15 November 2007 - Case #101
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California (USA).

ARUP Laboratories’ Surgical Pathology Workshop is scheduled for January 27 to February 1, 2008 at the Shadow Ridge Resort Hotel in Park City, Utah.
This five-day course is designed to address the activities and issues faced by the surgical pathologist – featuring short lectures and case-oriented discussions led by distinguished faculty from the University of Utah and ARUP Laboratories.
University of Utah School of Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing medical education for physicians.
Advertisement
Case #101
Clinical history:
A 40 year woman with nasal sinus congestion had a CT scan, which showed a mass. Endoscopy showed friable nasal tissue. A biopsy was obtained.
Microscopic images:


What is your diagnosis?
Diagnosis: NK / T cell lymphoma, nasal type
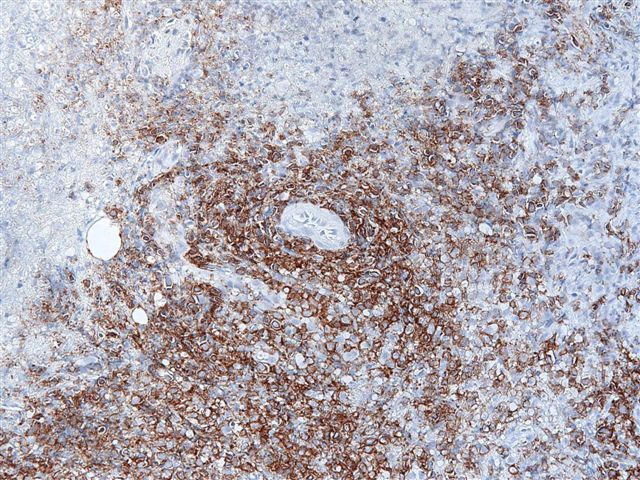
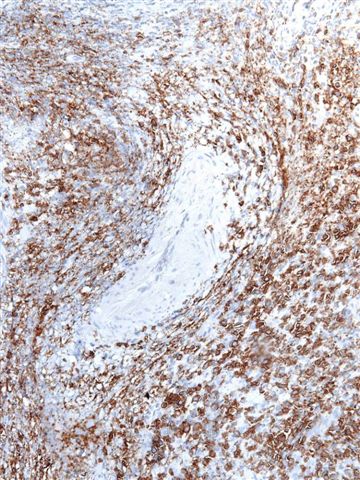
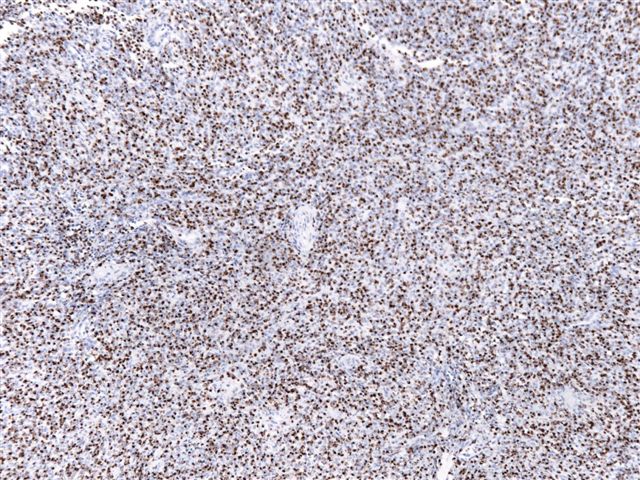
Immunostains:


Discussion:
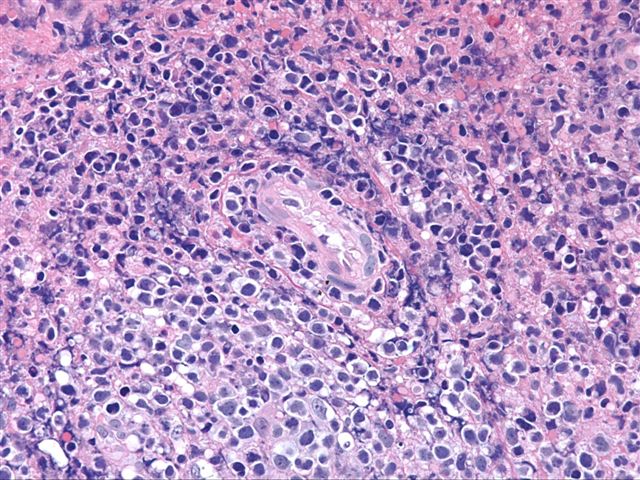
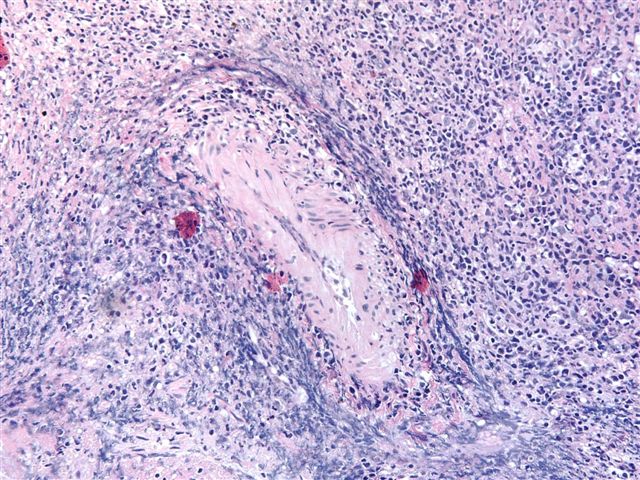
The low power images show large areas of necrosis. Higher power images show an angiocentric pattern of pleomorphic tumor cells with hyperchromatic nuclei and occasional perinuclear clearing. There is prominent angiodestruction, although the vessel walls lack neutrophils or fibrinoid necrosis.
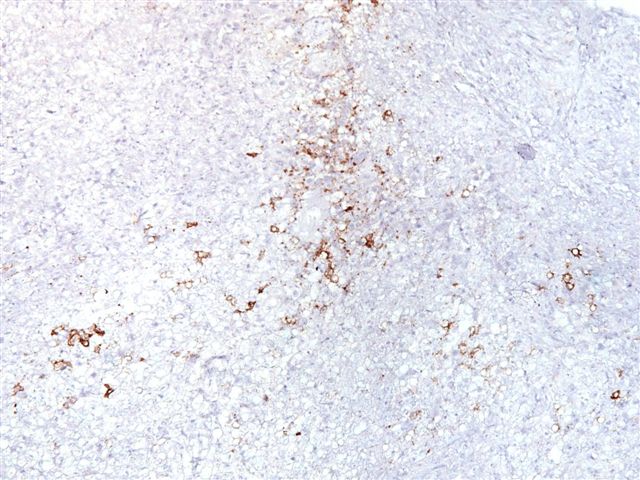
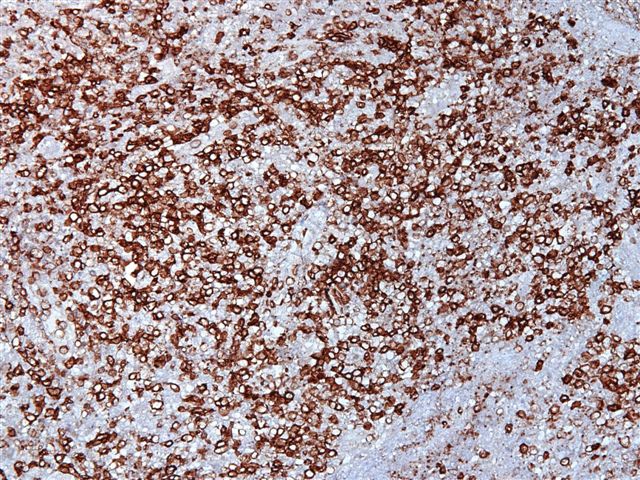
The tumor cells are negative for a cytokeratin cocktail, although some residual epithelial cells / vessels are positive. Most tumor cells are immunoreactive for the T cell marker CD3 (cytoplasmic staining) but negative for the B cell marker CD20. There is strong staining for the NK marker CD56, Epstein-Barr virus (by in situ hybridization) and TIA, a marker of activated cytotoxic T cells.
NK / T cell lymphomas (nasal type) were previously called angiocentric lymphoma or polymorphic reticulosis. They commonly present as a destructive nasal or midline facial tumor. In the U.S. they are rare and usually affect patients of Asian or Hispanic descent (Am J Surg Pathol 2000;24:1511). Outside the U.S., they are more common in Asia, Central and South America (Ai Zheng 2007;26:1170, Hum Path 2004;35:86, Appl Immunohistochem Mol Morphol 2007;15:38). Non-nasal NK / T cell lymphomas are similar and often present in the GI tract, skin and testis.
The tumor cells are positive for T cell markers CD2 and CD3 (cytoplasmic but not nuclear staining), as well as CD56, an NK marker. They are almost always EBV positive by immunostaining or in situ hybridization. They are also positive for cytotoxic T cell markers TIA, granzyme and occasionally perforin. However, they are negative for CD16 and CD57 and there is usually no T cell receptor gene rearrangement.
The differential diagnosis includes diffuse large B cell lymphoma (the infiltrating T cells may obscure the neoplastic B cells) and florid herpes simplex virus of the nasopharynx (CD56+, HSV+, no angioinvasion or angiodestruction, EBV-, polyclonal) (Am J Surg Pathol 1999;23:1356, Mod Pathol 2003;16:166).
Treatment includes radiation therapy and chemotherapy but the overall 5 year survival is only ~50% (Cancer 2006;106:609).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California (USA).
ARUP Laboratories’ Surgical Pathology Workshop is scheduled for January 27 to February 1, 2008 at the Shadow Ridge Resort Hotel in Park City, Utah.
This five-day course is designed to address the activities and issues faced by the surgical pathologist – featuring short lectures and case-oriented discussions led by distinguished faculty from the University of Utah and ARUP Laboratories.
University of Utah School of Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing medical education for physicians.
Website news:
(1) We continue to add new books to our Books pages. Visit here.
Visit and follow our Blog to see recent updates to the website.
(1) We continue to add new books to our Books pages. Visit here.
Visit and follow our Blog to see recent updates to the website.
Case #101
Clinical history:
A 40 year woman with nasal sinus congestion had a CT scan, which showed a mass. Endoscopy showed friable nasal tissue. A biopsy was obtained.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: NK / T cell lymphoma, nasal type
Immunostains:
Keratin
CD20
CD3
CD56
EBV (by ISH)
TIA
Discussion:
The low power images show large areas of necrosis. Higher power images show an angiocentric pattern of pleomorphic tumor cells with hyperchromatic nuclei and occasional perinuclear clearing. There is prominent angiodestruction, although the vessel walls lack neutrophils or fibrinoid necrosis.
The tumor cells are negative for a cytokeratin cocktail, although some residual epithelial cells / vessels are positive. Most tumor cells are immunoreactive for the T cell marker CD3 (cytoplasmic staining) but negative for the B cell marker CD20. There is strong staining for the NK marker CD56, Epstein-Barr virus (by in situ hybridization) and TIA, a marker of activated cytotoxic T cells.
NK / T cell lymphomas (nasal type) were previously called angiocentric lymphoma or polymorphic reticulosis. They commonly present as a destructive nasal or midline facial tumor. In the U.S. they are rare and usually affect patients of Asian or Hispanic descent (Am J Surg Pathol 2000;24:1511). Outside the U.S., they are more common in Asia, Central and South America (Ai Zheng 2007;26:1170, Hum Path 2004;35:86, Appl Immunohistochem Mol Morphol 2007;15:38). Non-nasal NK / T cell lymphomas are similar and often present in the GI tract, skin and testis.
The tumor cells are positive for T cell markers CD2 and CD3 (cytoplasmic but not nuclear staining), as well as CD56, an NK marker. They are almost always EBV positive by immunostaining or in situ hybridization. They are also positive for cytotoxic T cell markers TIA, granzyme and occasionally perforin. However, they are negative for CD16 and CD57 and there is usually no T cell receptor gene rearrangement.
The differential diagnosis includes diffuse large B cell lymphoma (the infiltrating T cells may obscure the neoplastic B cells) and florid herpes simplex virus of the nasopharynx (CD56+, HSV+, no angioinvasion or angiodestruction, EBV-, polyclonal) (Am J Surg Pathol 1999;23:1356, Mod Pathol 2003;16:166).
Treatment includes radiation therapy and chemotherapy but the overall 5 year survival is only ~50% (Cancer 2006;106:609).