1 March 2007 - Case #75
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Sungmi Jung, University of Pennsylvania Health System, Philadelphia, Pennsylvania (USA).

The Business Solution for Pathology™
This email is sponsored by Pathology Service Associates, LLC (PSA). Visit PSA at the American Pathology Foundation Spring Conference, March 1-2, 2007.
Is Your Pathology Practice Seeking to Gain a Competitive Advantage? PSA supports visionaries and leading pathology practices seeking to gain a competitive advantage within their markets. Formed exclusively for pathologists by pathologists, PSA is a leading provider of Pathology Billing and Collection Services, Pathology Practice Marketing Support, and Pathology Business Support Services.
Advertisement
Case #75
Clinical history:
A 57 year old man had a history of worsening headache with no focal neurologic signs. An MRI showed a 4.5 cm heterogeneous intraventricular mass causing obstructive hydrocephalus. The radiologic impression was a central neurocytoma.
Radiology image:

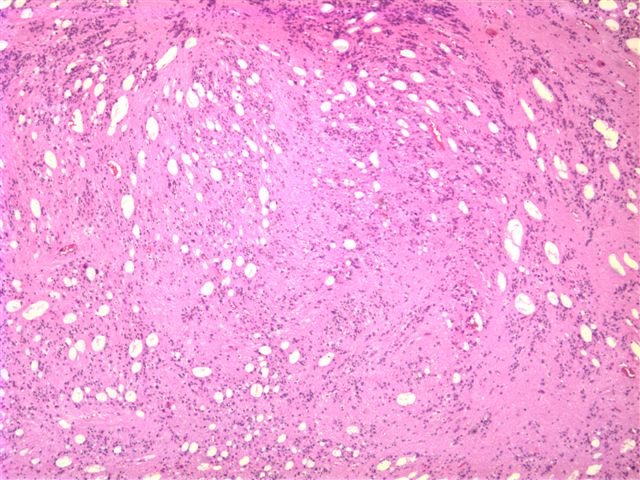
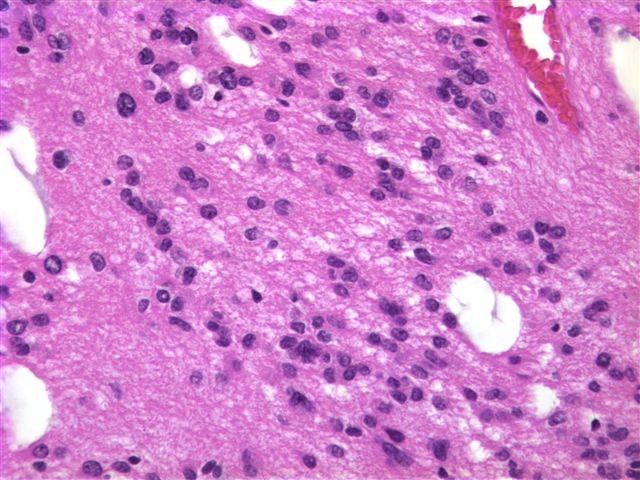
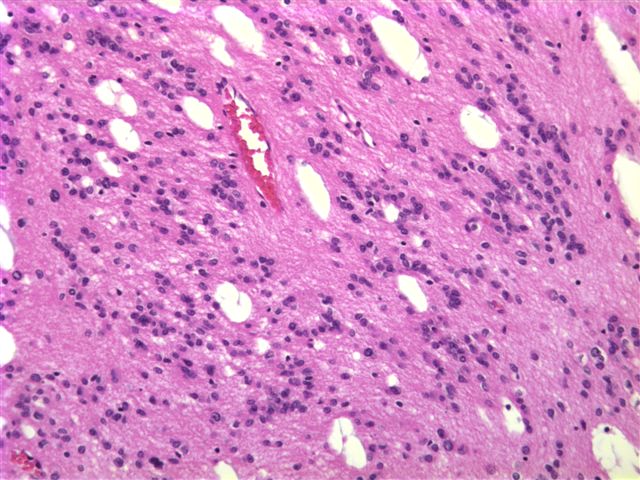
Microscopic images:
What is your diagnosis?
Diagnosis: Subependymoma
Discussion:
Subependymoma is a low grade CNS glial tumor of middle aged to elderly adults with a distinctive appearance and benign behavior (WHO grade I of IV). It usually occurs in the fourth ventricle or lateral ventricles, where it is often an incidental finding at autopsy or in the spinal cord, where it presents as a myelopathy.
Grossly, the tumors are well circumscribed, solid, gray-white and protrude into the lateral ventricles or fourth ventricle. Calcification is common. The tumors consist of small ependymal type cells in a dense glial, fibrillary background with prominent microcysts and mild nuclear pleomorphism. There may be occasional ependymal rosettes. There is no endothelial proliferation or necrosis. Cytology smears show bland tumor cells with prominent microcysts (Acta Cytol 2001;45:636). Tumor cells are almost uniformly immunoreactive for GFAP, NSE and NCAM but have a low Ki67 index (J Neurooncol 2005;74:1). Tumors with a prominent ependymal component are often classified as mixed tumors and are more aggressive than subependymomas, with a WHO grade of II of IV.
The differential diagnosis includes tanycytic ependymoma (grade II of IV), which also has astrocytic features, as well as distinctive zones either with abundant nuclei and relatively free of nuclei.
Excision is usually curative, although radiation is occasionally given.
References: Neurol India 2003;51:98, Neurol Med Chir (Tokyo) 2002;42:349
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Sungmi Jung, University of Pennsylvania Health System, Philadelphia, Pennsylvania (USA).
The Business Solution for Pathology™
This email is sponsored by Pathology Service Associates, LLC (PSA). Visit PSA at the American Pathology Foundation Spring Conference, March 1-2, 2007.
Is Your Pathology Practice Seeking to Gain a Competitive Advantage? PSA supports visionaries and leading pathology practices seeking to gain a competitive advantage within their markets. Formed exclusively for pathologists by pathologists, PSA is a leading provider of Pathology Billing and Collection Services, Pathology Practice Marketing Support, and Pathology Business Support Services.
Case #75
Clinical history:
A 57 year old man had a history of worsening headache with no focal neurologic signs. An MRI showed a 4.5 cm heterogeneous intraventricular mass causing obstructive hydrocephalus. The radiologic impression was a central neurocytoma.
Radiology image:
MRI
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Subependymoma
Discussion:
Subependymoma is a low grade CNS glial tumor of middle aged to elderly adults with a distinctive appearance and benign behavior (WHO grade I of IV). It usually occurs in the fourth ventricle or lateral ventricles, where it is often an incidental finding at autopsy or in the spinal cord, where it presents as a myelopathy.
Grossly, the tumors are well circumscribed, solid, gray-white and protrude into the lateral ventricles or fourth ventricle. Calcification is common. The tumors consist of small ependymal type cells in a dense glial, fibrillary background with prominent microcysts and mild nuclear pleomorphism. There may be occasional ependymal rosettes. There is no endothelial proliferation or necrosis. Cytology smears show bland tumor cells with prominent microcysts (Acta Cytol 2001;45:636). Tumor cells are almost uniformly immunoreactive for GFAP, NSE and NCAM but have a low Ki67 index (J Neurooncol 2005;74:1). Tumors with a prominent ependymal component are often classified as mixed tumors and are more aggressive than subependymomas, with a WHO grade of II of IV.
The differential diagnosis includes tanycytic ependymoma (grade II of IV), which also has astrocytic features, as well as distinctive zones either with abundant nuclei and relatively free of nuclei.
Excision is usually curative, although radiation is occasionally given.
References: Neurol India 2003;51:98, Neurol Med Chir (Tokyo) 2002;42:349