


20 March 2008 - Case #113
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Mowafak Hamodat, Eastern Health of Newfoundland and Labrador, St. John's, Canada.
Case #113
Clinical history:
A 24 year old woman had a 1 x 0.8 cm skin lesion with a central dark brown area, which was excised.
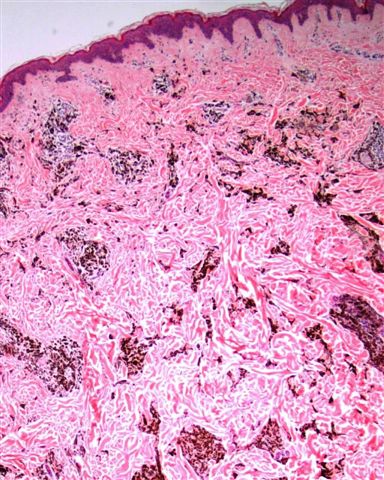
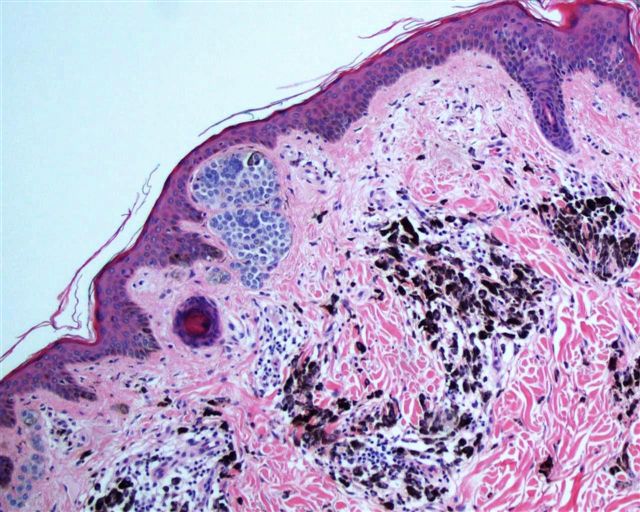
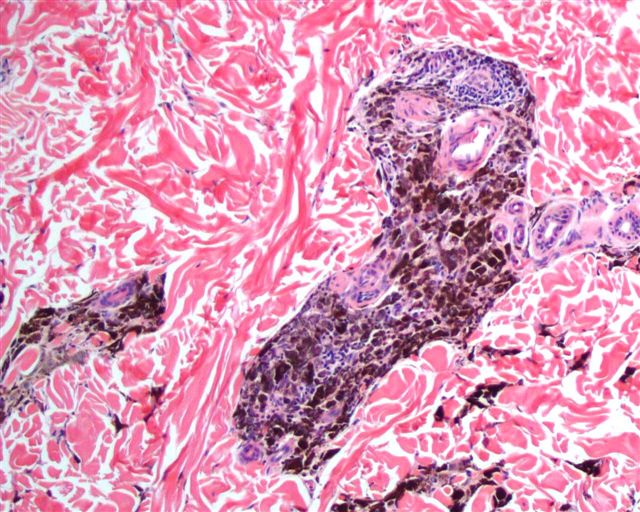
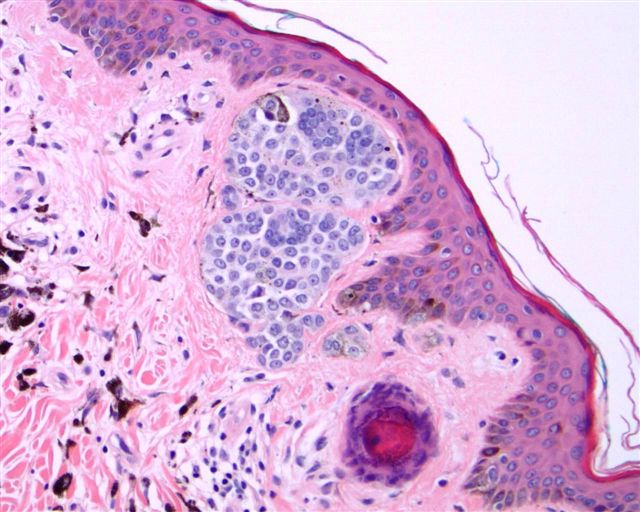
Microscopic images:

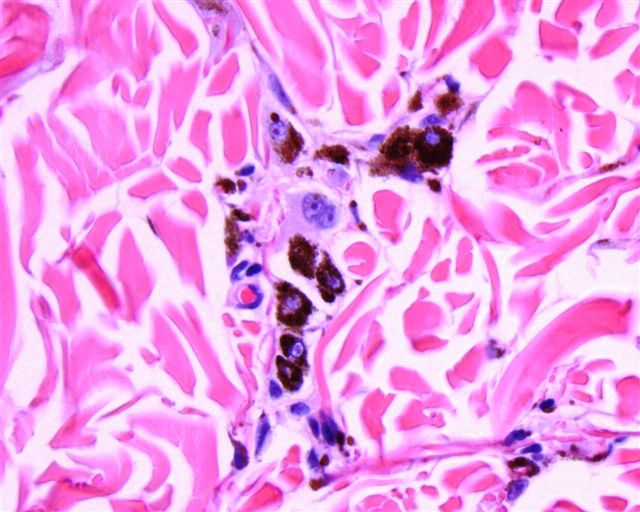
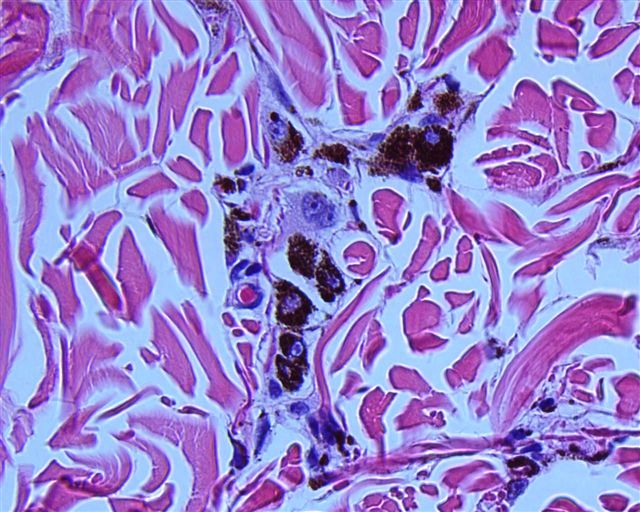
What is your diagnosis?
Diagnosis: Combined dermal / pigmented epithelioid melanocytoma
Discussion:
The diagnosis was confirmed by Dr. M. Mihm of Harvard Medical School.
Pigmented epithelioid melanocytoma is a low grade variant of melanoma first described under this name in 2004 (Am J Surg Pathol 2004;28:31). It includes lesions previously described as animal type melanoma and epithelioid blue nevus of the Carney complex (myxomas, spotty skin pigmentation, endocrine overactivity and schwannomas) (Am J Surg Pathol 1996;20:259).
The median patient age is 27 years, with a wide range. The extremities are the most common site, although numerous sites are affected. The tumor does not appear to be related to sun exposure. Clinically, the tumor resembles a combined nevus (Dermatol Online J 2005;11:1). The tumor consists of heavily pigmented epithelioid or spindled melanocytes in the deep dermis. There is variable atypia but no consistent high grade features. There may be ulceration, a combined nevus or rarely necrosis. Nodal metastases are found in 46% of cases but death from disease is rare. Recommended treatment is sentinel lymph node sampling and conservative re-excision.
These tumors are associated with loss of the protein kinase A regulatory subunit type 1alpha (R1alpha), coded by the PRKAR1A gene, which is lost in both sporadic cases and patients with Carney complex (Am J Surg Pathol 2007;31:1764).
Differential diagnosis includes blue nevus (no pigmented and epithelioid cells) and nodular melanosis (pigmented cells are actually pigment laden macrophages).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Mowafak Hamodat, Eastern Health of Newfoundland and Labrador, St. John's, Canada.
Website news:
(1) Visit our newly updated Thyroid Gland chapter to quickly review any of its 111 thyroid related topics. It contains extensive text, plus over 1000 high quality images and 760 references. We are currently updating the Soft Tissue chapters (it is being split in two). Don't forget, to search a particular page for a word or phase, use Control F, then type in the phrase.
Visit and follow our Blog to see recent updates to the website.
(1) Visit our newly updated Thyroid Gland chapter to quickly review any of its 111 thyroid related topics. It contains extensive text, plus over 1000 high quality images and 760 references. We are currently updating the Soft Tissue chapters (it is being split in two). Don't forget, to search a particular page for a word or phase, use Control F, then type in the phrase.
Visit and follow our Blog to see recent updates to the website.
Case #113
Clinical history:
A 24 year old woman had a 1 x 0.8 cm skin lesion with a central dark brown area, which was excised.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Combined dermal / pigmented epithelioid melanocytoma
Discussion:
The diagnosis was confirmed by Dr. M. Mihm of Harvard Medical School.
Pigmented epithelioid melanocytoma is a low grade variant of melanoma first described under this name in 2004 (Am J Surg Pathol 2004;28:31). It includes lesions previously described as animal type melanoma and epithelioid blue nevus of the Carney complex (myxomas, spotty skin pigmentation, endocrine overactivity and schwannomas) (Am J Surg Pathol 1996;20:259).
The median patient age is 27 years, with a wide range. The extremities are the most common site, although numerous sites are affected. The tumor does not appear to be related to sun exposure. Clinically, the tumor resembles a combined nevus (Dermatol Online J 2005;11:1). The tumor consists of heavily pigmented epithelioid or spindled melanocytes in the deep dermis. There is variable atypia but no consistent high grade features. There may be ulceration, a combined nevus or rarely necrosis. Nodal metastases are found in 46% of cases but death from disease is rare. Recommended treatment is sentinel lymph node sampling and conservative re-excision.
These tumors are associated with loss of the protein kinase A regulatory subunit type 1alpha (R1alpha), coded by the PRKAR1A gene, which is lost in both sporadic cases and patients with Carney complex (Am J Surg Pathol 2007;31:1764).
Differential diagnosis includes blue nevus (no pigmented and epithelioid cells) and nodular melanosis (pigmented cells are actually pigment laden macrophages).
