3 May 2007 - Case #82
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California (USA).

Peloris rapid tissue processing
This case is sponsored by Vision BioSystems and its Peloris rapid tissue processing. Peloris is a rapid tissue processor that creates high quality results for any tissue. It has a xylene-free option and a unique ActivFlo system that generates ideal processing conditions. A range of Peloris consumables adds extra value with cassettes that eliminate biopsy pads, solid Parablocks wax for easy, safe wax transfer and reagents to completely eliminate xylene. With Peloris, any laboratory can enjoy the confidence of high quality results while meeting new workflow challenges like reduced turnaround times, Lean production and same day diagnosis.
Peloris is part of Vision BioSystems Lean Histology range and it is ideal for laboratories pursuing Lean and six sigma principles.
Advertisement
Case #82
Clinical history:
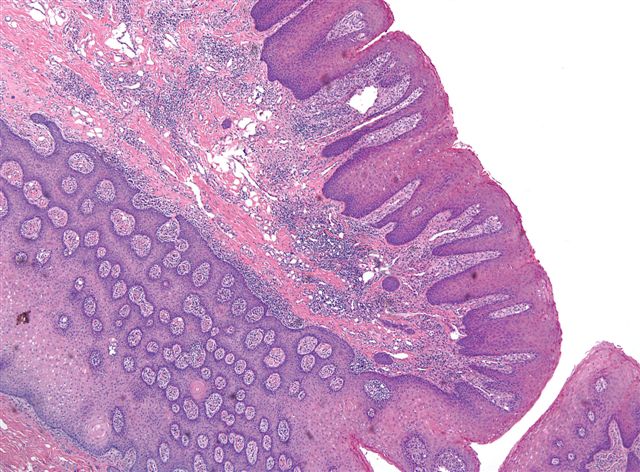
A 57 year old man had papillary lesions on his palate, which were excised.
Microscopic images:

What is your diagnosis?
Diagnosis: Verruciform xanthoma
Discussion:
Verruciform xanthoma is a rare lesion of the oral mucosa that usually occurs in the gingiva or alveolar ridge. It occurs less commonly on the penis or scrotum. It is considered reactive, although a multifocal lesion was reported in a child with a systemic lipid disorder (Am J Surg Pathol 1998;22:479, Am J Surg Pathol 1989;13:309). It is probably not HPV related (APMIS 2005;113:629, Arch Pathol Lab Med 2005;129:e62, Am J Dermatopathol 2000;22:447).
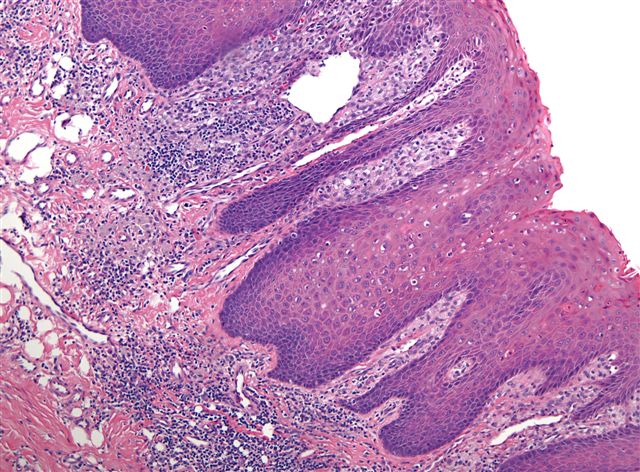
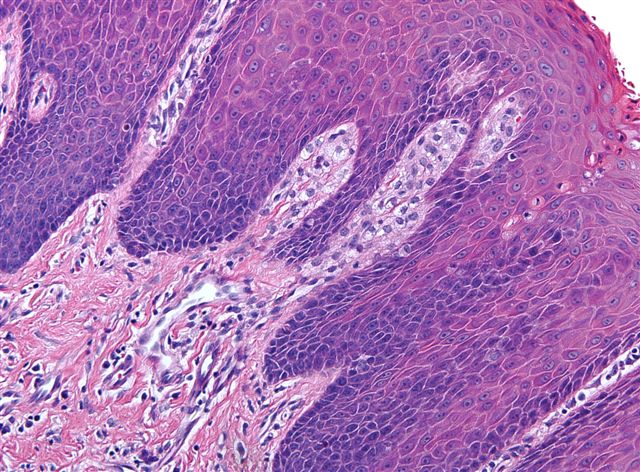
Grossly, verruciform xanthoma appears as a raised granular or verrucous lesion. Histologically, the characteristic finding is foamy macrophages within dermal papillae. The foam cells are immunoreactive for CD68, vimentin and factor XIIIa and negative for S100 and weak / negative for keratin. The overlying epidermis is either verruciform, papillary or flat (Oral Oncol 2003;39:325). No epithelial atypia is present.
The differential diagnosis includes squamous cell carcinoma, verrucous carcinoma and condyloma acuminatum. All of these entities lack prominent foamy macrophages. In addition, the lack of atypia rules out squamous cell carcinoma. Verrucous carcinoma is composed of lobules of mature squamous epithelium with minimal atypia but they are ulcerating or fungating. Condyloma acuminatum has prominent koilocytosis in the upper epidermis that is not found in verruciform xanthoma.
Excision is adequate treatment and these tumors do not recur (J Formos Med Assoc 2007;106:141).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California (USA).
This case is sponsored by Vision BioSystems and its Peloris rapid tissue processing. Peloris is a rapid tissue processor that creates high quality results for any tissue. It has a xylene-free option and a unique ActivFlo system that generates ideal processing conditions. A range of Peloris consumables adds extra value with cassettes that eliminate biopsy pads, solid Parablocks wax for easy, safe wax transfer and reagents to completely eliminate xylene. With Peloris, any laboratory can enjoy the confidence of high quality results while meeting new workflow challenges like reduced turnaround times, Lean production and same day diagnosis.
Peloris is part of Vision BioSystems Lean Histology range and it is ideal for laboratories pursuing Lean and six sigma principles.
Website news:
(1) Visit our Stains chapter for our recently expanded coverage of all of the cytokeratins, with hundreds of new references and image links.
(2) We also recently added a new article on "Pricing for Pathology billing" to the Management chapter.
Visit and follow our Blog to see recent updates to the website.
(1) Visit our Stains chapter for our recently expanded coverage of all of the cytokeratins, with hundreds of new references and image links.
(2) We also recently added a new article on "Pricing for Pathology billing" to the Management chapter.
Visit and follow our Blog to see recent updates to the website.
Case #82
Clinical history:
A 57 year old man had papillary lesions on his palate, which were excised.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Verruciform xanthoma
Discussion:
Verruciform xanthoma is a rare lesion of the oral mucosa that usually occurs in the gingiva or alveolar ridge. It occurs less commonly on the penis or scrotum. It is considered reactive, although a multifocal lesion was reported in a child with a systemic lipid disorder (Am J Surg Pathol 1998;22:479, Am J Surg Pathol 1989;13:309). It is probably not HPV related (APMIS 2005;113:629, Arch Pathol Lab Med 2005;129:e62, Am J Dermatopathol 2000;22:447).
Grossly, verruciform xanthoma appears as a raised granular or verrucous lesion. Histologically, the characteristic finding is foamy macrophages within dermal papillae. The foam cells are immunoreactive for CD68, vimentin and factor XIIIa and negative for S100 and weak / negative for keratin. The overlying epidermis is either verruciform, papillary or flat (Oral Oncol 2003;39:325). No epithelial atypia is present.
The differential diagnosis includes squamous cell carcinoma, verrucous carcinoma and condyloma acuminatum. All of these entities lack prominent foamy macrophages. In addition, the lack of atypia rules out squamous cell carcinoma. Verrucous carcinoma is composed of lobules of mature squamous epithelium with minimal atypia but they are ulcerating or fungating. Condyloma acuminatum has prominent koilocytosis in the upper epidermis that is not found in verruciform xanthoma.
Excision is adequate treatment and these tumors do not recur (J Formos Med Assoc 2007;106:141).