14 December 2005 - Case #31
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Professor D. Y. Cohen, Department of Pathology, Herzliyah Medical Center, Israel. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Case #31
Clinical history:
A 44 year old woman clinically had extensive tumor deposits on the omentum and serosal surfaces of the uterus, ovaries and fallopian tubes. A total abdominal hysterectomy, bilateral salpingo-oophorectomy was performed.
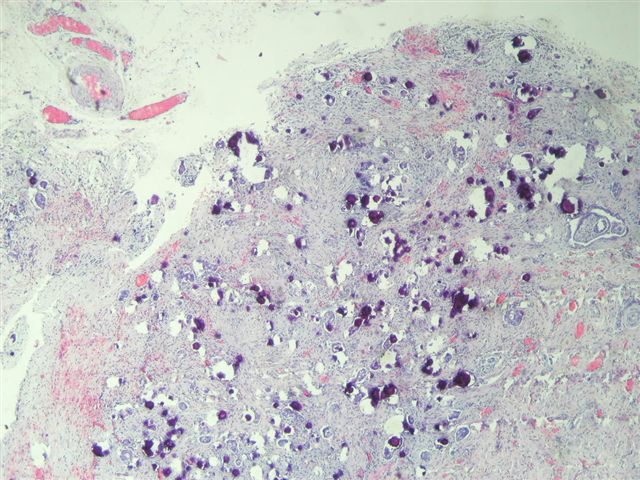
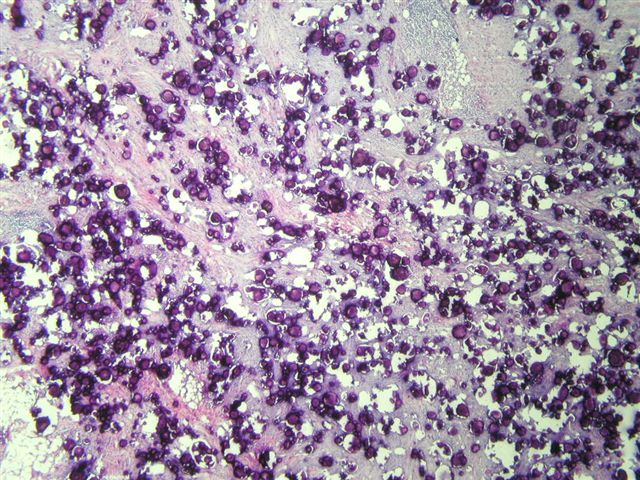
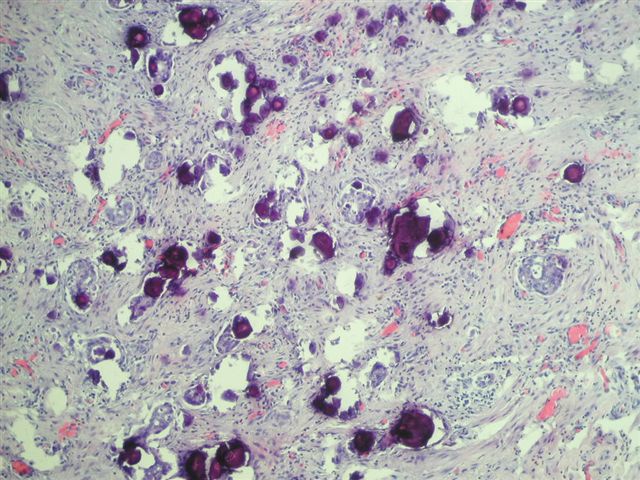
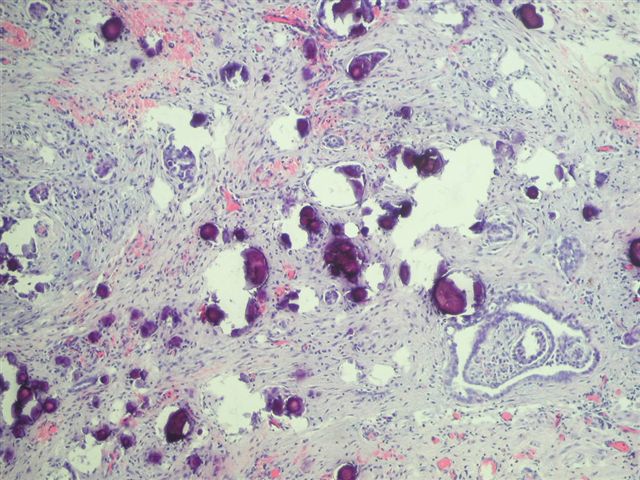
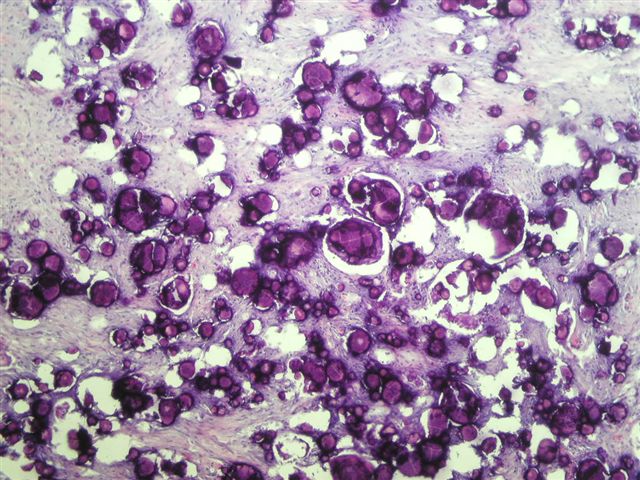
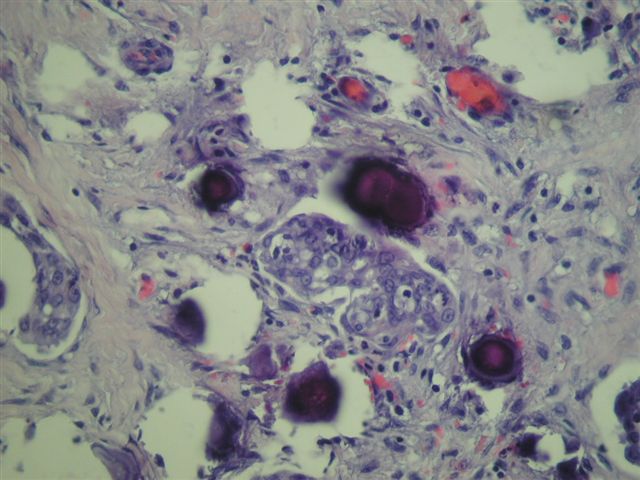
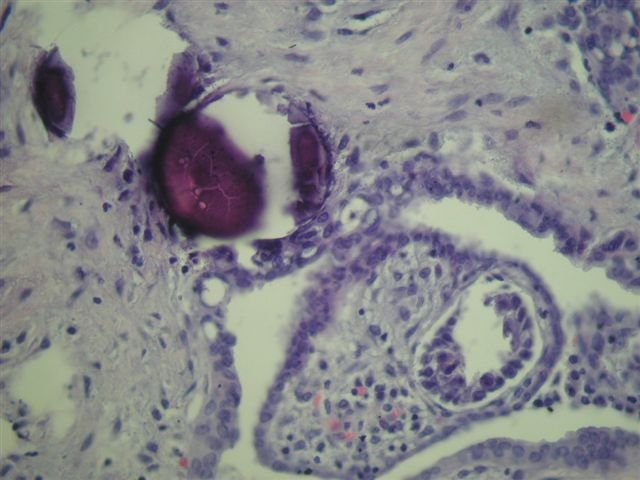
Microscopic images (low to high power):
What is your diagnosis?
Diagnosis: Serous psammocarcinoma
Discussion:
In all sites examined, the tumor was composed primarily of psammoma bodies with intervening areas of fibroblastic proliferation and small clusters of epithelial cells. Only mild to moderate atypia was present. Mitotic figures were absent or rare.
Psammocarcinoma, first reported in 1990 (Int J Gynecol Pathol 1990;9:110), is a rare variant of either peritoneal or ovarian serous carcinoma characterized by massive (75% or more) psammoma bodies. Cytologic features are low grade and mitotic figures are absent or rare. Extraovarian tumor implants may be present and the tumors are often stage III.
Treatment typically consists of maximal debulking with no chemotherapy or radiation therapy (Gynecol Oncol 1999;73:331). In young women, conservative surgery may be an option (Gynecol Oncol 1999;73:312).
The behavior of psammocarcinoma is indolent and more closely resembles serous borderline tumors than serous carcinomas. However, a case of aggressive disease with diffuse recurrence has been reported (Obstet Gynecol 1998;92:659).
Reference: Am J Surg Pathol 1998;22:849
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Professor D. Y. Cohen, Department of Pathology, Herzliyah Medical Center, Israel. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Case #31
Clinical history:
A 44 year old woman clinically had extensive tumor deposits on the omentum and serosal surfaces of the uterus, ovaries and fallopian tubes. A total abdominal hysterectomy, bilateral salpingo-oophorectomy was performed.
Microscopic images (low to high power):
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Serous psammocarcinoma
Discussion:
In all sites examined, the tumor was composed primarily of psammoma bodies with intervening areas of fibroblastic proliferation and small clusters of epithelial cells. Only mild to moderate atypia was present. Mitotic figures were absent or rare.
Psammocarcinoma, first reported in 1990 (Int J Gynecol Pathol 1990;9:110), is a rare variant of either peritoneal or ovarian serous carcinoma characterized by massive (75% or more) psammoma bodies. Cytologic features are low grade and mitotic figures are absent or rare. Extraovarian tumor implants may be present and the tumors are often stage III.
Treatment typically consists of maximal debulking with no chemotherapy or radiation therapy (Gynecol Oncol 1999;73:331). In young women, conservative surgery may be an option (Gynecol Oncol 1999;73:312).
The behavior of psammocarcinoma is indolent and more closely resembles serous borderline tumors than serous carcinomas. However, a case of aggressive disease with diffuse recurrence has been reported (Obstet Gynecol 1998;92:659).
Reference: Am J Surg Pathol 1998;22:849