28 June 2007 - Case #88
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Hanni Gulwani, Sir Ganga Ram Hospital, New Delhi (India).
Case #88
Clinical history:
A 13 month old girl had an incidental liver mass that was excised. Clinically, it was thought to be a hepatoblastoma.
Gross images:


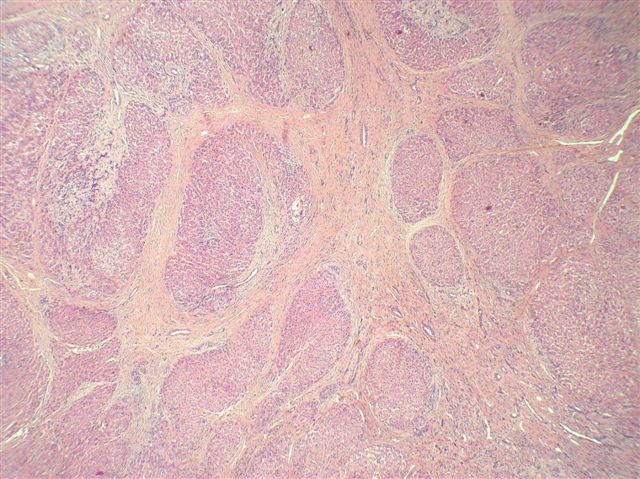
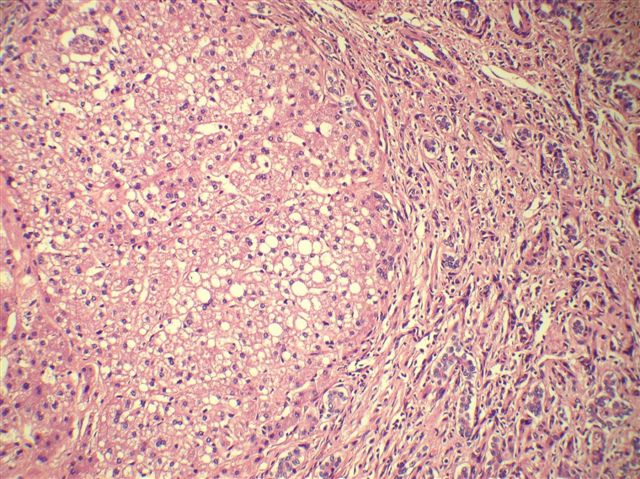
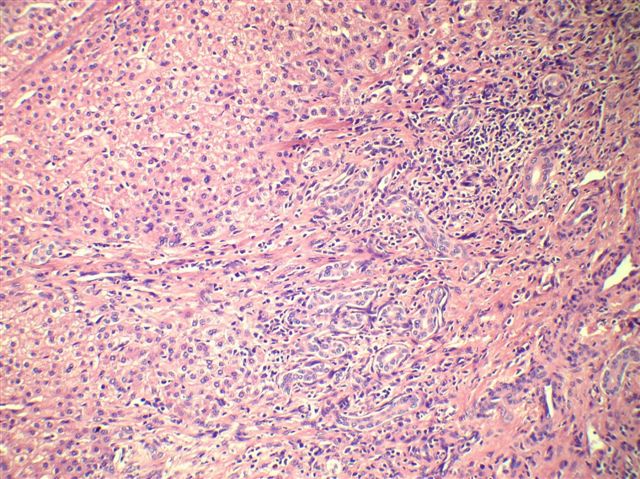
Microscopic images:
What is your diagnosis?
Diagnosis: Focal nodular hyperplasia of the liver
Discussion:
This tumor characteristically is a solitary (80%), subcapsular, nodular and bulging mass, light brown to yellow (usually lighter than the surrounding liver), with a central stellate scar from which broad fibrous septa radiate outwards. It is usually well circumscribed but not encapsulated. The normal liver (N) has a smooth cut surface.
Microscopic images show an abnormal nodular architecture that contains all the components of a normal liver lobule. Thick fibrous septa divide the lesion into lobules resembling those of cirrhosis, with marked bile ductular proliferation. There are often changes of chronic cholestasis, including Mallory hyaline, bile pigment, copper deposits and pseudoxanthomatous change. Large malformed vessels are also present, particularly in the central scar. Most tumors (80%) have the 3 classic features of abnormal architecture, bile ductular proliferation and malformed vessels. Nonclassic forms lack either abnormal architecture or malformed vessels and are divided into 3 types: telangiectatic, mixed hyperplastic and adenomatous or atypia of large cell (Am J Surg Pathol 1999;23:1441).
Focal nodular hyperplasia (FNH) is the second most common tumor of the liver, after hemangioma. Some studies show a female predominance. The median age is 38 years. It may be associated with oral contraceptive use in women. It also constitutes 2% of pediatric hepatic tumors. FNH is believed to represent a localized hepatocyte response to an underlying congenital arteriovenous malformation or other vascular anomaly. It is not a premalignant condition (Am J Gastroenterol 2006;101:2341). Patients are usually clinically asymptomatic with incidental detection of a mass but some may have abdominal discomfort, pain, anorexia or fatigue (Hepatobiliary Pancreat Dis Int 2004;3:199). CT and MRI are important diagnostic methods but it is difficult to make a definite preoperative diagnosis in many cases (Hepatobiliary Pancreat Dis Int 2007;6:52).
The differential diagnosis includes cirrhosis, fibrolamellar hepatocellular carcinoma and hepatocellular adenoma. Cirrhosis affects the entire liver and has no normal areas. Fibrolamellar carcinoma has significant fibrosis but also marked atypia of hepatocytes. Hepatocellular adenoma is monoclonal (FNH is not) but shares some clinical features with FNH. In fact, telangiectatic FNH is considered by some to be a variant of hepatocellular adenoma (World J Gastroenterol 2007;13:2649).
FNH is a benign condition. Pediatric patients are usually treated conservatively. Adult women should discontinue oral contraceptives, if applicable. Surgery is indicated for symptomatic patients, complications, compression of adjacent organs or lesion progression (Eur J Pediatr Surg 2006;16:235).
References: Radiographics 2004;24:3, eMedicine: Focal Nodular Hyperplasia (FNH) Imaging and Diagnosis [Accessed 20 May 2024]
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Hanni Gulwani, Sir Ganga Ram Hospital, New Delhi (India).
Case #88
Clinical history:
A 13 month old girl had an incidental liver mass that was excised. Clinically, it was thought to be a hepatoblastoma.
Gross images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Focal nodular hyperplasia of the liver
Discussion:
This tumor characteristically is a solitary (80%), subcapsular, nodular and bulging mass, light brown to yellow (usually lighter than the surrounding liver), with a central stellate scar from which broad fibrous septa radiate outwards. It is usually well circumscribed but not encapsulated. The normal liver (N) has a smooth cut surface.
Microscopic images show an abnormal nodular architecture that contains all the components of a normal liver lobule. Thick fibrous septa divide the lesion into lobules resembling those of cirrhosis, with marked bile ductular proliferation. There are often changes of chronic cholestasis, including Mallory hyaline, bile pigment, copper deposits and pseudoxanthomatous change. Large malformed vessels are also present, particularly in the central scar. Most tumors (80%) have the 3 classic features of abnormal architecture, bile ductular proliferation and malformed vessels. Nonclassic forms lack either abnormal architecture or malformed vessels and are divided into 3 types: telangiectatic, mixed hyperplastic and adenomatous or atypia of large cell (Am J Surg Pathol 1999;23:1441).
Focal nodular hyperplasia (FNH) is the second most common tumor of the liver, after hemangioma. Some studies show a female predominance. The median age is 38 years. It may be associated with oral contraceptive use in women. It also constitutes 2% of pediatric hepatic tumors. FNH is believed to represent a localized hepatocyte response to an underlying congenital arteriovenous malformation or other vascular anomaly. It is not a premalignant condition (Am J Gastroenterol 2006;101:2341). Patients are usually clinically asymptomatic with incidental detection of a mass but some may have abdominal discomfort, pain, anorexia or fatigue (Hepatobiliary Pancreat Dis Int 2004;3:199). CT and MRI are important diagnostic methods but it is difficult to make a definite preoperative diagnosis in many cases (Hepatobiliary Pancreat Dis Int 2007;6:52).
The differential diagnosis includes cirrhosis, fibrolamellar hepatocellular carcinoma and hepatocellular adenoma. Cirrhosis affects the entire liver and has no normal areas. Fibrolamellar carcinoma has significant fibrosis but also marked atypia of hepatocytes. Hepatocellular adenoma is monoclonal (FNH is not) but shares some clinical features with FNH. In fact, telangiectatic FNH is considered by some to be a variant of hepatocellular adenoma (World J Gastroenterol 2007;13:2649).
FNH is a benign condition. Pediatric patients are usually treated conservatively. Adult women should discontinue oral contraceptives, if applicable. Surgery is indicated for symptomatic patients, complications, compression of adjacent organs or lesion progression (Eur J Pediatr Surg 2006;16:235).
References: Radiographics 2004;24:3, eMedicine: Focal Nodular Hyperplasia (FNH) Imaging and Diagnosis [Accessed 20 May 2024]