11 October 2006 - Case of the Week #61
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
We thank Dr. Ankur Sangoi, Stanford University, California (USA) for contributing this case.
Case of the Week #61
Clinical history:
At a well child checkup, a 15 month old asymptomatic boy was noted to have a large, right upper quadrant abdominal mass. CT scan showed a large hepatic mass extending to the level of the iliac crest. Laboratory testing showed an elevated AFP at 1,398 and the clinical impression was hepatoblastoma.
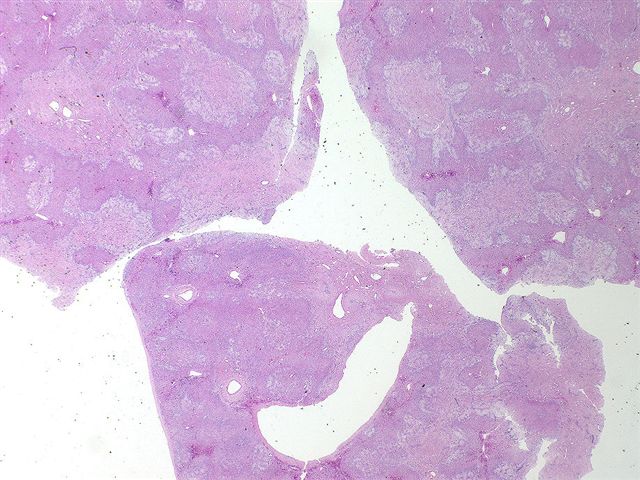
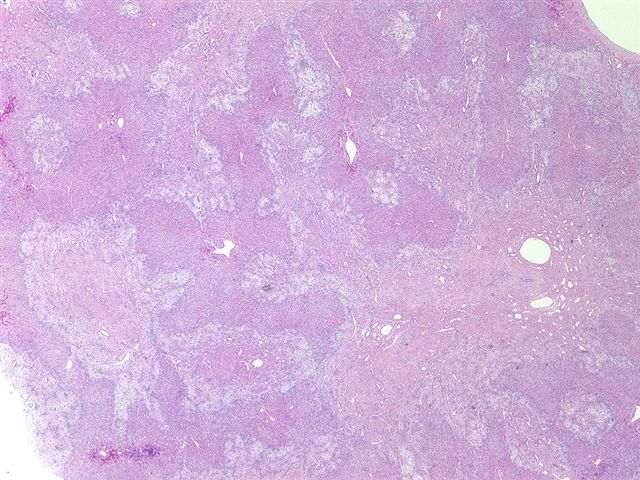
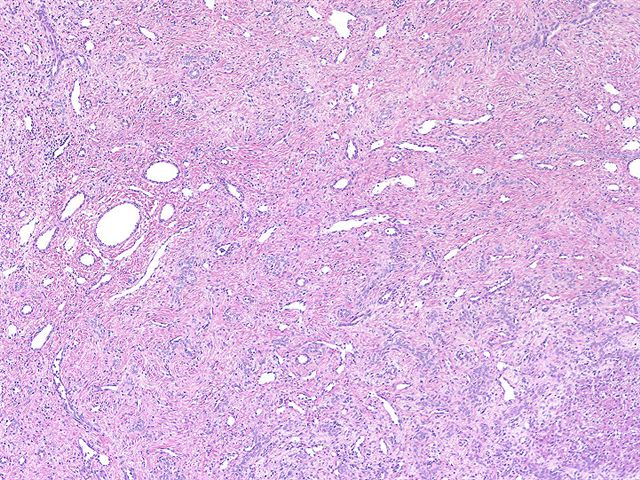
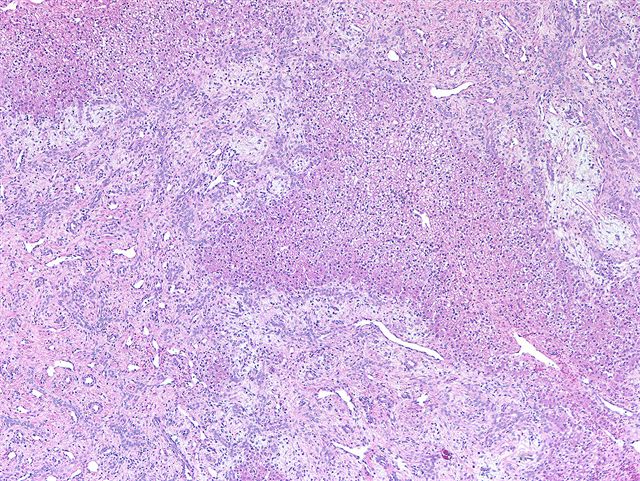
Microscopic images:
What is your diagnosis?
Diagnosis: Mesenchymal hamartoma
Discussion:
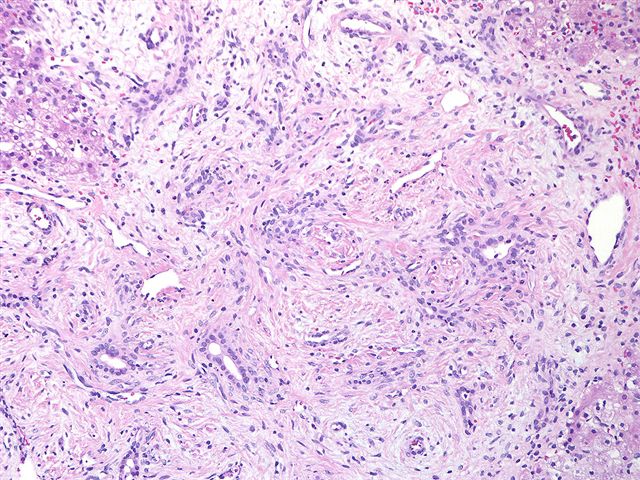
The images show branching bile ducts without atypia in a loose, myxoid stroma with myofibroblast-like cells, dilated vessels and lymphatics. At low power, it may resemble fibroadenoma. At high power, normal appearing hepatocytes are often present. There is usually extramedullary hematopoiesis, and the bile ducts may have a mesenchymal collar. No atypia or tumor giant cells are present.
Mesenchymal hamartoma was previously called cavernous cystic hamartoma, lymphangioadenomatoid tumor and benign mesenchymoma. It is typically an asymptomatic pediatric tumor, with 75% occurring before age one year and ~66% occurring in males. It comprises 8% of all pediatric liver tumors. The AFP is typically normal or minimally elevated, although occasionally it is markedly elevated.
These tumors range from 5 - 23 cm and are typically solitary and well circumscribed. They often have fluid filled cysts and become fibrotic with age. There is usually no necrosis, hemorrhage or calcification.
Mesenchymal hamartomas typically have benign behavior, although they rarely transform to embryonal sarcoma (Pediatr Dev Pathol 2001;4:482). Treatment consists of excision, which is curative but associated with high mortality, particularly with very large tumors.
In adults, the tumors are more fibrous and less myxoid, and extramedullary hematopoiesis is rare. Liver transplantation may be necessary (J Clin Pathol 2006;59:542).
These tumors are immunoreactive for CK7, vimentin, smooth muscle actin and desmin (Hum Path 2002;33:893). They are negative for CK20. Many cases have been associated with an interstitial deletion near 19q13.4 (Cancer Genet Cytogenet 2004;153:60).
The differential diagnosis includes bile duct adenoma (no hepatocyte islands), bile duct hamartoma (usually multiple with fibrous background), infantile hemangioendothelioma (more vascular) and embryonal sarcoma (marked cellularity and atypical cells).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
We thank Dr. Ankur Sangoi, Stanford University, California (USA) for contributing this case.
Case of the Week #61
Clinical history:
At a well child checkup, a 15 month old asymptomatic boy was noted to have a large, right upper quadrant abdominal mass. CT scan showed a large hepatic mass extending to the level of the iliac crest. Laboratory testing showed an elevated AFP at 1,398 and the clinical impression was hepatoblastoma.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Mesenchymal hamartoma
Discussion:
The images show branching bile ducts without atypia in a loose, myxoid stroma with myofibroblast-like cells, dilated vessels and lymphatics. At low power, it may resemble fibroadenoma. At high power, normal appearing hepatocytes are often present. There is usually extramedullary hematopoiesis, and the bile ducts may have a mesenchymal collar. No atypia or tumor giant cells are present.
Mesenchymal hamartoma was previously called cavernous cystic hamartoma, lymphangioadenomatoid tumor and benign mesenchymoma. It is typically an asymptomatic pediatric tumor, with 75% occurring before age one year and ~66% occurring in males. It comprises 8% of all pediatric liver tumors. The AFP is typically normal or minimally elevated, although occasionally it is markedly elevated.
These tumors range from 5 - 23 cm and are typically solitary and well circumscribed. They often have fluid filled cysts and become fibrotic with age. There is usually no necrosis, hemorrhage or calcification.
Mesenchymal hamartomas typically have benign behavior, although they rarely transform to embryonal sarcoma (Pediatr Dev Pathol 2001;4:482). Treatment consists of excision, which is curative but associated with high mortality, particularly with very large tumors.
In adults, the tumors are more fibrous and less myxoid, and extramedullary hematopoiesis is rare. Liver transplantation may be necessary (J Clin Pathol 2006;59:542).
These tumors are immunoreactive for CK7, vimentin, smooth muscle actin and desmin (Hum Path 2002;33:893). They are negative for CK20. Many cases have been associated with an interstitial deletion near 19q13.4 (Cancer Genet Cytogenet 2004;153:60).
The differential diagnosis includes bile duct adenoma (no hepatocyte islands), bile duct hamartoma (usually multiple with fibrous background), infantile hemangioendothelioma (more vascular) and embryonal sarcoma (marked cellularity and atypical cells).