
8 November 2007 - Case #100
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Lisa A. Cerilli, University of New Mexico Health Sciences, Albuquerque, New Mexico (USA).

ARUP Laboratories’ Surgical Pathology Workshop is scheduled for January 27 to February 1, 2008 at the Shadow Ridge Resort Hotel in Park City, Utah.
This five-day course is designed to address the activities and issues faced by the surgical pathologist – featuring short lectures and case-oriented discussions led by distinguished faculty from the University of Utah and ARUP Laboratories.
University of Utah School of Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing medical education for physicians.
Advertisement
Case #100
Clinical history:
A 50 year old man had bilateral enlarging neck masses for 10 months. A core needle biopsy and cytology specimens were obtained.
Microscopic images:
What is your diagnosis?
Diagnosis: Nasopharyngeal carcinoma; favor undifferentiated subtype (metastatic)
Immunostains:
Discussion:
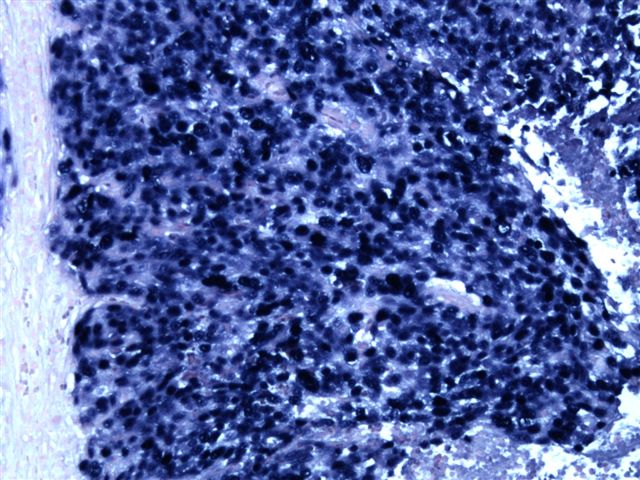
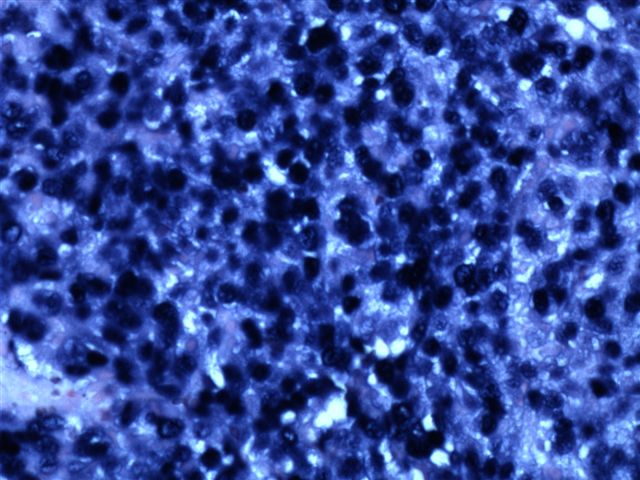
EBER stains were strongly immunoreactive.
Nasopharyngeal carcinoma is rare in the U.S. (incidence of 0.4 per 100,000 in whites) but it is endemic in South China (21.4 per 100K in Hong Kong) and parts of Africa. It is strongly associated with Epstein-Barr virus infection. Other risk factors include consumption of salt preserved fish containing carcinogenic nitrosamines, family history, specific HLA class I genotypes, tobacco smoking, chronic respiratory tract conditions and low consumption of fresh fruits and vegetables (Cancer Epidemiol Biomarkers Prev 2006;15:1765). The patient in this case was a native of New Mexico; other risk factors are unknown.
Nasopharyngeal carcinoma is classified into 3 histologic subtypes: keratinizing squamous cell carcinoma (WHO type 1), nonkeratinizing differentiated (WHO type 2) and nonkeratinizing undifferentiated (WHO type 3).
The undifferentiated subtype is composed of a syncytial arrangement of relatively uniform cells with indistinct cell margins. The cells have vesicular nuclei and prominent nucleoli. The tumor cells may be spindled. There is usually an inflammatory infiltrate of lymphocytes (often T cells), plasma cells, eosinophils and macrophages. There is usually no necrosis. The Schmincke pattern exists when the infiltrate is extensive, causing isolation of tumor cells and resembling lymphoma. The Regaud pattern exists when tumor cells form well defined nests separated by inflammatory cells. Tumor cells are immunoreactive for keratins, including CK5/6 and EBER1 by in situ hybridization. Nonkeratinizing squamous cell carcinoma is more differentiated. Tumor cells have distinct cell borders, a pavement stone pattern, more abundant eosinophilic cytoplasm and hyperchromatic nuclei (Mod Pathol 2002;15:229).
The differential diagnosis includes sinonasal undifferentiated carcinoma (SNUC) and melanoma. SNUC arises only in the nasal cavity and paranasal sinuses. Tumor cells are hyperchromatic with coarse chromatin and individual cell necrosis and central necrosis of cell nests are common. Tumor cells are EBER1 negative (Am J Surg Pathol 2002;26:371). Melanoma usually has different clinical characteristics and immunostaining properties, although the histology may be similar.
Treatment of undifferentiated nasopharyngeal carcinoma consists of immunotherapy with interferon, chemotherapy and radiation therapy. The 5 year survival is 50 - 60%.
References: Orphanet J Rare Dis 2006;1:23
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Lisa A. Cerilli, University of New Mexico Health Sciences, Albuquerque, New Mexico (USA).
ARUP Laboratories’ Surgical Pathology Workshop is scheduled for January 27 to February 1, 2008 at the Shadow Ridge Resort Hotel in Park City, Utah.
This five-day course is designed to address the activities and issues faced by the surgical pathologist – featuring short lectures and case-oriented discussions led by distinguished faculty from the University of Utah and ARUP Laboratories.
University of Utah School of Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing medical education for physicians.
Case #100
Clinical history:
A 50 year old man had bilateral enlarging neck masses for 10 months. A core needle biopsy and cytology specimens were obtained.
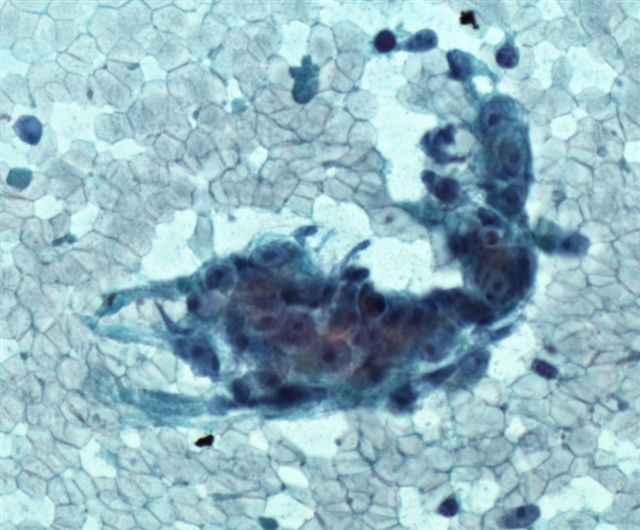
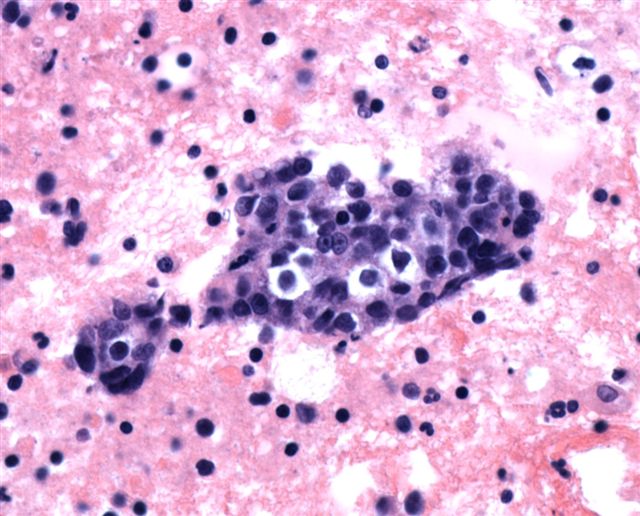
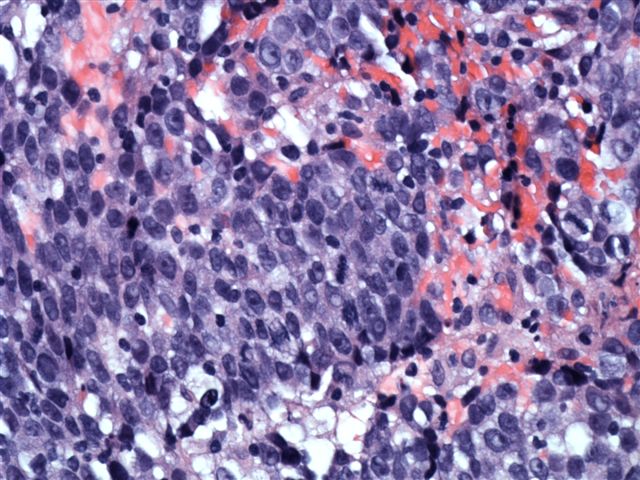
Microscopic images:
Pap stain
Cell block
Cell block
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Nasopharyngeal carcinoma; favor undifferentiated subtype (metastatic)
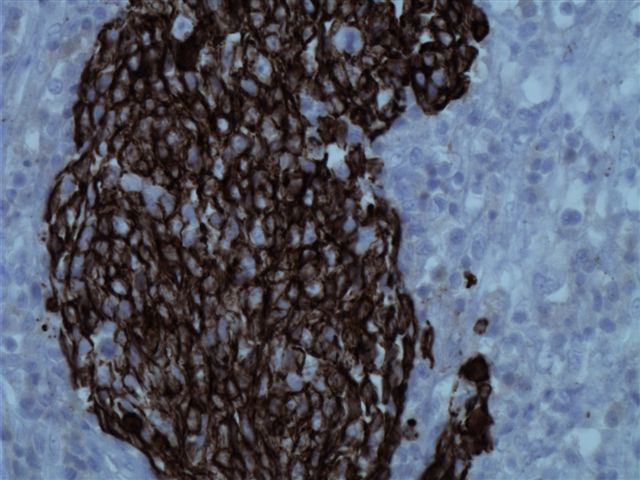
Immunostains:
CK5/6
EBER
Discussion:
EBER stains were strongly immunoreactive.
Nasopharyngeal carcinoma is rare in the U.S. (incidence of 0.4 per 100,000 in whites) but it is endemic in South China (21.4 per 100K in Hong Kong) and parts of Africa. It is strongly associated with Epstein-Barr virus infection. Other risk factors include consumption of salt preserved fish containing carcinogenic nitrosamines, family history, specific HLA class I genotypes, tobacco smoking, chronic respiratory tract conditions and low consumption of fresh fruits and vegetables (Cancer Epidemiol Biomarkers Prev 2006;15:1765). The patient in this case was a native of New Mexico; other risk factors are unknown.
Nasopharyngeal carcinoma is classified into 3 histologic subtypes: keratinizing squamous cell carcinoma (WHO type 1), nonkeratinizing differentiated (WHO type 2) and nonkeratinizing undifferentiated (WHO type 3).
The undifferentiated subtype is composed of a syncytial arrangement of relatively uniform cells with indistinct cell margins. The cells have vesicular nuclei and prominent nucleoli. The tumor cells may be spindled. There is usually an inflammatory infiltrate of lymphocytes (often T cells), plasma cells, eosinophils and macrophages. There is usually no necrosis. The Schmincke pattern exists when the infiltrate is extensive, causing isolation of tumor cells and resembling lymphoma. The Regaud pattern exists when tumor cells form well defined nests separated by inflammatory cells. Tumor cells are immunoreactive for keratins, including CK5/6 and EBER1 by in situ hybridization. Nonkeratinizing squamous cell carcinoma is more differentiated. Tumor cells have distinct cell borders, a pavement stone pattern, more abundant eosinophilic cytoplasm and hyperchromatic nuclei (Mod Pathol 2002;15:229).
The differential diagnosis includes sinonasal undifferentiated carcinoma (SNUC) and melanoma. SNUC arises only in the nasal cavity and paranasal sinuses. Tumor cells are hyperchromatic with coarse chromatin and individual cell necrosis and central necrosis of cell nests are common. Tumor cells are EBER1 negative (Am J Surg Pathol 2002;26:371). Melanoma usually has different clinical characteristics and immunostaining properties, although the histology may be similar.
Treatment of undifferentiated nasopharyngeal carcinoma consists of immunotherapy with interferon, chemotherapy and radiation therapy. The 5 year survival is 50 - 60%.
References: Orphanet J Rare Dis 2006;1:23
