


15 March 2007 - Case #77
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Vladimir Osipov, Medical College of Wisconsin, Milwaukee, Wisconsin (USA).

The Business Solution for Pathology
Is Your Pathology Practice Seeking to Gain a Competitive Advantage? PSA supports visionaries and leading pathology practices seeking to gain a competitive advantage within their markets. Formed exclusively for pathologists by pathologists, PSA is a leading provider of Pathology Billing and Collection Services, Pathology Practice Marketing Support, and Pathology Business Support Services.
Advertisement
Case #77
Clinical history:
A 55 year old man had a thigh mass measuring 10 cm, which was excised.
Microscopic images:



What is your diagnosis?
Diagnosis: Epithelioid hemangioendothelioma (malignant)
Discussion:
Epithelioid hemangioendotheliomas (EHE) are intermediate grade vascular malignancies that are closely associated with or arise from a vein in 50% of cases. They occur in various organs and soft tissue, including the skin, lung, liver and bone.
The tumors are composed of cords or small nests of round endothelial cells with abundant eosinophilic cytoplasm. Tumors that arise from vessels extend outward from the lumen towards soft tissue. The tumor cells often have intracytoplasmic vacuoles representing small vascular lumina and which may resemble mucin. The nuclei are round and may be indented. In most cases, there is minimal mitotic activity, atypia or necrosis. However, about 25% of cases exhibit frank malignant features of prominent nuclear pleomorphism (as in this case), mitotic activity, focal spindling or necrosis. The stroma may be scanty or myxoid, as in this case.
Tumor cells are immunoreactive for vascular markers, including CD31 and von Willebrand factor and are often positive focally for keratin. The reticulin stain demonstrates that nests and cords of cells are invested by a reticulin sheath. Occasional tumors may demonstrate t(1;3)(p36.3;q25) (Am J Surg Pathol 2001;25:684).
The differential diagnosis includes metastatic carcinoma, epithelioid sarcoma and epithelioid angiosarcoma. Carcinomas usually exhibit more marked atypia and mitotic activity. They are usually not angiocentric and are negative for vascular markers. Epithelioid sarcoma develops on the distal extremities of young individuals and its tumor cells merge and blend with the collagenous stroma. These tumors are strongly keratin positive and negative for factor VIII related antigen, although they are often CD34 positive and rarely CD31 positive (Virchows Arch A Pathol Anat Histopathol 1987;410:309, Histopathology 1998;33:425, Virchows Arch 2003;443:93). Epithelioid angiosarcoma is composed of solid sheets of cells with marked atypia and prominent mitotic figures, accompanied by necrosis and irregular sinusoidal vascular channels.
For tumors with low histologic grade, recommended treatment is wide local excision. Tumors of high histologic grade, as in this case, tend to have more aggressive behavior. As a result, radical local excision is recommended and node dissections may be helpful. Epithelioid hemangioendothelioma has an unpredictable clinical course that is less aggressive than angiosarcoma but still causes frequent recurrence (13%), metastases (20 - 30%) and death due to disease (13%) (Am J Surg Pathol 1997;21:363).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Vladimir Osipov, Medical College of Wisconsin, Milwaukee, Wisconsin (USA).
Is Your Pathology Practice Seeking to Gain a Competitive Advantage? PSA supports visionaries and leading pathology practices seeking to gain a competitive advantage within their markets. Formed exclusively for pathologists by pathologists, PSA is a leading provider of Pathology Billing and Collection Services, Pathology Practice Marketing Support, and Pathology Business Support Services.
Case #77
Clinical history:
A 55 year old man had a thigh mass measuring 10 cm, which was excised.
Microscopic images:
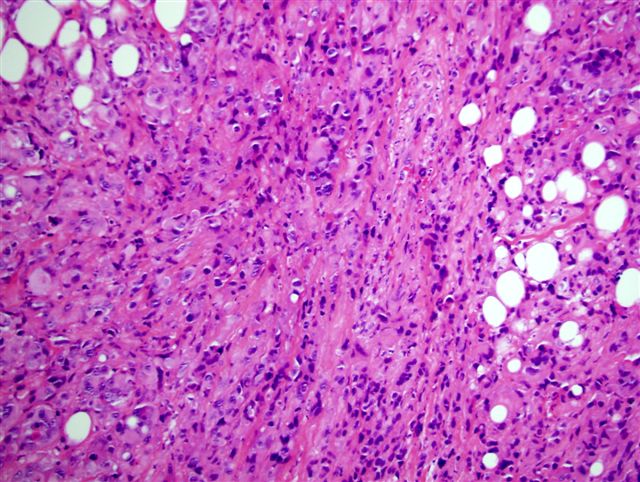
Low power
Medium power
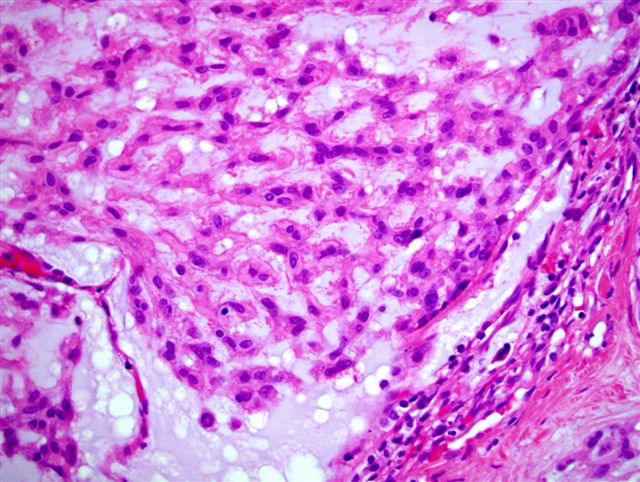
High power
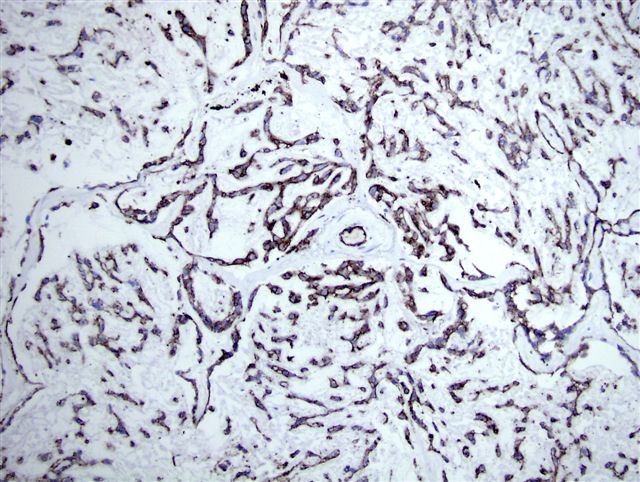
CD31
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Epithelioid hemangioendothelioma (malignant)
Discussion:
Epithelioid hemangioendotheliomas (EHE) are intermediate grade vascular malignancies that are closely associated with or arise from a vein in 50% of cases. They occur in various organs and soft tissue, including the skin, lung, liver and bone.
The tumors are composed of cords or small nests of round endothelial cells with abundant eosinophilic cytoplasm. Tumors that arise from vessels extend outward from the lumen towards soft tissue. The tumor cells often have intracytoplasmic vacuoles representing small vascular lumina and which may resemble mucin. The nuclei are round and may be indented. In most cases, there is minimal mitotic activity, atypia or necrosis. However, about 25% of cases exhibit frank malignant features of prominent nuclear pleomorphism (as in this case), mitotic activity, focal spindling or necrosis. The stroma may be scanty or myxoid, as in this case.
Tumor cells are immunoreactive for vascular markers, including CD31 and von Willebrand factor and are often positive focally for keratin. The reticulin stain demonstrates that nests and cords of cells are invested by a reticulin sheath. Occasional tumors may demonstrate t(1;3)(p36.3;q25) (Am J Surg Pathol 2001;25:684).
The differential diagnosis includes metastatic carcinoma, epithelioid sarcoma and epithelioid angiosarcoma. Carcinomas usually exhibit more marked atypia and mitotic activity. They are usually not angiocentric and are negative for vascular markers. Epithelioid sarcoma develops on the distal extremities of young individuals and its tumor cells merge and blend with the collagenous stroma. These tumors are strongly keratin positive and negative for factor VIII related antigen, although they are often CD34 positive and rarely CD31 positive (Virchows Arch A Pathol Anat Histopathol 1987;410:309, Histopathology 1998;33:425, Virchows Arch 2003;443:93). Epithelioid angiosarcoma is composed of solid sheets of cells with marked atypia and prominent mitotic figures, accompanied by necrosis and irregular sinusoidal vascular channels.
For tumors with low histologic grade, recommended treatment is wide local excision. Tumors of high histologic grade, as in this case, tend to have more aggressive behavior. As a result, radical local excision is recommended and node dissections may be helpful. Epithelioid hemangioendothelioma has an unpredictable clinical course that is less aggressive than angiosarcoma but still causes frequent recurrence (13%), metastases (20 - 30%) and death due to disease (13%) (Am J Surg Pathol 1997;21:363).
