10 January 2007 - Case #69
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Sharon Bihlmeyer, University of Vermont, Burlington, Vermont, USA.

Practice management services to increase your income
Case #69
Clinical history:
A 34 year old man had a scrotal abscess and underwent an incision and drainage procedure.
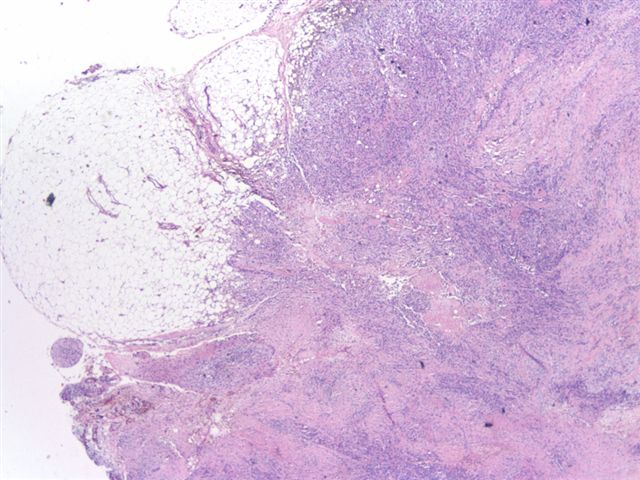
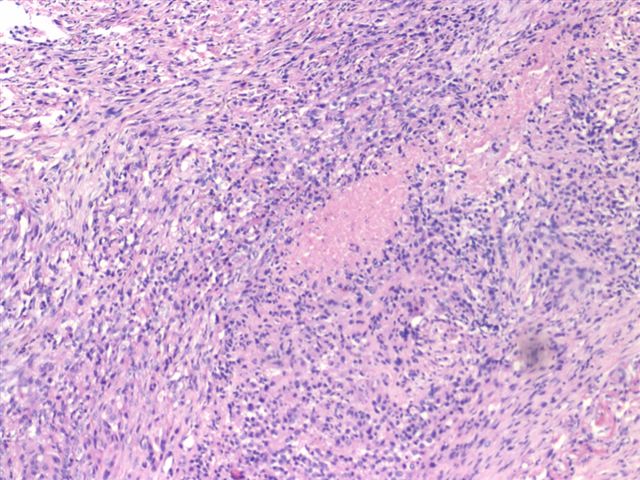
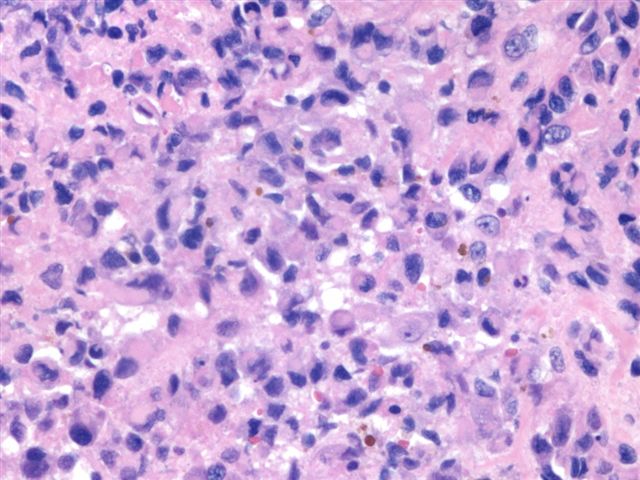
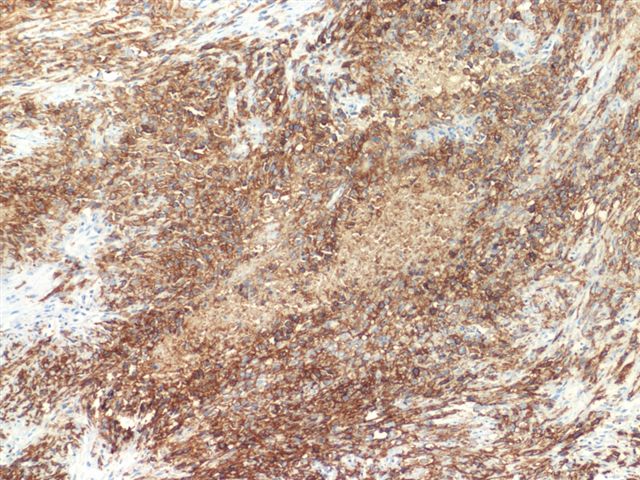
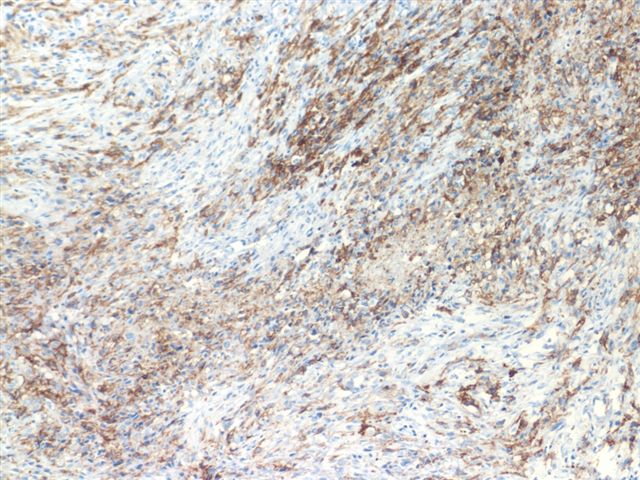
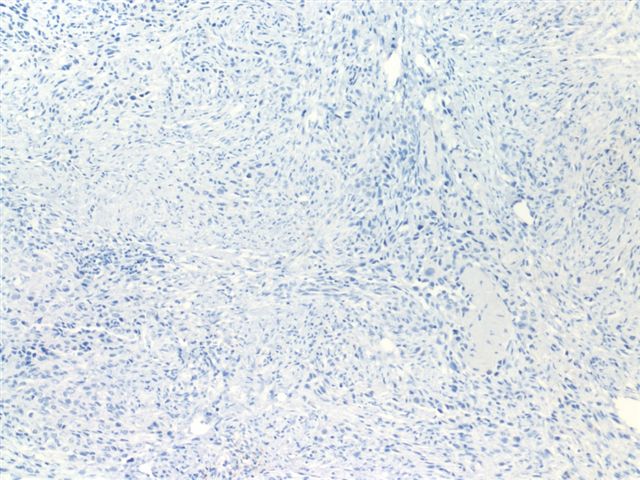
The specimen showed large areas of necrosis (image 1) and infiltrative margins (image 2). There were also granuloma-like areas (image 3) and rhabdoid-like cells (image 4). The tumor cells were immunoreactive for EMA (image 5) and CD34 (image 6) and negative for PLAP (image 7).
Microscopic images:

What is your diagnosis?
Diagnosis: Epithelioid sarcoma - reviewed by Dr. Chris Fletcher, who concurs
Stain images:
Discussion:
Epithelioid sarcoma is a rare soft tissue sarcoma, which typically presents as a subcutaneous or deep dermal mass in the distal extremities of individuals ages 10 - 35 years, with 67% occurring in males. They are often misdiagnosed due to their relatively bland initial appearance.
In 1997, Guillou described a more aggressive proximal type sarcoma that primarily involved the pelvis (Am J Surg Pathol 1997;21:130). These tumors are composed primarily of large epithelioid cells with more atypia than classic epithelioid sarcoma and often resemble a rhabdoid tumor due to intracytoplasmic hyaline inclusions. Large areas of necrosis and a multinodular pattern are common but a granuloma-like pattern is uncommon. The tumor cells are immunoreactive for keratin, EMA and vimentin, with variable immunostaining for desmin, CD34 and smooth muscle actin. They are negative for S100. The scrotum is an unusual site for epithelioid sarcoma, with only 2 case reports identified (Eur Urol 2006;49:406, Diagn Cytopathol 2001;24:36).
Enzinger and Weiss believe this tumor may be a variant of extrarenal malignant rhabdoid tumor (Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001). The differential diagnosis includes epithelioid malignant peripheral nerve sheath tumor (MPNST) (S100+, keratin-, rarely EMA+) and melanoma (S100+, usually HMB45+), as well as classic epithelioid sarcoma.
These tumors behave aggressively, with frequent metastases leading to death.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Sharon Bihlmeyer, University of Vermont, Burlington, Vermont, USA.
Practice management services to increase your income
Website news:
(1) This case is sponsored by Vachette Pathology. Imagine someone that solves your billing and payment problems, someone who guarantees to help you put more money back into your pocket. You do not have to change billing agents to increase your income. You simply have to manage the process. Who's watching your wallet?
Vachette Pathology is a Pathology Practice Management Firm, we are not a billing agency; what we do is manage your financial bloodline. We will push your billing process to optimum performance, renegotiate your manage care contracts and help with the business of pathology, all to ensure your financial future. For further information, please contact Mick Raich at: mraich@vachettepathology.com or call at 866-407-0763.
Visit and follow our Blog to see recent updates to the website.
(1) This case is sponsored by Vachette Pathology. Imagine someone that solves your billing and payment problems, someone who guarantees to help you put more money back into your pocket. You do not have to change billing agents to increase your income. You simply have to manage the process. Who's watching your wallet?
Vachette Pathology is a Pathology Practice Management Firm, we are not a billing agency; what we do is manage your financial bloodline. We will push your billing process to optimum performance, renegotiate your manage care contracts and help with the business of pathology, all to ensure your financial future. For further information, please contact Mick Raich at: mraich@vachettepathology.com or call at 866-407-0763.
Visit and follow our Blog to see recent updates to the website.
Case #69
Clinical history:
A 34 year old man had a scrotal abscess and underwent an incision and drainage procedure.
The specimen showed large areas of necrosis (image 1) and infiltrative margins (image 2). There were also granuloma-like areas (image 3) and rhabdoid-like cells (image 4). The tumor cells were immunoreactive for EMA (image 5) and CD34 (image 6) and negative for PLAP (image 7).
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Epithelioid sarcoma - reviewed by Dr. Chris Fletcher, who concurs
Stain images:
EMA
CD34
PLAP
Discussion:
Epithelioid sarcoma is a rare soft tissue sarcoma, which typically presents as a subcutaneous or deep dermal mass in the distal extremities of individuals ages 10 - 35 years, with 67% occurring in males. They are often misdiagnosed due to their relatively bland initial appearance.
In 1997, Guillou described a more aggressive proximal type sarcoma that primarily involved the pelvis (Am J Surg Pathol 1997;21:130). These tumors are composed primarily of large epithelioid cells with more atypia than classic epithelioid sarcoma and often resemble a rhabdoid tumor due to intracytoplasmic hyaline inclusions. Large areas of necrosis and a multinodular pattern are common but a granuloma-like pattern is uncommon. The tumor cells are immunoreactive for keratin, EMA and vimentin, with variable immunostaining for desmin, CD34 and smooth muscle actin. They are negative for S100. The scrotum is an unusual site for epithelioid sarcoma, with only 2 case reports identified (Eur Urol 2006;49:406, Diagn Cytopathol 2001;24:36).
Enzinger and Weiss believe this tumor may be a variant of extrarenal malignant rhabdoid tumor (Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001). The differential diagnosis includes epithelioid malignant peripheral nerve sheath tumor (MPNST) (S100+, keratin-, rarely EMA+) and melanoma (S100+, usually HMB45+), as well as classic epithelioid sarcoma.
These tumors behave aggressively, with frequent metastases leading to death.