31 August 2007 - Case #94
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Juan José Segura Fonseca, Departamento de Patología, Hospital San Juan de Dios, San José, Costa Rica.
Case #94
Clinical history:
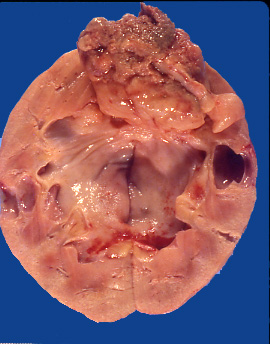
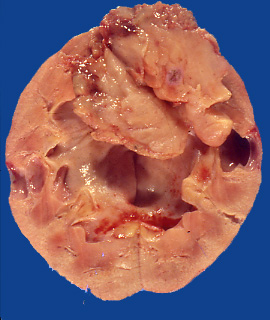
A 57 year old Caucasian man was admitted for gross hematuria and flank pain. An intravenous pyelogram disclosed a large filling defect in the renal pelvis due to tumor. A nephrectomy was performed. On opening the kidney, a large solid tumor filled the entire renal pelvis and was associated with dilated calyces. The tumor was polypoid and did not adhere to the inner surface of the urothelium. It was attached by a broad base to the superior border of the pelvis. It exhibited hemorrhagic necrosis and was composed of soft tan tissue.
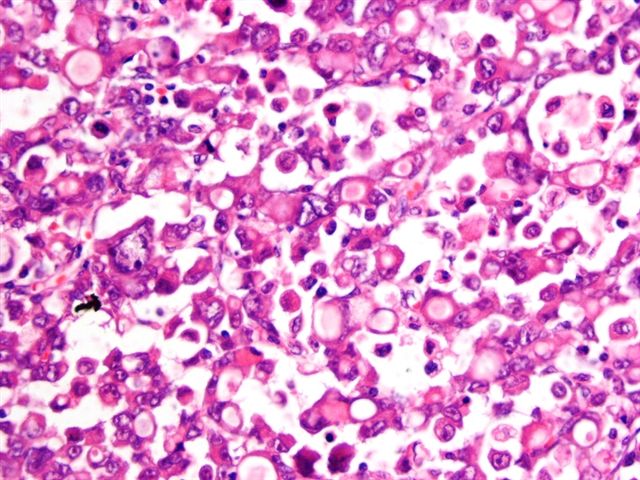
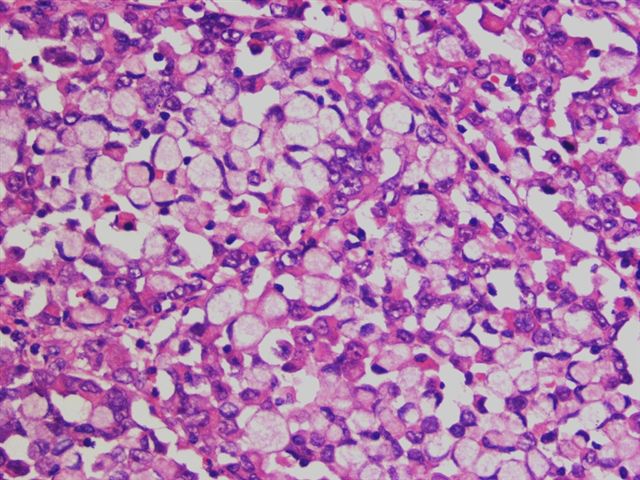
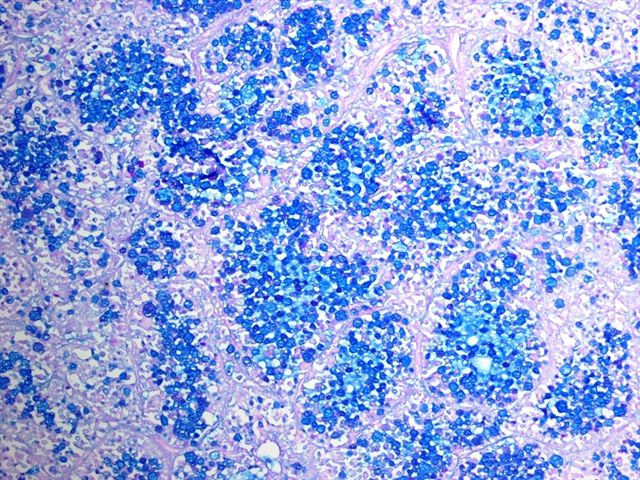
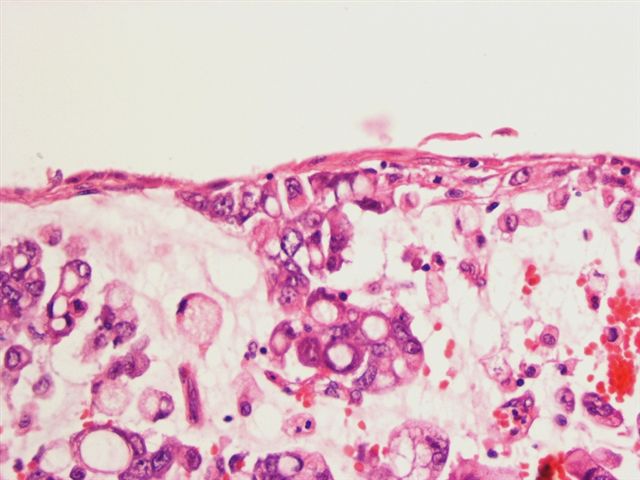
Microscopy showed numerous cells with pink, rhabdoid features and abundant intracytoplasmic lumina. Some areas were composed almost entirely of signet ring cells that demonstrated abundant intracytoplasmic mucin with the PAS / Alcian blue stain. No areas of urothelial (transitional cell) carcinoma were identified.
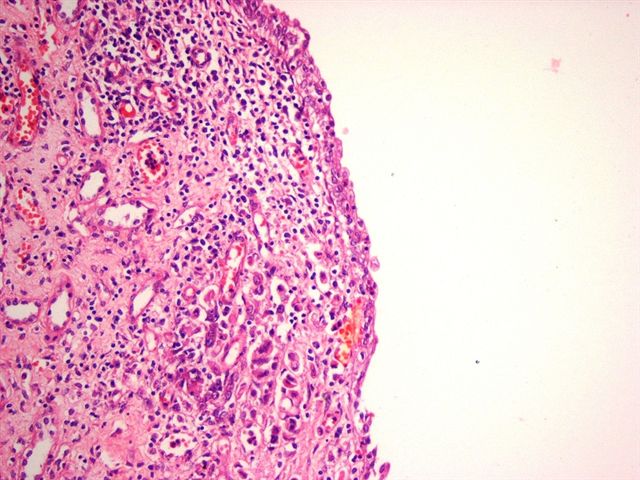
There was also severe chronic inflammation of the renal pelvis with atrophic urothelium and superficial invasion by tumor cells, as well as superficial goblet cell metaplasia of the urothelium.
Gross images:
Microscopic images:
What is your diagnosis?
Diagnosis: Signet ring cell adenocarcinoma of the renal pelvis
Discussion:
Primary neoplasms of the renal pelvis are rare and account for 7% of all renal tumors. Most are urothelial (transitional cell) carcinomas (Campbell: Campbell's Urology, 1986, Am J Surg Pathol 2004;28:1545, Mod Pathol 2006;19:494). The urothelium can display a wide variety of differentiation and metaplastic changes, particularly in high grade neoplasms. These changes have been described in detail in the urinary bladder but are less well known in the renal pelvis (MacLennan: Urologic Surgical Pathology, 4th Edition, 2019).
Among the high grade carcinomas of the renal pelvis, mucinous adenocarcinoma is very uncommon, representing < 1% of renal pelvic neoplasms (Urol Int 1988;43:299). Most are pure adenocarcinomas with gland formation and mucin production. Only rarely are they associated with conventional urothelial carcinoma (Urol Int 1988;43:299, Int J Urol 2004;11:1016).
Mucinous carcinomas are usually large, infiltrating tumors which fill a dilated renal pelvis and calyces and invade the adjacent renal parenchyma (Hinyokika Kiyo 2002;48:187, Hinyokika Kiyo 1997;43:727, Pathol Res Pract 1993;189:946, Urology 1993;41:292). The signet ring pattern is rare and may be associated with collagenous spherulosis (Pathol Res Pract 1993;189:946, Int J Surg Pathol 2005;13:375). Intestinal, mucinous, cystitis cystica and goblet cell metaplasia of the urothelium, present in this case, have been implicated as precursor lesions (Indian J Cancer 2003;40:108).
The differential diagnosis includes high grade urothelial carcinoma, which may show foci of signet rings and the rare lipoid cell variant of urothelial carcinoma (Mod Pathol 2006;19:494, Am J Surg Pathol 2007;31:770). The signet ring cells in both variants are mucin negative and the tumors also have areas of usual type high grade urothelial carcinoma. Metastases from the stomach, breast or other organs must also be ruled out.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Juan José Segura Fonseca, Departamento de Patología, Hospital San Juan de Dios, San José, Costa Rica.
Website news:
(1) In September, we will attend the Beaumont Hospital DNA Conference in Troy, Michigan and the CAP Annual Meeting in Chicago. In October, we will attend the Wayne State University annual conference in Dearborn, Michigan and the ASCP Annual Meeting in New Orleans.
Visit and follow our Blog to see recent updates to the website.
(1) In September, we will attend the Beaumont Hospital DNA Conference in Troy, Michigan and the CAP Annual Meeting in Chicago. In October, we will attend the Wayne State University annual conference in Dearborn, Michigan and the ASCP Annual Meeting in New Orleans.
Visit and follow our Blog to see recent updates to the website.
Case #94
Clinical history:
A 57 year old Caucasian man was admitted for gross hematuria and flank pain. An intravenous pyelogram disclosed a large filling defect in the renal pelvis due to tumor. A nephrectomy was performed. On opening the kidney, a large solid tumor filled the entire renal pelvis and was associated with dilated calyces. The tumor was polypoid and did not adhere to the inner surface of the urothelium. It was attached by a broad base to the superior border of the pelvis. It exhibited hemorrhagic necrosis and was composed of soft tan tissue.
Microscopy showed numerous cells with pink, rhabdoid features and abundant intracytoplasmic lumina. Some areas were composed almost entirely of signet ring cells that demonstrated abundant intracytoplasmic mucin with the PAS / Alcian blue stain. No areas of urothelial (transitional cell) carcinoma were identified.
There was also severe chronic inflammation of the renal pelvis with atrophic urothelium and superficial invasion by tumor cells, as well as superficial goblet cell metaplasia of the urothelium.
Gross images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Signet ring cell adenocarcinoma of the renal pelvis
Discussion:
Primary neoplasms of the renal pelvis are rare and account for 7% of all renal tumors. Most are urothelial (transitional cell) carcinomas (Campbell: Campbell's Urology, 1986, Am J Surg Pathol 2004;28:1545, Mod Pathol 2006;19:494). The urothelium can display a wide variety of differentiation and metaplastic changes, particularly in high grade neoplasms. These changes have been described in detail in the urinary bladder but are less well known in the renal pelvis (MacLennan: Urologic Surgical Pathology, 4th Edition, 2019).
Among the high grade carcinomas of the renal pelvis, mucinous adenocarcinoma is very uncommon, representing < 1% of renal pelvic neoplasms (Urol Int 1988;43:299). Most are pure adenocarcinomas with gland formation and mucin production. Only rarely are they associated with conventional urothelial carcinoma (Urol Int 1988;43:299, Int J Urol 2004;11:1016).
Mucinous carcinomas are usually large, infiltrating tumors which fill a dilated renal pelvis and calyces and invade the adjacent renal parenchyma (Hinyokika Kiyo 2002;48:187, Hinyokika Kiyo 1997;43:727, Pathol Res Pract 1993;189:946, Urology 1993;41:292). The signet ring pattern is rare and may be associated with collagenous spherulosis (Pathol Res Pract 1993;189:946, Int J Surg Pathol 2005;13:375). Intestinal, mucinous, cystitis cystica and goblet cell metaplasia of the urothelium, present in this case, have been implicated as precursor lesions (Indian J Cancer 2003;40:108).
The differential diagnosis includes high grade urothelial carcinoma, which may show foci of signet rings and the rare lipoid cell variant of urothelial carcinoma (Mod Pathol 2006;19:494, Am J Surg Pathol 2007;31:770). The signet ring cells in both variants are mucin negative and the tumors also have areas of usual type high grade urothelial carcinoma. Metastases from the stomach, breast or other organs must also be ruled out.