28 January 2010 - Case #167
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Husain A. Saleh, Wayne State University, Detroit, Michigan (USA) for contributing this case and the discussion.



This 24.25 hour review and update in the areas of clinical chemistry, immunology, microbiology, and molecular medicine is intended to improve knowledge about the pathogenesis and clinical manifestations of a wide variety of metabolic, infectious, immunologic, and genetic disorders along with the selection, performance, and interpretation of clinical laboratory tests.
Course Directors: Harry R. Hill, MD, Elaine Lyon, PhD and William L. Roberts, MD, PhD
Special Guests: Robert Christenson, PhD, DABCC, FACB, Andrea Ferreira-Gonzalez, PhD and Steven M. Holland, MD
Advertisement
Case #167
Clinical history:
A 35 year old African American man presented with a large posterior neck / shoulder mass. CT scan of the neck and chest showed a 13 x 11 x 10 cm soft tissue mass of the right neck without calcifications. Previous surgery had been done in the vicinity. FNA of this mass was performed.
Microscopic images:



What is your diagnosis?
Diagnosis: Desmoid tumor (extraabdominal fibromatosis)
Discussion:
Extraabdominal fibromatosis or desmoid tumor is a rare, slow growing soft tissue neoplasm, usually occurring in young adults, that has been described in several organs and body sites. In up to 65% of cases, there is a history of surgery near the mass. In this case, the patient had 3 prior local surgical resections.
Clinically, the lesions are locally destructive and infiltrative; radiologic studies may give an impression of malignancy. Superficial fibromatosis involves the hands, feet and penis. Deep fibromatosis may involve the abdominal cavity or wall in young women but more commonly involves extraabdominal areas, especially limbs and girdles. They are generally rapidly growing and attain a larger size than superficial tumors. Occasionally, it presents in a familial context, as in Gardner syndrome, or in children (juvenile fibromatosis).
Histologically, early lesions show a cellular fibroblastic proliferation that decreases over time, with later tumors showing a predominance of collagen and more mature fibroblasts. Most tumors are centrally hypocellular surrounded by a peripheral, more cellular zone.
There are only limited reports of aspiration biopsy cytology for these tumors. The samples are often of low cellularity but may be moderately cellular depending on the age and proliferative phase of the lesion. They display a uniform appearance of fibroblastic / myofibroblastic spindle or polygonal bland tumor cells. There is moderate cytoplasm which is delicate, wispy and basophilic. The nuclei are elongated, bipolar or naked and uniformly bland with fine, evenly distributed chromatin and no distinct nucleoli. The tumor cells may be present as single, loose clusters or in small tissue fragments imparting a vague fascicular pattern. Fragments of dense collagenized stroma or matrix can also be seen.
In this case, the FNA biopsy was moderately cellular with syncytia in three dimensions and occasional loose clusters or singly dispersed cells. Cells were bland and spindled without mitosis, nuclear pleomorphism or atypia. A few fragments of collagenized or myxoid tissue were noted. The background appeared clean, without hemorrhage or tumor necrosis.
Desmoid tumor must be distinguished from other spindle cell tumors, particularly those with metastatic potential. In general, the differential diagnosis is broad and includes several fibroblastic / myofibroblastic lesions, such as nodular fasciitis, hypertrophic scar tissue, solitary fibrous tumor, leiomyoma / myofibroma, schwannoma and low grade fibrosarcoma. The latter is difficult to differentiate from desmoid tumor because both have bland cytologic features. However, low grade sarcomas display more cellularity, atypia and mitotic figures. Nodular fasciitis is usually more cellular, with a predominance of loose clusters (like tissue culture), single cells and myxoid tissue fragments, cellular atypia and an inflammatory background. Leiomyoma has blunted, not spindled bipolar cells. Schwannoma and neurofibroma typically have slender cells and wavy nuclei with pointed ends. Aspirates of stromal tissue repair are less cellular, with much more inflammation and reactive cellular atypia. An erroneous diagnosis on aspiration cytology is usually due to paucicellular specimens.
Immunostains may be helpful. Desmoid tumor cells display nuclear positivity for beta catenin, androgen receptor, estrogen receptor beta, cathepsin D and smooth muscle actin and are usually negative for CD34, c-kit, desmin, progesterone receptor and estrogen receptor alpha (Am J Surg Pathol 2005;29:653). In this case, the tumor cells were positive for beta catenin and negative for estrogen and progesterone receptors, CD117 / c-kit, CD34 and desmin, essentially in agreement with findings of other authors.
Due to the infiltrative pattern of desmoid tumors, surgical resection is commonly incomplete and recurrence rates can be as high as 30%. Conservative treatment is suggested, as the tumors often stop growing if they are not resected (Acta Orthop Scand 2003;74:455). Desmoid tumors do not metastasize.
Reference: Cancer 2007;111:166
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Husain A. Saleh, Wayne State University, Detroit, Michigan (USA) for contributing this case and the discussion.
This 24.25 hour review and update in the areas of clinical chemistry, immunology, microbiology, and molecular medicine is intended to improve knowledge about the pathogenesis and clinical manifestations of a wide variety of metabolic, infectious, immunologic, and genetic disorders along with the selection, performance, and interpretation of clinical laboratory tests.
Course Directors: Harry R. Hill, MD, Elaine Lyon, PhD and William L. Roberts, MD, PhD
Special Guests: Robert Christenson, PhD, DABCC, FACB, Andrea Ferreira-Gonzalez, PhD and Steven M. Holland, MD
Case #167
Clinical history:
A 35 year old African American man presented with a large posterior neck / shoulder mass. CT scan of the neck and chest showed a 13 x 11 x 10 cm soft tissue mass of the right neck without calcifications. Previous surgery had been done in the vicinity. FNA of this mass was performed.
Microscopic images:
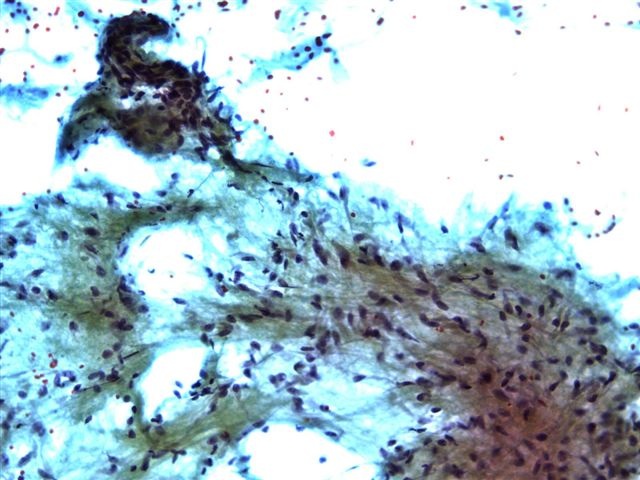
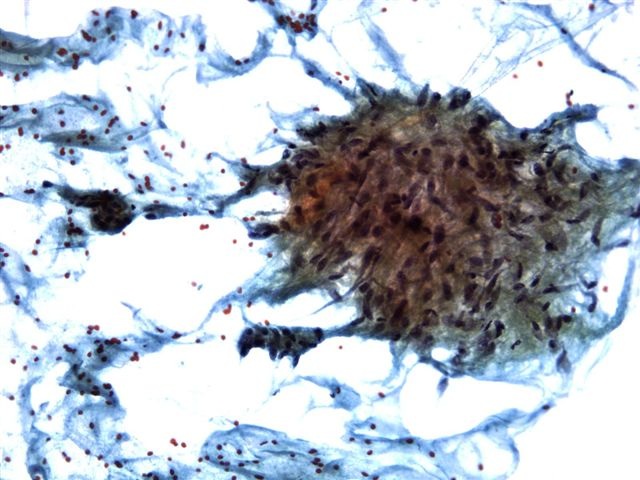
Diff-Quik stained smear
Pap stained smears
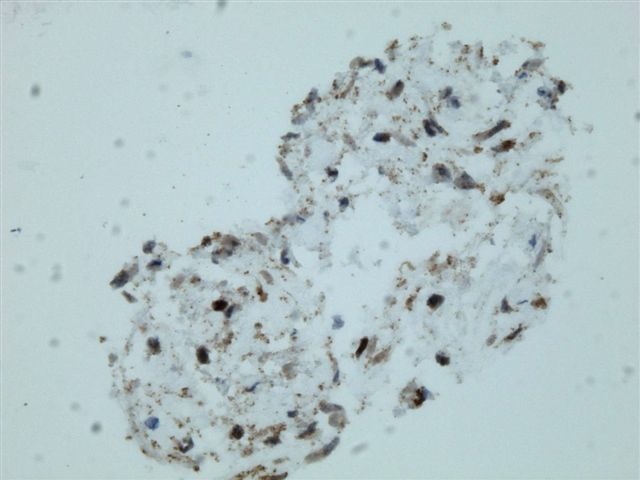
Beta catenin on cell block section
FNA biopsy
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Desmoid tumor (extraabdominal fibromatosis)
Discussion:
Extraabdominal fibromatosis or desmoid tumor is a rare, slow growing soft tissue neoplasm, usually occurring in young adults, that has been described in several organs and body sites. In up to 65% of cases, there is a history of surgery near the mass. In this case, the patient had 3 prior local surgical resections.
Clinically, the lesions are locally destructive and infiltrative; radiologic studies may give an impression of malignancy. Superficial fibromatosis involves the hands, feet and penis. Deep fibromatosis may involve the abdominal cavity or wall in young women but more commonly involves extraabdominal areas, especially limbs and girdles. They are generally rapidly growing and attain a larger size than superficial tumors. Occasionally, it presents in a familial context, as in Gardner syndrome, or in children (juvenile fibromatosis).
Histologically, early lesions show a cellular fibroblastic proliferation that decreases over time, with later tumors showing a predominance of collagen and more mature fibroblasts. Most tumors are centrally hypocellular surrounded by a peripheral, more cellular zone.
There are only limited reports of aspiration biopsy cytology for these tumors. The samples are often of low cellularity but may be moderately cellular depending on the age and proliferative phase of the lesion. They display a uniform appearance of fibroblastic / myofibroblastic spindle or polygonal bland tumor cells. There is moderate cytoplasm which is delicate, wispy and basophilic. The nuclei are elongated, bipolar or naked and uniformly bland with fine, evenly distributed chromatin and no distinct nucleoli. The tumor cells may be present as single, loose clusters or in small tissue fragments imparting a vague fascicular pattern. Fragments of dense collagenized stroma or matrix can also be seen.
In this case, the FNA biopsy was moderately cellular with syncytia in three dimensions and occasional loose clusters or singly dispersed cells. Cells were bland and spindled without mitosis, nuclear pleomorphism or atypia. A few fragments of collagenized or myxoid tissue were noted. The background appeared clean, without hemorrhage or tumor necrosis.
Desmoid tumor must be distinguished from other spindle cell tumors, particularly those with metastatic potential. In general, the differential diagnosis is broad and includes several fibroblastic / myofibroblastic lesions, such as nodular fasciitis, hypertrophic scar tissue, solitary fibrous tumor, leiomyoma / myofibroma, schwannoma and low grade fibrosarcoma. The latter is difficult to differentiate from desmoid tumor because both have bland cytologic features. However, low grade sarcomas display more cellularity, atypia and mitotic figures. Nodular fasciitis is usually more cellular, with a predominance of loose clusters (like tissue culture), single cells and myxoid tissue fragments, cellular atypia and an inflammatory background. Leiomyoma has blunted, not spindled bipolar cells. Schwannoma and neurofibroma typically have slender cells and wavy nuclei with pointed ends. Aspirates of stromal tissue repair are less cellular, with much more inflammation and reactive cellular atypia. An erroneous diagnosis on aspiration cytology is usually due to paucicellular specimens.
Immunostains may be helpful. Desmoid tumor cells display nuclear positivity for beta catenin, androgen receptor, estrogen receptor beta, cathepsin D and smooth muscle actin and are usually negative for CD34, c-kit, desmin, progesterone receptor and estrogen receptor alpha (Am J Surg Pathol 2005;29:653). In this case, the tumor cells were positive for beta catenin and negative for estrogen and progesterone receptors, CD117 / c-kit, CD34 and desmin, essentially in agreement with findings of other authors.
Due to the infiltrative pattern of desmoid tumors, surgical resection is commonly incomplete and recurrence rates can be as high as 30%. Conservative treatment is suggested, as the tumors often stop growing if they are not resected (Acta Orthop Scand 2003;74:455). Desmoid tumors do not metastasize.
Reference: Cancer 2007;111:166