16 May 2007 - Case #84
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California (USA).

Novocastra™ — superior reagents for IHC and ISH
This case is sponsored by Vision BioSystems™ and its Novocastra™ reagent range, which includes antibodies, probes, detection systems and ancillaries. These advanced products provide superior results in IHC staining, ISH staining and other advanced diagnostic techniques.
With over 16 years of experience, Novocastra products have earned a reputation for quality and innovation. Novocastra’s highly qualified and experienced scientific team ensure all products are specifically tailored for today’s laboratories and their application needs. This includes ensuring new antibodies are ideal for formalin-fixed, paraffin-embedded tissue.
The Novocastra range currently contains over 1,400 products. Additional products are released regularly as the development team concentrates on new diagnostically focused, IVD-labeled products.
Advertisement
Case #84
Clinical history:
A 58 year old woman with no prior history presented with chronic sinusitis and underwent functional endoscopic sinus surgery (FESS).
Microscopic images:
What is your diagnosis?
Diagnosis: Sinonasal hemangiopericytoma
Immunostains:
Discussion:
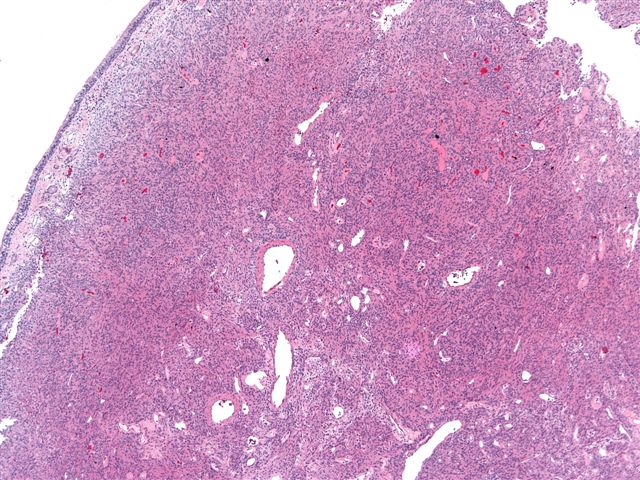
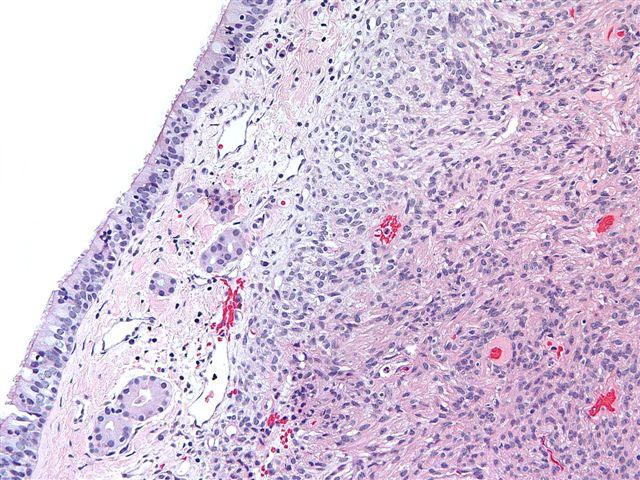
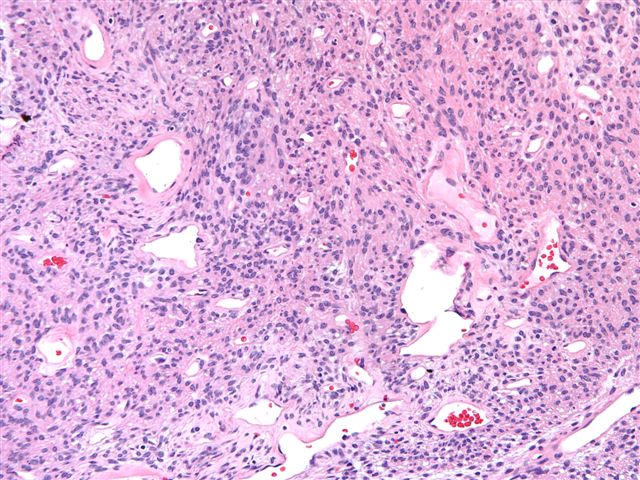
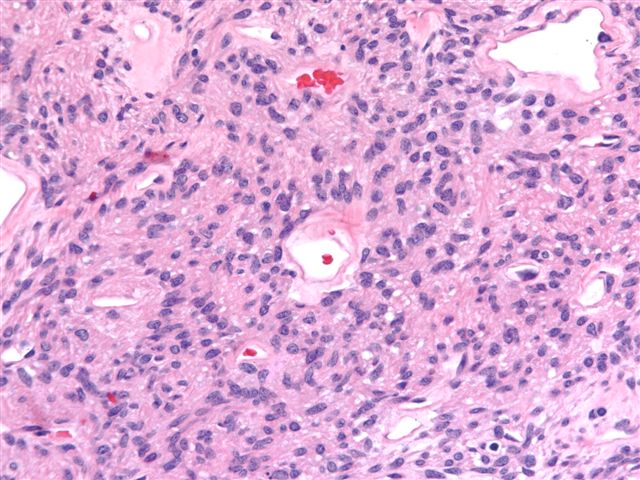
The specimen shows surface respiratory epithelium overlying the diffuse growth of bland spindled or round / oval cells. There are prominent blood vessels with a staghorn appearance and perivascular hyalinization. There is no / mild atypia, no necrosis and no significant mitotic activity. The CD34 immunostain highlights the vascular endothelium but not the tumor cells. However, the tumor cells are strongly immunoreactive for smooth muscle actin.
Sinonasal hemangiopericytoma is an uncommon tumor of pericytic myoid differentiation. The World Health Organization calls it glomangiopericytoma and others have suggested it be called myopericytoma (J Laryngol Otol 2008;122:403). It typically affects older adults, with a mean age of 63 years but may occur in children. There is often a history of airway obstruction or epistaxis in the nasal cavity or paranasal sinuses.
The histology in this case is typical. In addition, there is often a prominent inflammatory infiltrate containing eosinophils and mast cells.
Almost all cases are immunoreactive for vimentin and smooth muscle actin, with less common staining for muscle specific actin (77%) and factor XIIIa (78%). The tumor cells are negative for cytokeratin and usually for the vascular markers CD31, CD34 and factor VIII.
Electron microscopy shows that these tumors have true pericytic differentiation, with numerous intracytoplasmic thin filaments with dense bodies, irregular basement membrane-like materials, a continuous basement membrane separating tumor cells from capillaries and occasional intercellular junctions.
The differential diagnosis includes lobular capillary hemangioma, solitary fibrous tumor and glomus tumor. Lobular capillary hemangioma has a low power lobular pattern. Although spindled fibroblasts and blood vessels are prominent, the overall picture resembles granulation tissue and capillaries are small. Solitary fibrous tumor has a patternless pattern, with ropey keloid type collagen. The vascular pattern is similar to sinonasal hemangiopericytoma but a recent study found that the vessels in sinonasal hemangiopericytoma were always D2-40 positive (a marker of lymphatic endothelium) in contrast to solitary fibrous tumors / soft tissue hemangiopericytomas, which were always D2-40 negative (Virchows Arch 2006;448:459). Finally, although a glomus tumor is also a pericytic tumor and has a similar staining pattern, it is extremely rare in the sinonasal region. In addition, its morphology is different, as it typically is composed of compact epithelioid cells.
Excision of sinonasal hemangiopericytoma is adequate treatment. However, since these tumors recur 18% of the time, follow up is necessary. There are no metastases and these tumors only rarely cause death.
References: Am J Surg Pathol 2003;27:737, Arch Pathol Lab Med 2001;125:686
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California (USA).
This case is sponsored by Vision BioSystems™ and its Novocastra™ reagent range, which includes antibodies, probes, detection systems and ancillaries. These advanced products provide superior results in IHC staining, ISH staining and other advanced diagnostic techniques.
With over 16 years of experience, Novocastra products have earned a reputation for quality and innovation. Novocastra’s highly qualified and experienced scientific team ensure all products are specifically tailored for today’s laboratories and their application needs. This includes ensuring new antibodies are ideal for formalin-fixed, paraffin-embedded tissue.
The Novocastra range currently contains over 1,400 products. Additional products are released regularly as the development team concentrates on new diagnostically focused, IVD-labeled products.
Website news:
(1) Sign up for our new Books email by subscribing to our Monthly Updates newsletter here. Every month, we will send you a list of new pathology related books with a short summary and link to Amazon.com and the publisher for further information. The email is free, and you can unsubscribe at any time.
Visit and follow our Blog to see recent updates to the website.
(1) Sign up for our new Books email by subscribing to our Monthly Updates newsletter here. Every month, we will send you a list of new pathology related books with a short summary and link to Amazon.com and the publisher for further information. The email is free, and you can unsubscribe at any time.
Visit and follow our Blog to see recent updates to the website.
Case #84
Clinical history:
A 58 year old woman with no prior history presented with chronic sinusitis and underwent functional endoscopic sinus surgery (FESS).
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Sinonasal hemangiopericytoma
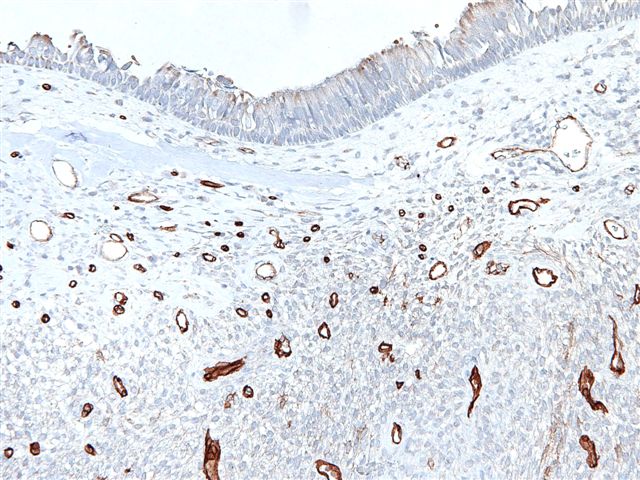
Immunostains:
CD34
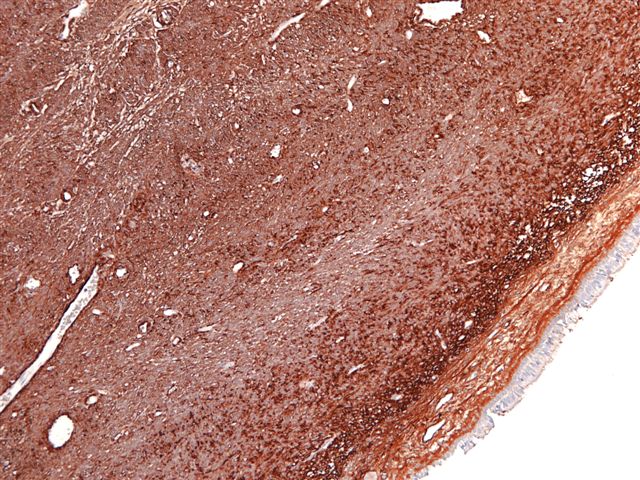
Smooth muscle actin
Discussion:
The specimen shows surface respiratory epithelium overlying the diffuse growth of bland spindled or round / oval cells. There are prominent blood vessels with a staghorn appearance and perivascular hyalinization. There is no / mild atypia, no necrosis and no significant mitotic activity. The CD34 immunostain highlights the vascular endothelium but not the tumor cells. However, the tumor cells are strongly immunoreactive for smooth muscle actin.
Sinonasal hemangiopericytoma is an uncommon tumor of pericytic myoid differentiation. The World Health Organization calls it glomangiopericytoma and others have suggested it be called myopericytoma (J Laryngol Otol 2008;122:403). It typically affects older adults, with a mean age of 63 years but may occur in children. There is often a history of airway obstruction or epistaxis in the nasal cavity or paranasal sinuses.
The histology in this case is typical. In addition, there is often a prominent inflammatory infiltrate containing eosinophils and mast cells.
Almost all cases are immunoreactive for vimentin and smooth muscle actin, with less common staining for muscle specific actin (77%) and factor XIIIa (78%). The tumor cells are negative for cytokeratin and usually for the vascular markers CD31, CD34 and factor VIII.
Electron microscopy shows that these tumors have true pericytic differentiation, with numerous intracytoplasmic thin filaments with dense bodies, irregular basement membrane-like materials, a continuous basement membrane separating tumor cells from capillaries and occasional intercellular junctions.
The differential diagnosis includes lobular capillary hemangioma, solitary fibrous tumor and glomus tumor. Lobular capillary hemangioma has a low power lobular pattern. Although spindled fibroblasts and blood vessels are prominent, the overall picture resembles granulation tissue and capillaries are small. Solitary fibrous tumor has a patternless pattern, with ropey keloid type collagen. The vascular pattern is similar to sinonasal hemangiopericytoma but a recent study found that the vessels in sinonasal hemangiopericytoma were always D2-40 positive (a marker of lymphatic endothelium) in contrast to solitary fibrous tumors / soft tissue hemangiopericytomas, which were always D2-40 negative (Virchows Arch 2006;448:459). Finally, although a glomus tumor is also a pericytic tumor and has a similar staining pattern, it is extremely rare in the sinonasal region. In addition, its morphology is different, as it typically is composed of compact epithelioid cells.
Excision of sinonasal hemangiopericytoma is adequate treatment. However, since these tumors recur 18% of the time, follow up is necessary. There are no metastases and these tumors only rarely cause death.
References: Am J Surg Pathol 2003;27:737, Arch Pathol Lab Med 2001;125:686