12 April 2007 - Case #80
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Alia Albawardi, Faculty of Medicine & Health Sciences, United Arab Emirates University (UAE).
Case #80
Clinical history:
A 28 year old man had a red nodule on the left thigh for 6 months that was slowly growing. The clinical suspicion was Kaposi sarcoma.
Microscopic images:
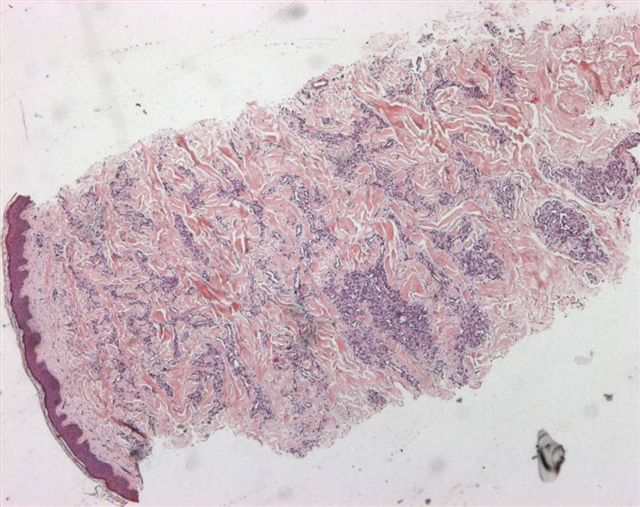
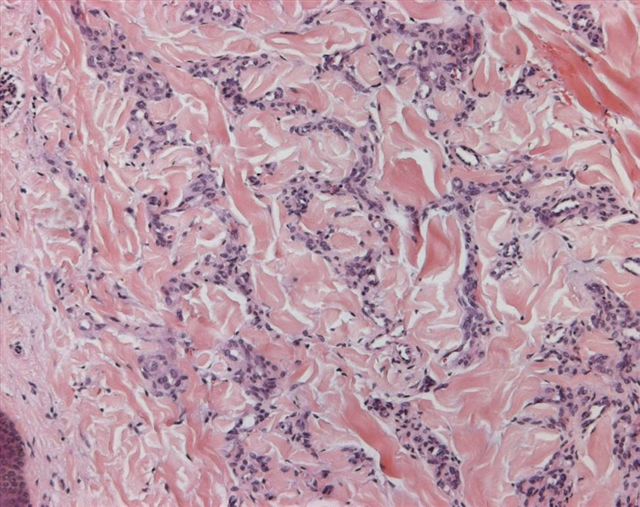
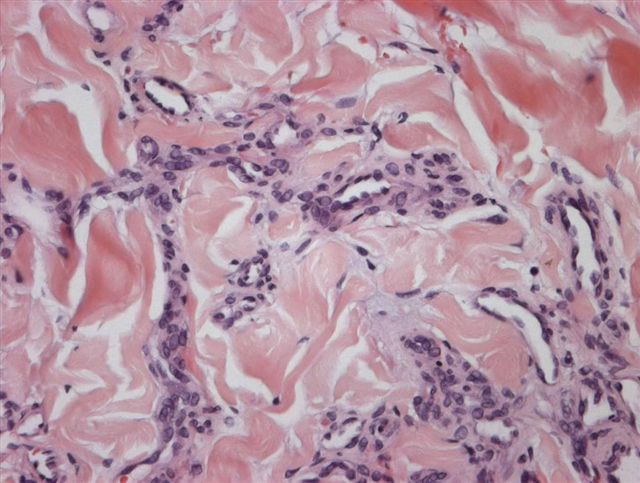
What is your diagnosis?
Diagnosis: Microvenular hemangioma
Discussion:
Microvenular hemangioma was first described by Hunt in 1991 (J Cutan Pathol 1991;18:235). It is rare, with < 50 cases reported. It presents as a slow growing, solitary, asymptomatic, purple-red papule or plaque in young to middle aged adults, often on the trunk or limbs. The histology shows a dermal proliferation of small, irregular branching capillaries and venules with inconspicuous lumina. Endothelial cells may be plump but no atypia is present. The stroma is collagenous. No spindle cells are present.
The endothelial cells are immunoreactive for CD34 and factor VIII related antigen. Smooth muscle actin highlights pericytes surrounding the endothelial cells.
The main differential diagnosis is patch stage Kaposi sarcoma, which also has irregular vascular spaces. However, they are anastomosing and not collapsed and are accompanied by atypical endothelial cells, eosinophilic hyaline globules, plasma cells and fascicles of spindle cells. There may be irregular dissection of collagen bundles by vessels. The spindle cells are HHV8 positive and the patients are HIV positive, which is usually helpful (Am J Clin Pathol 2004;121:335). However, there was a recent report of HHV8 positive microvenular hemangioma in an unusual case of POEMS syndrome (Arch Pathol Lab Med 2003;127:1034).
Kaposiform hemangioendothelioma also has slit-like lumina, although they are due to nodules and sheets of compact spindle cells. It affects the skin or retroperitoneum of infants and children and may be associated with severe coagulopathy.
Microvenular hemangioma is a benign lesion. To date, excision appears to be curative.
References: Dermatology 2003;206:161, Pathol Int 1998;48:237
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Alia Albawardi, Faculty of Medicine & Health Sciences, United Arab Emirates University (UAE).
Website news:
(1) In response to many inquiries, we will never charge our users or require registration for PathologyOutlines.com. We believe the Internet should be free to all, and in fact, are trying to convince more pathology journals to make their content “free full text” without registration, at least for the older issues.
Visit and follow our Blog to see recent updates to the website.
(1) In response to many inquiries, we will never charge our users or require registration for PathologyOutlines.com. We believe the Internet should be free to all, and in fact, are trying to convince more pathology journals to make their content “free full text” without registration, at least for the older issues.
Visit and follow our Blog to see recent updates to the website.
Case #80
Clinical history:
A 28 year old man had a red nodule on the left thigh for 6 months that was slowly growing. The clinical suspicion was Kaposi sarcoma.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Microvenular hemangioma
Discussion:
Microvenular hemangioma was first described by Hunt in 1991 (J Cutan Pathol 1991;18:235). It is rare, with < 50 cases reported. It presents as a slow growing, solitary, asymptomatic, purple-red papule or plaque in young to middle aged adults, often on the trunk or limbs. The histology shows a dermal proliferation of small, irregular branching capillaries and venules with inconspicuous lumina. Endothelial cells may be plump but no atypia is present. The stroma is collagenous. No spindle cells are present.
The endothelial cells are immunoreactive for CD34 and factor VIII related antigen. Smooth muscle actin highlights pericytes surrounding the endothelial cells.
The main differential diagnosis is patch stage Kaposi sarcoma, which also has irregular vascular spaces. However, they are anastomosing and not collapsed and are accompanied by atypical endothelial cells, eosinophilic hyaline globules, plasma cells and fascicles of spindle cells. There may be irregular dissection of collagen bundles by vessels. The spindle cells are HHV8 positive and the patients are HIV positive, which is usually helpful (Am J Clin Pathol 2004;121:335). However, there was a recent report of HHV8 positive microvenular hemangioma in an unusual case of POEMS syndrome (Arch Pathol Lab Med 2003;127:1034).
Kaposiform hemangioendothelioma also has slit-like lumina, although they are due to nodules and sheets of compact spindle cells. It affects the skin or retroperitoneum of infants and children and may be associated with severe coagulopathy.
Microvenular hemangioma is a benign lesion. To date, excision appears to be curative.
References: Dermatology 2003;206:161, Pathol Int 1998;48:237