5 January 2011 - Case #194
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Eddie Fridman, The Chaim Sheba Medical Center (Israel), for contributing this case.
Case #194
Clinical history:
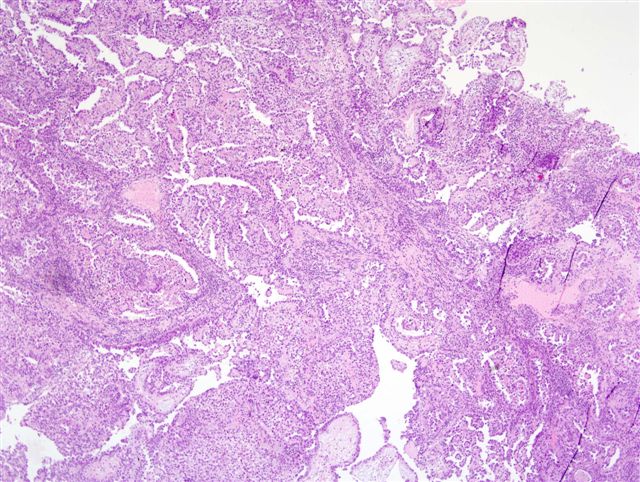
An 82 year old woman had a clinical diagnosis of space occupying lesion of the bladder neck and proximal urethra and underwent a transurethral resection.
Microscopic images:


What is your diagnosis?
Diagnosis: Clear cell adenocarcinoma of the proximal urethra
Discussion:
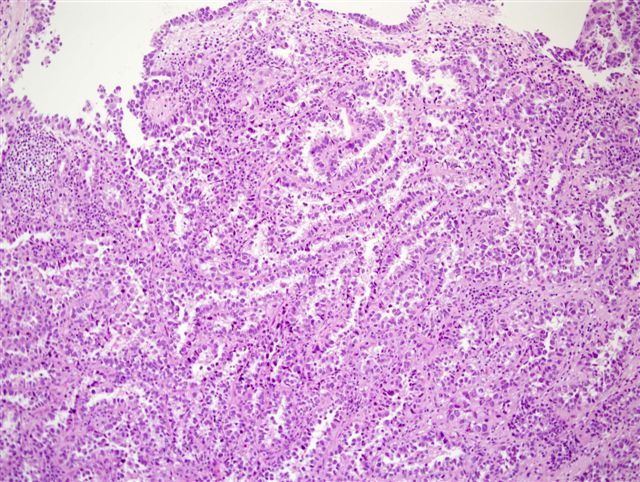
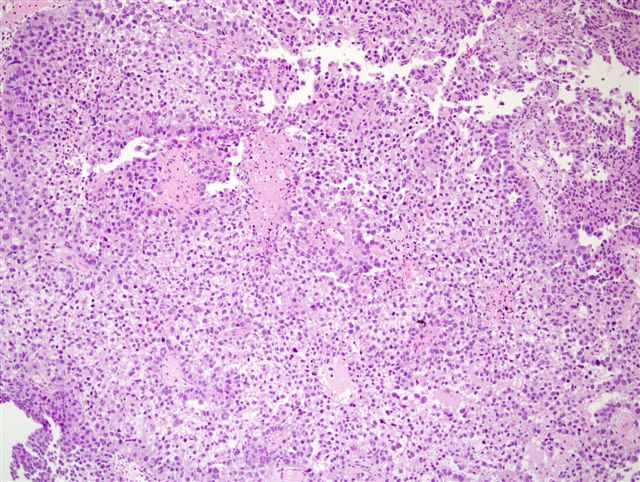
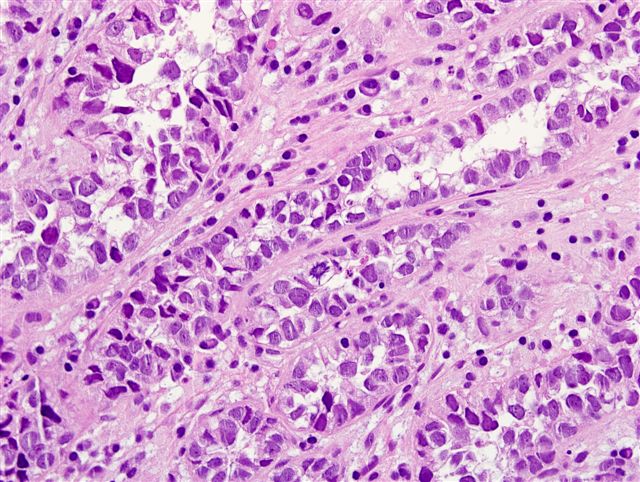
Clear cell adenocarcinoma of the urethra is a rare, high grade tumor that usually occurs in women. Grossly, the tumors are usually papillary. They have various architectural patterns, including tubules, cysts, papillae and diffuse tumor. Most tumors have prominent clear cells due to glycogen and hobnailing. Tumor cells have prominent pleomorphism and marked mitotic activity. There is often obvious muscular invasion and necrosis (Am J Surg Pathol 1985;9:816). Tumor cells are immunoreactive for CK7, CK903, Ki67 and p53, and usually negative for CK20. In contrast to most urothelial carcinomas, they are also immunoreactive for P504S and negative for p63 (Arch Pathol Lab Med 2008;132:1417).
The differential diagnosis includes nephrogenic adenoma, a metaplastic process often occurring in young adults with a history of GU trauma, surgery or stones. In nephrogenic adenoma, there may be reactive changes in the tumor cells and mitotic activity but there is no marked pleomorphism or invasion. There are usually no clear cells and if present, they are focal. Ki67 and p53 are usually negative or have minimal staining (Hum Pathol 1998;29:1451).
A recent report described clear cell adenocarcinomas that resemble nephrogenic adenoma due to less prominent nuclear pleomorphism, less prominent nucleoli and fewer clear cells (Hum Pathol 2010;41:594). However, this variant of clear cell adenocarcinoma did exhibit extensive muscular invasion and focal hyperchromatic and pleomorphic tumor cells that would not be present in nephrogenic adenoma.
Clear cell adenocarcinoma is an aggressive tumor, with low rates of 5 year survival (Clin Genitourin Cancer 2008;6:131). In this case, the patient received an incomplete course of chemotherapy after her surgery. She was well during the next 3 and a half years, until 5 months ago, when she underwent pelvic lymph node excision, revealing a few pelvic nodal metastases with a similar morphology as the primary tumor. She is currently without any new disease.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Eddie Fridman, The Chaim Sheba Medical Center (Israel), for contributing this case.
Website news:
(1) If you visit Amazon.com, click here, or on the Amazon banner on the left side of our Home Page, or on any links on our Books pages. By visiting Amazon via these links, Amazon sends us 5% of the cost of all items you purchase, at no additional charge to you.
(2) Thanks for your support. In 2010, we had 2,999,616 visits, or over 88 million hits.
Visit and follow our Blog to see recent updates to the website.
(1) If you visit Amazon.com, click here, or on the Amazon banner on the left side of our Home Page, or on any links on our Books pages. By visiting Amazon via these links, Amazon sends us 5% of the cost of all items you purchase, at no additional charge to you.
(2) Thanks for your support. In 2010, we had 2,999,616 visits, or over 88 million hits.
Visit and follow our Blog to see recent updates to the website.
Case #194
Clinical history:
An 82 year old woman had a clinical diagnosis of space occupying lesion of the bladder neck and proximal urethra and underwent a transurethral resection.
Microscopic images:
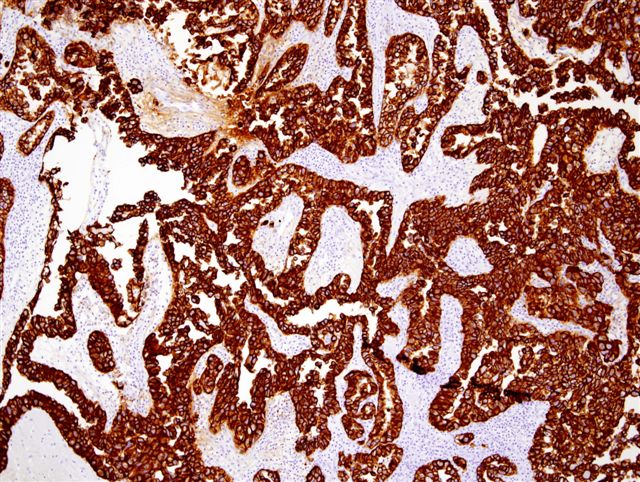
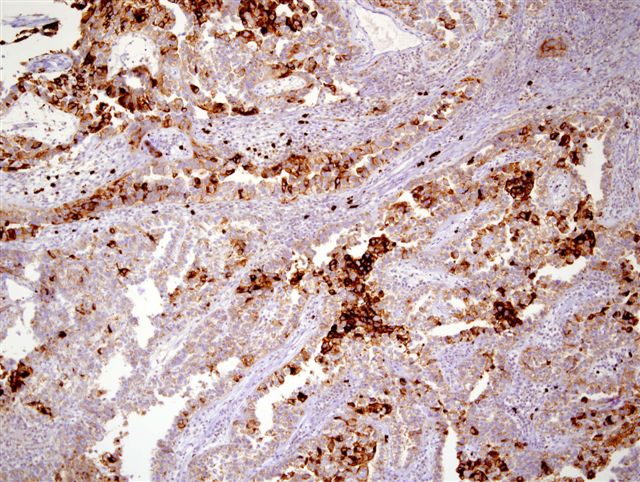
CK7 (left), CD15 (right)
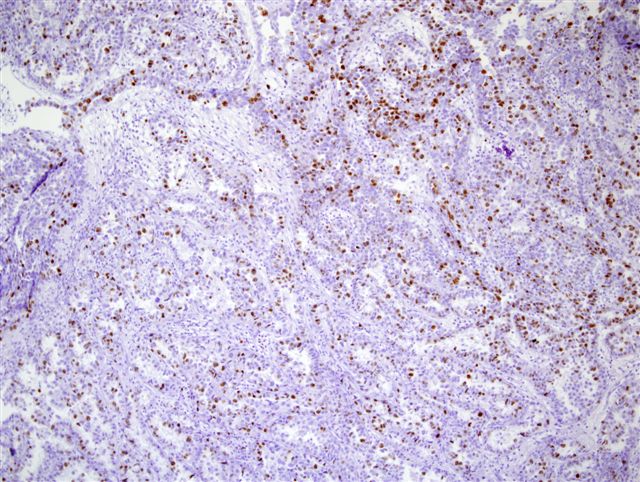
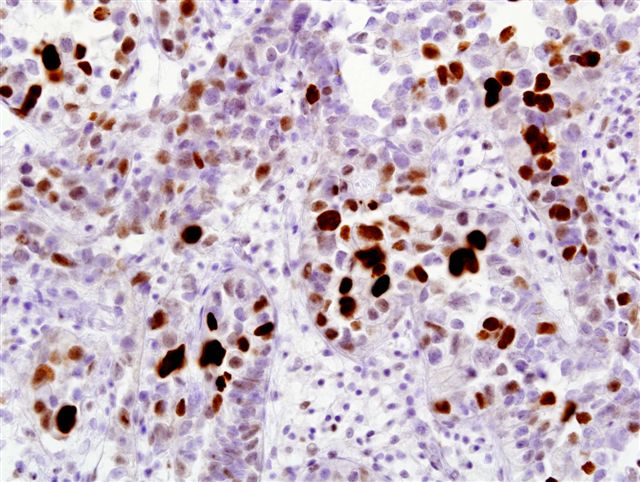
Ki67 staining
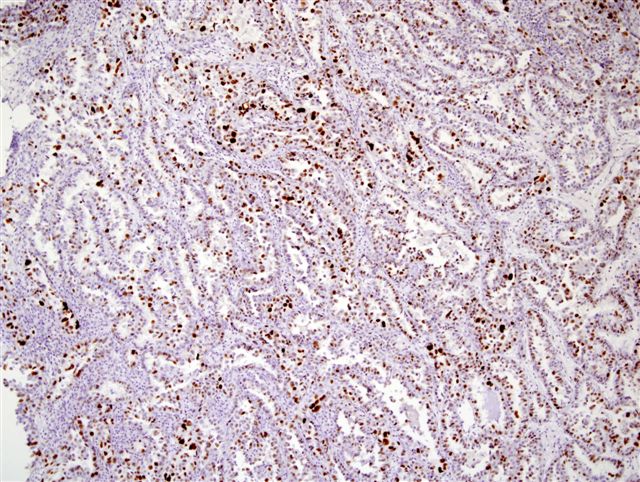
p53 staining
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Clear cell adenocarcinoma of the proximal urethra
Discussion:
Clear cell adenocarcinoma of the urethra is a rare, high grade tumor that usually occurs in women. Grossly, the tumors are usually papillary. They have various architectural patterns, including tubules, cysts, papillae and diffuse tumor. Most tumors have prominent clear cells due to glycogen and hobnailing. Tumor cells have prominent pleomorphism and marked mitotic activity. There is often obvious muscular invasion and necrosis (Am J Surg Pathol 1985;9:816). Tumor cells are immunoreactive for CK7, CK903, Ki67 and p53, and usually negative for CK20. In contrast to most urothelial carcinomas, they are also immunoreactive for P504S and negative for p63 (Arch Pathol Lab Med 2008;132:1417).
The differential diagnosis includes nephrogenic adenoma, a metaplastic process often occurring in young adults with a history of GU trauma, surgery or stones. In nephrogenic adenoma, there may be reactive changes in the tumor cells and mitotic activity but there is no marked pleomorphism or invasion. There are usually no clear cells and if present, they are focal. Ki67 and p53 are usually negative or have minimal staining (Hum Pathol 1998;29:1451).
A recent report described clear cell adenocarcinomas that resemble nephrogenic adenoma due to less prominent nuclear pleomorphism, less prominent nucleoli and fewer clear cells (Hum Pathol 2010;41:594). However, this variant of clear cell adenocarcinoma did exhibit extensive muscular invasion and focal hyperchromatic and pleomorphic tumor cells that would not be present in nephrogenic adenoma.
Clear cell adenocarcinoma is an aggressive tumor, with low rates of 5 year survival (Clin Genitourin Cancer 2008;6:131). In this case, the patient received an incomplete course of chemotherapy after her surgery. She was well during the next 3 and a half years, until 5 months ago, when she underwent pelvic lymph node excision, revealing a few pelvic nodal metastases with a similar morphology as the primary tumor. She is currently without any new disease.