
8 February 2007 - Case #73
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Juan José Segura Fonseca, Hospital San Juan de Dios, San José, Costa Rica.

The Business Solution for Pathology™
This email is sponsored by Pathology Service Associates, LLC (PSA), who invites you, and members of your practice, to participate in the PSA hosted Audio Conference titled “Specialty Physicians are Competing for Your Pathology Revenue, How Will Your Practice Respond and Maintain Business?” This call will be presented by Jane Pine Wood, Esq., of McDonald Hopkins Co., LPA, and Al Sirmon, CPA, President and Chief Executive Officer of PSA, LLC. 1.5 CME credits have been designated for this call.
Advertisement
Case #73
Clinical history:
A 66 year old man was admitted with a history of enlargement of the right mandible for several months, associated with pain and loosening of several teeth. A small fistulous tract was draining into the mucosa. Xrays disclosed an extensive lytic and cyst-like lesion that involved almost the entire right mandible. A surgical curettage was done.
Radiology image:

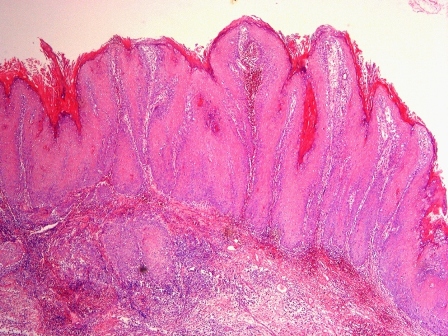
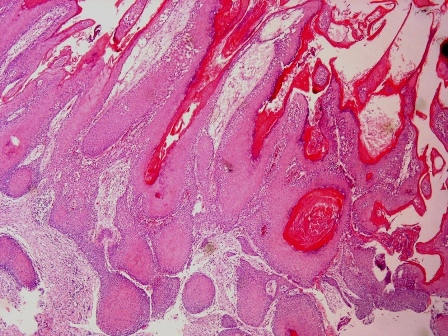
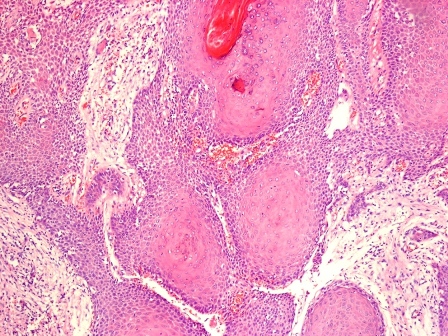
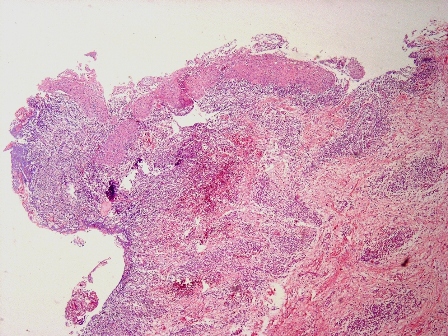
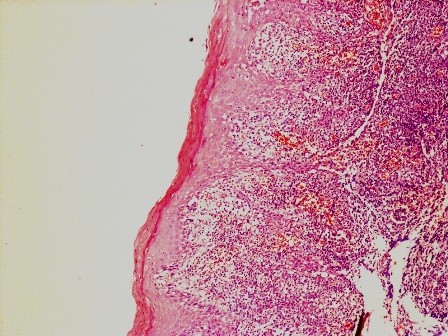
Microscopic images:

What is your diagnosis?
Diagnosis: Primary intraosseous odontogenic verrucous carcinoma of the mandible arising in a dentigerous cyst
Discussion:
Low and medium power magnifications show squamous epithelium with marked papillomatous and acantholytic hyperplasia. Superficial stromal invasion by solid nests of well differentiated squamous carcinoma is present. A residual squamous epithelial lining with chronic inflammation, belonging to a dentigerous cyst, is present.
This is one of the few cases of verrucous carcinoma arising as a primary intraosseous odontogenic carcinoma of the mandible or maxilla within a dentigerous cyst (a cyst that surrounds the crown of an impacted tooth) (Tumori 2001;87:444, Oral Surg Oral Med Oral Pathol 1980;49:151). Primary intraosseous odontogenic carcinomas are usually squamous cell carcinomas within the jaw, without a connection to oral mucosa. They develop from the epithelial lining of an odontogenic cyst or de novo from intraosseous odontogenic rests (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:194). The mean patient age is 52 years (range 4 to 76 years), with 70% occurring in men (Int J Oral Maxillofac Surg 2001;30:349). Most tumors (92%) occur in the mandible.
Clinically, primary intraosseous odontogenic carcinoma is characterized by progressive swelling of the jaw, pain and loosening of the teeth. Xrays show a fully radiolucent cystic-like pattern of bone destruction but with well defined margins. The histology is usually a high grade squamous cell carcinoma with aggressive behavior and a destructive pattern. Cervical nodal metastases are common and 50% of cases recur within 2 years. Aggressive surgical excision is recommended, possibly with postoperative radiotherapy (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:e29). The overall 2 and 4 year survival is 60% and 40% respectively.
Verrucous carcinoma was initially described as a type of epidermoid carcinoma of the oral cavity by Ackerman (Surgery 1948;23:670). It is a warty, papillomatous, exophytic white tumor of the oral mucosa. Histologically, it has proliferating, papillomatous, well differentiated squamous epithelium with no cytological atypia. The margins are rounded and invasion is superficial with pushing borders. Destructive and deep stromal invasion is not present. The differential diagnosis includes verrucous proliferation without invasion (J Oral Pathol Med 2002;31:500).
References: J Craniomaxillofac Surg 2004;32:166, Rev Stomatol Chir Maxillofac 2003;104:265, Oral Oncol 2000;36:305, Indian J Dent Res 2004;15:103
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Juan José Segura Fonseca, Hospital San Juan de Dios, San José, Costa Rica.
The Business Solution for Pathology™
This email is sponsored by Pathology Service Associates, LLC (PSA), who invites you, and members of your practice, to participate in the PSA hosted Audio Conference titled “Specialty Physicians are Competing for Your Pathology Revenue, How Will Your Practice Respond and Maintain Business?” This call will be presented by Jane Pine Wood, Esq., of McDonald Hopkins Co., LPA, and Al Sirmon, CPA, President and Chief Executive Officer of PSA, LLC. 1.5 CME credits have been designated for this call.
Case #73
Clinical history:
A 66 year old man was admitted with a history of enlargement of the right mandible for several months, associated with pain and loosening of several teeth. A small fistulous tract was draining into the mucosa. Xrays disclosed an extensive lytic and cyst-like lesion that involved almost the entire right mandible. A surgical curettage was done.
Radiology image:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Primary intraosseous odontogenic verrucous carcinoma of the mandible arising in a dentigerous cyst
Discussion:
Low and medium power magnifications show squamous epithelium with marked papillomatous and acantholytic hyperplasia. Superficial stromal invasion by solid nests of well differentiated squamous carcinoma is present. A residual squamous epithelial lining with chronic inflammation, belonging to a dentigerous cyst, is present.
This is one of the few cases of verrucous carcinoma arising as a primary intraosseous odontogenic carcinoma of the mandible or maxilla within a dentigerous cyst (a cyst that surrounds the crown of an impacted tooth) (Tumori 2001;87:444, Oral Surg Oral Med Oral Pathol 1980;49:151). Primary intraosseous odontogenic carcinomas are usually squamous cell carcinomas within the jaw, without a connection to oral mucosa. They develop from the epithelial lining of an odontogenic cyst or de novo from intraosseous odontogenic rests (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:194). The mean patient age is 52 years (range 4 to 76 years), with 70% occurring in men (Int J Oral Maxillofac Surg 2001;30:349). Most tumors (92%) occur in the mandible.
Clinically, primary intraosseous odontogenic carcinoma is characterized by progressive swelling of the jaw, pain and loosening of the teeth. Xrays show a fully radiolucent cystic-like pattern of bone destruction but with well defined margins. The histology is usually a high grade squamous cell carcinoma with aggressive behavior and a destructive pattern. Cervical nodal metastases are common and 50% of cases recur within 2 years. Aggressive surgical excision is recommended, possibly with postoperative radiotherapy (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:e29). The overall 2 and 4 year survival is 60% and 40% respectively.
Verrucous carcinoma was initially described as a type of epidermoid carcinoma of the oral cavity by Ackerman (Surgery 1948;23:670). It is a warty, papillomatous, exophytic white tumor of the oral mucosa. Histologically, it has proliferating, papillomatous, well differentiated squamous epithelium with no cytological atypia. The margins are rounded and invasion is superficial with pushing borders. Destructive and deep stromal invasion is not present. The differential diagnosis includes verrucous proliferation without invasion (J Oral Pathol Med 2002;31:500).
References: J Craniomaxillofac Surg 2004;32:166, Rev Stomatol Chir Maxillofac 2003;104:265, Oral Oncol 2000;36:305, Indian J Dent Res 2004;15:103
