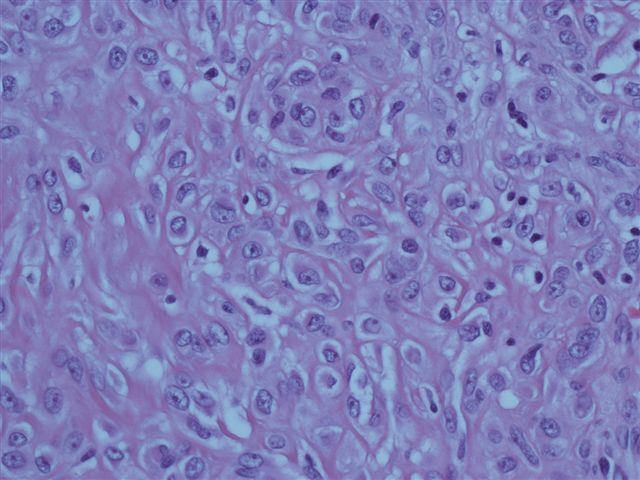
Microscopic images:
What is your diagnosis?
Diagnosis: Epithelioid variant of benign fibrous histiocytoma
Immunostains:

Discussion:
This uncommon variant of benign fibrous histiocytoma (dermatofibroma) usually presents as a small (1 cm or less), solitary, elevated nodule in the extremities. The mean age is 42 years (Br J Dermatol 1989;120:185). It is composed of uniform, medium to large, angulated epithelioid cells, often perivascular, with overlying epidermal effacement (Am J Surg Pathol 1994;18:583). There is minimal inflammation and no prominent giant cells. The phenotype is predominantly myofibroblastic and not histiocytic. These tumors are immunoreactive for factor XIII but negative for CD68 and CD163. They may arise from the dermal microvascular unit (J Cutan Pathol 2003;30:415).
The differential diagnosis includes solitary epithelioid histiocytoma, Rosai-Dorfman disease and granulomatous conditions. This case most closely resembles solitary epithelioid histiocytoma, a recently described lesion formerly called reticulohistiocytoma (Am J Surg Pathol 2006;30:521). It is composed of large epithelioid histiocytes but with abundant dense eosinophilic and glassy cytoplasm, often with spike-like cytoplasmic extensions. The nuclei are round / oval with distinct nucleoli. Unlike this case, there are variable nuclear grooves and multinucleated cells, and frequent lymphocytes and neutrophils. There is some overlap with epithelioid variant of benign fibrous histiocytoma regarding the staining pattern, as the histiocytes are immunoreactive for vimentin and may have focal staining for factor XIIIa. They are also immunoreactive for CD163, CD68 (may be focal) and negative for MelanA, S100 and keratin.
Rosai-Dorfman disease usually presents with multiple skin lesions and adenopathy. Its histiocytes are pleomorphic, with emperipolesis and S100 staining. There are also prominent B cells and plasma cells. Granulomas also contain epithelioid histiocytes but they are in well formed clusters and are surrounded by lymphocytes.
Malignant lesions to consider include melanoma (tight clustering of cells, S100+, HMB45+), epithelioid sarcoma (deep seated, granuloma type clusters with necrosis, more atypia, keratin+, CD163-) and histiocytic sarcoma (marked atypia and mitotic activity).
Epithelioid variant of benign fibrous histiocytoma has an excellent prognosis, with only rare recurrences reported after excision.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Keloth E. Pradeep, Wrexham Maelor Hospital, United Kingdom, for contributing this case.
Website news:
(1) We recently established The Detroit College Promise. This program, modeled on the Kalamazoo Promise, will provide tuition scholarships for Detroit Public School students. We expect that it will dramatically increase the number of Detroit college graduates over time, and transform the City of Detroit into a center of urban brainpower and economic prosperity. Click here for more information.
Visit and follow our Blog to see recent updates to the website.
(1) We recently established The Detroit College Promise. This program, modeled on the Kalamazoo Promise, will provide tuition scholarships for Detroit Public School students. We expect that it will dramatically increase the number of Detroit college graduates over time, and transform the City of Detroit into a center of urban brainpower and economic prosperity. Click here for more information.
Visit and follow our Blog to see recent updates to the website.
Case #116
Clinical history:
A 60 year old man had a pearly papular lesion of the scalp.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Epithelioid variant of benign fibrous histiocytoma
Immunostains:
Vimentin
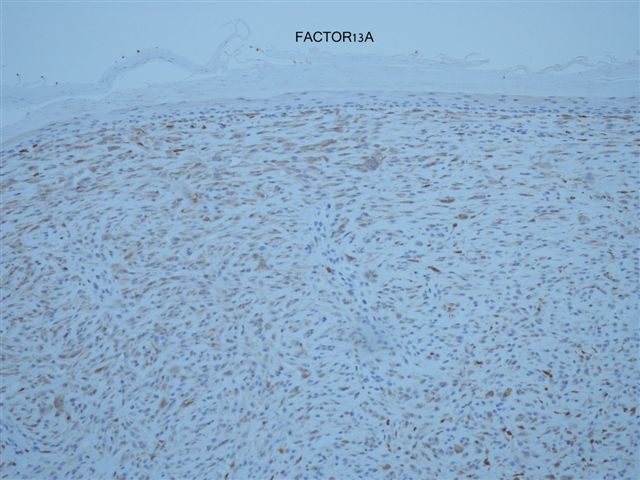
Factor XIIIA
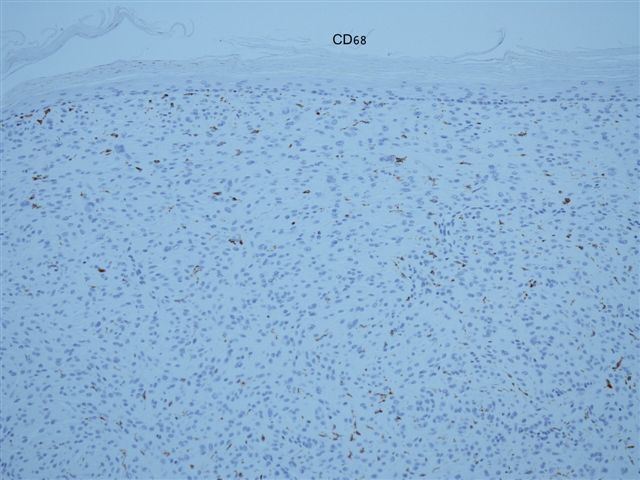
CD68
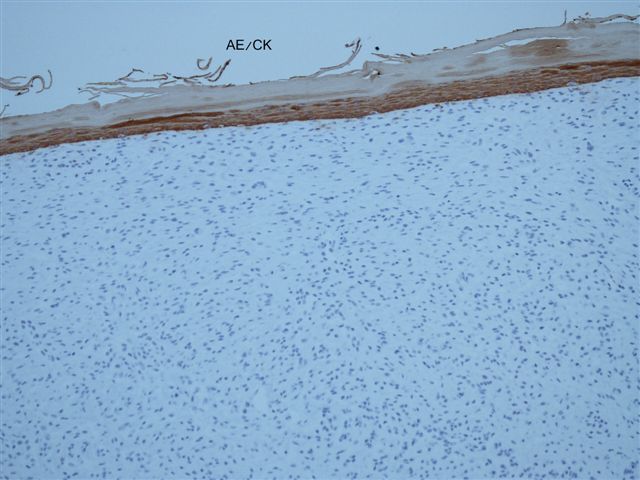
Keratin
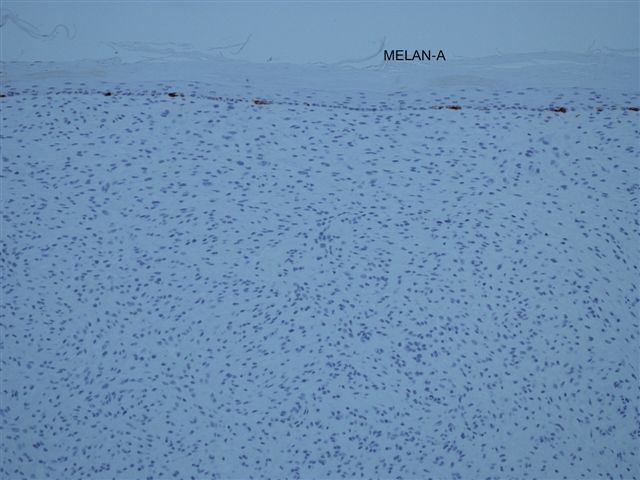
MelanA
Discussion:
This uncommon variant of benign fibrous histiocytoma (dermatofibroma) usually presents as a small (1 cm or less), solitary, elevated nodule in the extremities. The mean age is 42 years (Br J Dermatol 1989;120:185). It is composed of uniform, medium to large, angulated epithelioid cells, often perivascular, with overlying epidermal effacement (Am J Surg Pathol 1994;18:583). There is minimal inflammation and no prominent giant cells. The phenotype is predominantly myofibroblastic and not histiocytic. These tumors are immunoreactive for factor XIII but negative for CD68 and CD163. They may arise from the dermal microvascular unit (J Cutan Pathol 2003;30:415).
The differential diagnosis includes solitary epithelioid histiocytoma, Rosai-Dorfman disease and granulomatous conditions. This case most closely resembles solitary epithelioid histiocytoma, a recently described lesion formerly called reticulohistiocytoma (Am J Surg Pathol 2006;30:521). It is composed of large epithelioid histiocytes but with abundant dense eosinophilic and glassy cytoplasm, often with spike-like cytoplasmic extensions. The nuclei are round / oval with distinct nucleoli. Unlike this case, there are variable nuclear grooves and multinucleated cells, and frequent lymphocytes and neutrophils. There is some overlap with epithelioid variant of benign fibrous histiocytoma regarding the staining pattern, as the histiocytes are immunoreactive for vimentin and may have focal staining for factor XIIIa. They are also immunoreactive for CD163, CD68 (may be focal) and negative for MelanA, S100 and keratin.
Rosai-Dorfman disease usually presents with multiple skin lesions and adenopathy. Its histiocytes are pleomorphic, with emperipolesis and S100 staining. There are also prominent B cells and plasma cells. Granulomas also contain epithelioid histiocytes but they are in well formed clusters and are surrounded by lymphocytes.
Malignant lesions to consider include melanoma (tight clustering of cells, S100+, HMB45+), epithelioid sarcoma (deep seated, granuloma type clusters with necrosis, more atypia, keratin+, CD163-) and histiocytic sarcoma (marked atypia and mitotic activity).
Epithelioid variant of benign fibrous histiocytoma has an excellent prognosis, with only rare recurrences reported after excision.
