
19 May 2005 - Case of the Week #7
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case is sponsored by our new advertiser Wavelength Consulting. Wavelength Consulting is Australia's premier medical recruitment firm. Their commitment to quality, integrity and confidentiality makes them the recruitment company of choice for international medical placements. They have a wealth of experience matching qualified doctors from around the world with positions throughout Australia and New Zealand. Their Australian based staff have the experience and relationships with hospitals and pathology practices, the Australasian College of Pathologists, immigration and registration boards to ensure that your transition is handled swiftly and smoothly. Visit their website www.wave.com.au to view a selection of jobs and to apply on-line or phone Chris Wallace on +61 2 9332 3368. Alternatively email chris@wave.com.au
This case was contributed by Dr. Peter Morawiecki, Great Lakes Naval Hospital, Great Lakes, Illinois (USA).
Case of the Week #7
Clinical history:
A 19 year old man had a few month history of a 0.5 cm subcutaneous, firm, grey lump on the right wrist. It was clinically suspected to be an epidermal cyst.
Microscopic images:

What is your diagnosis?
Diagnosis: Cellular blue nevus
Discussion:
Blue nevi appear to arise from the arrested migration of immature melanocytes in the dermis. They are uncommon, and are usually diagnosed in adults but may become apparent in early childhood or even at birth. Their blue color (clinically) is due to the Tyndall effect of selective absorption of parts of the light spectrum by deeply located (dermal) melanin pigment, which is usually abundant. There are several types of blue nevi, including common, cellular, atypical cellular, epithelioid and malignant.
The cellular blue nevus most commonly involves the buttock and sacrococcygeal areas but may also involve the scalp, face, hands and feet. It is considered benign but may rarely recur or involve regional lymph nodes. Unfortunately, no specific features to date have been identified to indicate whether cellular blue nevi will have aggressive behavior.
Cellular blue nevi are usually large (> 1.5 cm), with intense pigmentation. Microscopically, they consist of a well circumscribed collection of interweaving fascicles with increased cellularity and infiltration into the subcutaneous tissue. Heavily pigmented spindle and dendritic cells alternate with clear cells. The cells have finely eosinophilic or clear cytoplasm, with vesicular nuclei and small nucleoli. They may rarely be amelanotic. The margins are usually pushing. There is no / minimal atypia, no nuclear pleomorphism, no epidermal invasion, no peripheral inflammation, no necrosis and no / minimal mitotic figures. However, scalp lesions may exhibit intracranial extension.
Cellular blue nevi, as well as common blue nevi, are immunoreactive for melanocytic stains, such as S100, HMB45 and MelanA / MART1. Treatment consists of simple excision.
The differential diagnosis includes atypical cellular blue nevi, which exhibit either atypia insufficient for a diagnosis of malignancy or a mitotic rate of < 2 per square millimeter. They are also treated with conservative excision. The differential diagnosis may also include malignant blue nevi, which are very rare melanomas that are highly aggressive and may metastasize and cause death. They either have malignant cytology with a benign blue nevi component or appear benign at low power but have infiltrative borders, necrosis, mitotic figures or atypia at higher power.
References: Hum Path 2004;35:1292, AJSP 2002;26:1493, AJSP 2001;25:316
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case is sponsored by our new advertiser Wavelength Consulting. Wavelength Consulting is Australia's premier medical recruitment firm. Their commitment to quality, integrity and confidentiality makes them the recruitment company of choice for international medical placements. They have a wealth of experience matching qualified doctors from around the world with positions throughout Australia and New Zealand. Their Australian based staff have the experience and relationships with hospitals and pathology practices, the Australasian College of Pathologists, immigration and registration boards to ensure that your transition is handled swiftly and smoothly. Visit their website www.wave.com.au to view a selection of jobs and to apply on-line or phone Chris Wallace on +61 2 9332 3368. Alternatively email chris@wave.com.au
This case was contributed by Dr. Peter Morawiecki, Great Lakes Naval Hospital, Great Lakes, Illinois (USA).
Case of the Week #7
Clinical history:
A 19 year old man had a few month history of a 0.5 cm subcutaneous, firm, grey lump on the right wrist. It was clinically suspected to be an epidermal cyst.
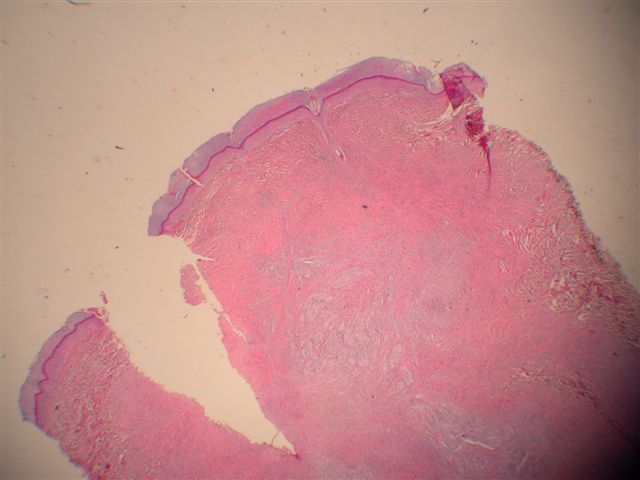
Microscopic images:
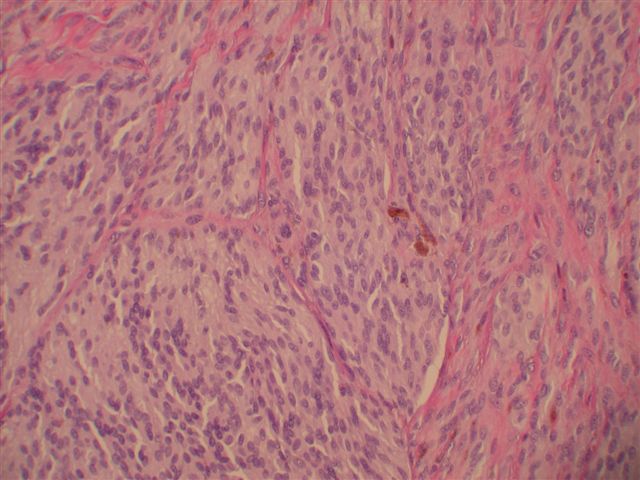
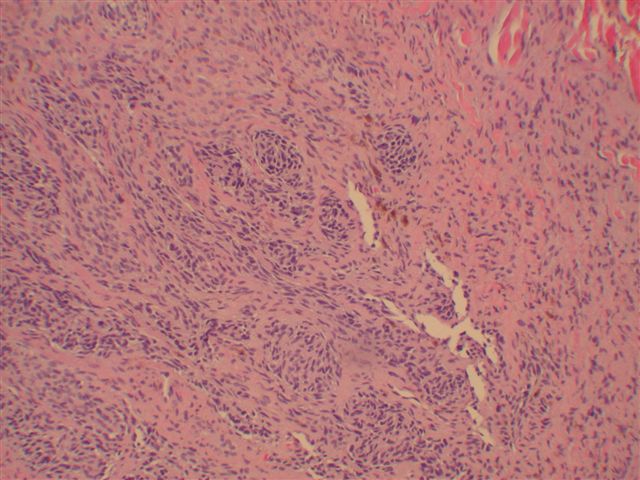
Low power
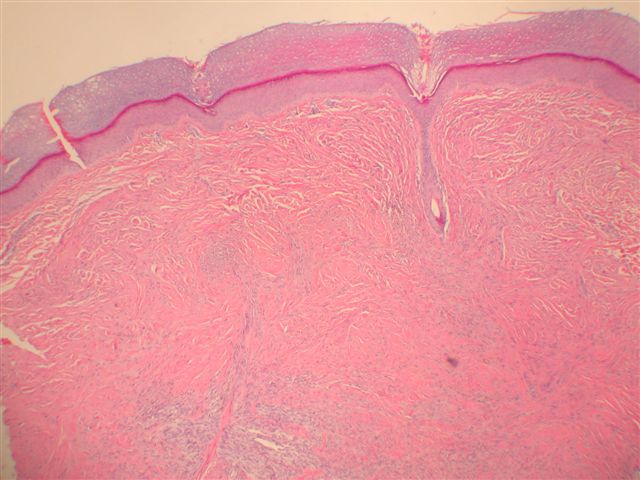
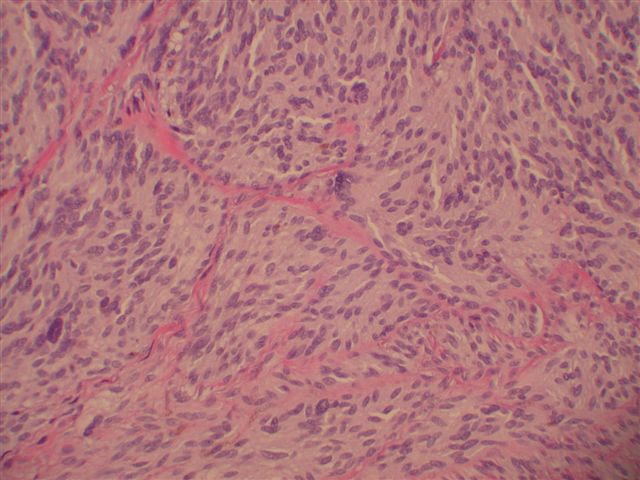
Medium power
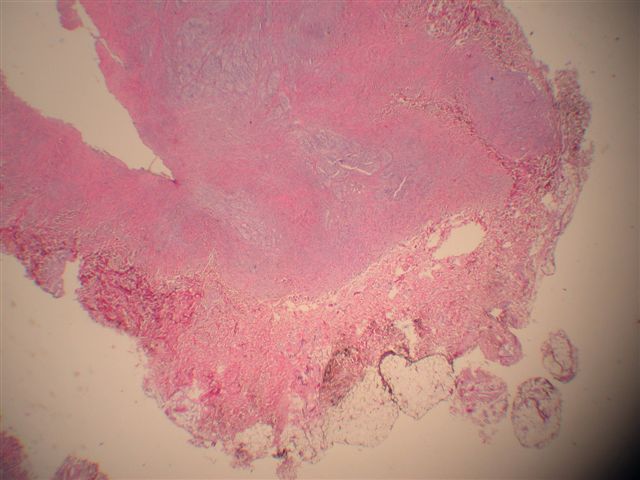
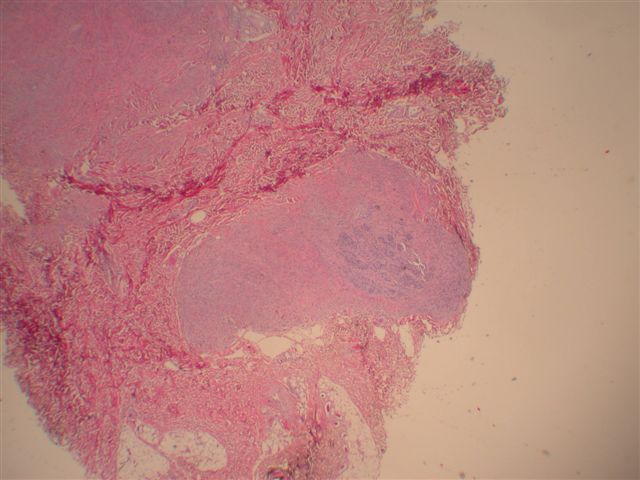
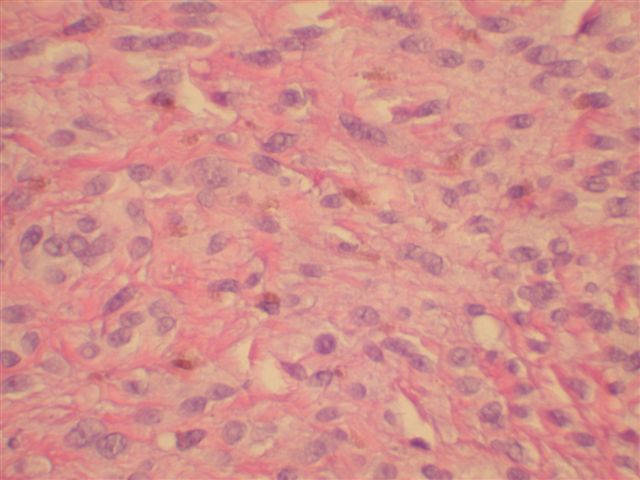
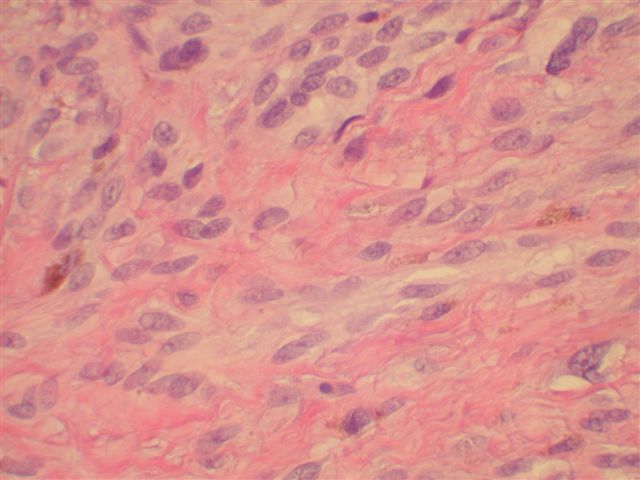
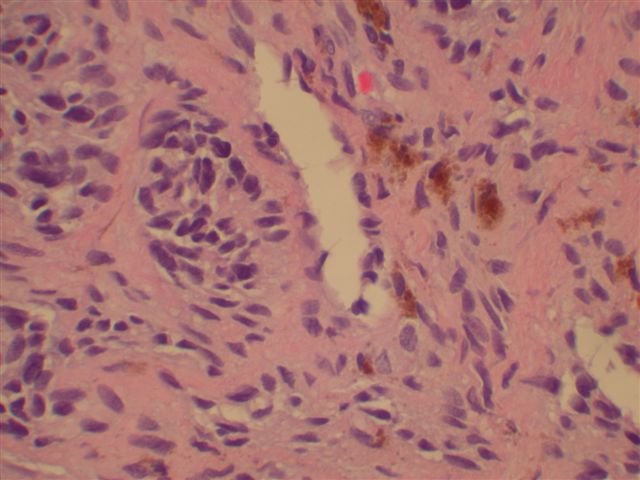
High power
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Cellular blue nevus
Discussion:
Blue nevi appear to arise from the arrested migration of immature melanocytes in the dermis. They are uncommon, and are usually diagnosed in adults but may become apparent in early childhood or even at birth. Their blue color (clinically) is due to the Tyndall effect of selective absorption of parts of the light spectrum by deeply located (dermal) melanin pigment, which is usually abundant. There are several types of blue nevi, including common, cellular, atypical cellular, epithelioid and malignant.
The cellular blue nevus most commonly involves the buttock and sacrococcygeal areas but may also involve the scalp, face, hands and feet. It is considered benign but may rarely recur or involve regional lymph nodes. Unfortunately, no specific features to date have been identified to indicate whether cellular blue nevi will have aggressive behavior.
Cellular blue nevi are usually large (> 1.5 cm), with intense pigmentation. Microscopically, they consist of a well circumscribed collection of interweaving fascicles with increased cellularity and infiltration into the subcutaneous tissue. Heavily pigmented spindle and dendritic cells alternate with clear cells. The cells have finely eosinophilic or clear cytoplasm, with vesicular nuclei and small nucleoli. They may rarely be amelanotic. The margins are usually pushing. There is no / minimal atypia, no nuclear pleomorphism, no epidermal invasion, no peripheral inflammation, no necrosis and no / minimal mitotic figures. However, scalp lesions may exhibit intracranial extension.
Cellular blue nevi, as well as common blue nevi, are immunoreactive for melanocytic stains, such as S100, HMB45 and MelanA / MART1. Treatment consists of simple excision.
The differential diagnosis includes atypical cellular blue nevi, which exhibit either atypia insufficient for a diagnosis of malignancy or a mitotic rate of < 2 per square millimeter. They are also treated with conservative excision. The differential diagnosis may also include malignant blue nevi, which are very rare melanomas that are highly aggressive and may metastasize and cause death. They either have malignant cytology with a benign blue nevi component or appear benign at low power but have infiltrative borders, necrosis, mitotic figures or atypia at higher power.
References: Hum Path 2004;35:1292, AJSP 2002;26:1493, AJSP 2001;25:316
