19 November 2009 - Case #162
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Atif Ahmed, Children's Mercy Hospitals and Clinics, Kansas, MO (USA), for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Case #162
Clinical history:
A 9 month old girl was admitted for repair of an imperforate anus. Distal sacral agenesis was identified on Xray. Imaging studies also revealed a partly cystic, partly solid mass in the presacral area.
Microscopic images:

What is your diagnosis?
Diagnosis: Currarino syndrome, with components of mature cystic teratoma and ependymoma (anaplastic, WHO grade III)
Discussion:
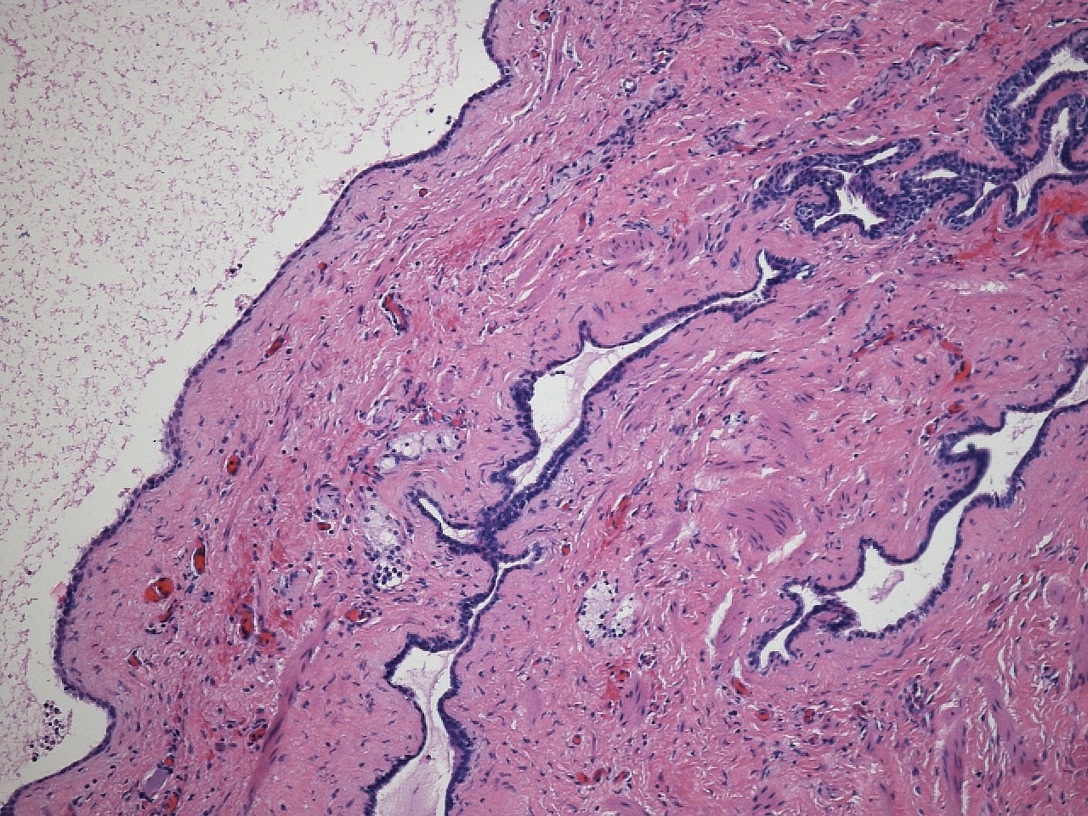
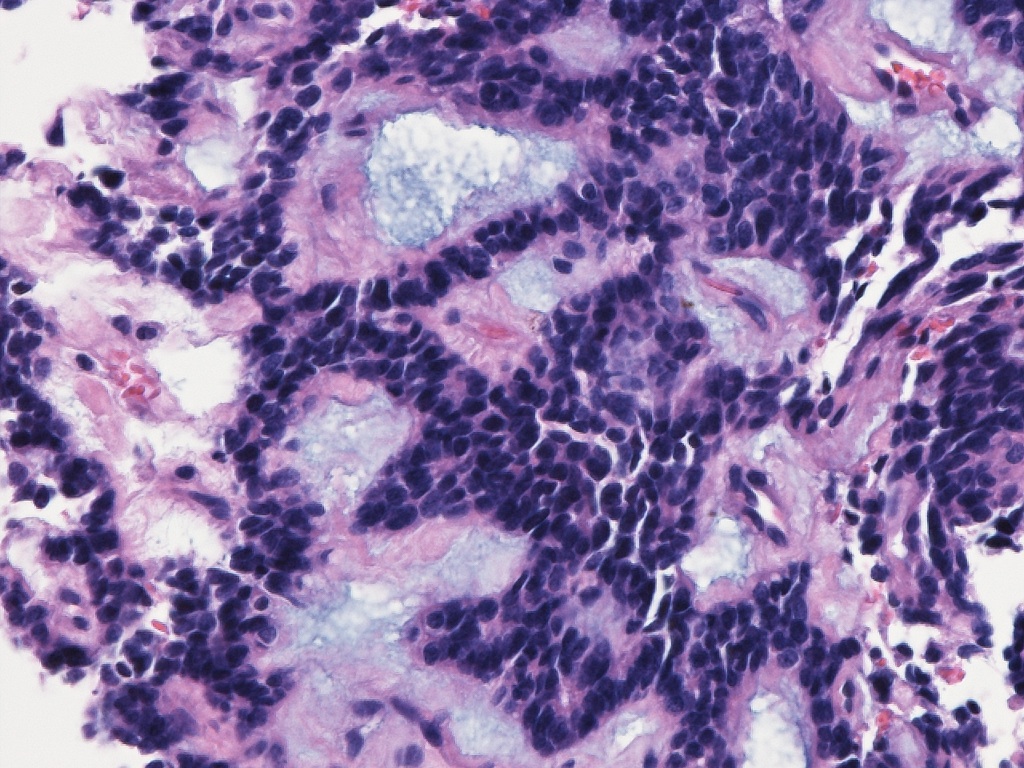
The cystic areas were grossly and microscopically identified as mature cystic teratoma, composed of fibrous tissue, adipose tissue and glandular cystic elements including a dermoid cyst (figure 1). In addition, a neuronal tumor is present (figures 2 and 3) characterized by papillary formations, tumor cells arranged around islands of mucin, and other histologic features suggestive of myxopapillary ependymoma. The tumor cells stained diffusely with GFAP and vimentin. Further analysis revealed hypercellularity, increased mitotic rate and high MIB1 proliferation rate (> 50%), leading to reclassification of the tumor to anaplastic ependymoma (WHO grade III).
Currarino syndrome is a triad of (a) partial sacral agenesis with intact first sacral vertebra, (b) anorectal malformations and (c) a presacral mass (J Med Genet 2000;37:561). It is an autosomal dominant syndrome associated with mutations in the MNX1 (HLXB9) gene (J Pediatr Surg 2009;44:1892). Patients with the same mutation may have variable phenotypic expression (J Hum Genet 2007;52:698). Presacral tumors reported with this syndrome include anterior myelomeningocele, teratoma, hamartoma, dermoid cyst, neuroenteric cyst or a combination (Am J Med Genet 2004;128:299).
Teratoma and myelomeningocele are the most frequent presacral components. Teratomas may undergo malignant degeneration into peripheral primitive neuroectodermal tumor (Pediatr Blood Cancer 2008;50:172). The present case represents the first reported occurrence of ependymoma and teratoma in a patient with Currarino syndrome.
References: Neurosurgery 2006;58:924, Childs Nerv Syst 2000;16:522, Pediatrics 2002;109:961
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Atif Ahmed, Children's Mercy Hospitals and Clinics, Kansas, MO (USA), for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Website news:
(1) Thanks to Dr. Suhail Muzaffar, City Hospital, West Midlands, UK, for contributing images of normal duodenum for our Small Bowel chapter and Dr. Guido Nicol, Genova, Italy, for submitting images of Enterobius vermicularis eggs for the Cervix-Cytology chapter.
(2) We have hired another medical editor, and anticipate updating chapters more frequently. We are currently updating Bladder, Breast-nonmalignant, Chemistry-Adrenal and Cardiac, Coagulation, Penis/Scrotum, Soft Tissue Part 3 and Uterus.
Visit and follow our Blog to see recent updates to the website.
(1) Thanks to Dr. Suhail Muzaffar, City Hospital, West Midlands, UK, for contributing images of normal duodenum for our Small Bowel chapter and Dr. Guido Nicol, Genova, Italy, for submitting images of Enterobius vermicularis eggs for the Cervix-Cytology chapter.
(2) We have hired another medical editor, and anticipate updating chapters more frequently. We are currently updating Bladder, Breast-nonmalignant, Chemistry-Adrenal and Cardiac, Coagulation, Penis/Scrotum, Soft Tissue Part 3 and Uterus.
Visit and follow our Blog to see recent updates to the website.
Case #162
Clinical history:
A 9 month old girl was admitted for repair of an imperforate anus. Distal sacral agenesis was identified on Xray. Imaging studies also revealed a partly cystic, partly solid mass in the presacral area.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Currarino syndrome, with components of mature cystic teratoma and ependymoma (anaplastic, WHO grade III)
Discussion:
The cystic areas were grossly and microscopically identified as mature cystic teratoma, composed of fibrous tissue, adipose tissue and glandular cystic elements including a dermoid cyst (figure 1). In addition, a neuronal tumor is present (figures 2 and 3) characterized by papillary formations, tumor cells arranged around islands of mucin, and other histologic features suggestive of myxopapillary ependymoma. The tumor cells stained diffusely with GFAP and vimentin. Further analysis revealed hypercellularity, increased mitotic rate and high MIB1 proliferation rate (> 50%), leading to reclassification of the tumor to anaplastic ependymoma (WHO grade III).
Currarino syndrome is a triad of (a) partial sacral agenesis with intact first sacral vertebra, (b) anorectal malformations and (c) a presacral mass (J Med Genet 2000;37:561). It is an autosomal dominant syndrome associated with mutations in the MNX1 (HLXB9) gene (J Pediatr Surg 2009;44:1892). Patients with the same mutation may have variable phenotypic expression (J Hum Genet 2007;52:698). Presacral tumors reported with this syndrome include anterior myelomeningocele, teratoma, hamartoma, dermoid cyst, neuroenteric cyst or a combination (Am J Med Genet 2004;128:299).
Teratoma and myelomeningocele are the most frequent presacral components. Teratomas may undergo malignant degeneration into peripheral primitive neuroectodermal tumor (Pediatr Blood Cancer 2008;50:172). The present case represents the first reported occurrence of ependymoma and teratoma in a patient with Currarino syndrome.
References: Neurosurgery 2006;58:924, Childs Nerv Syst 2000;16:522, Pediatrics 2002;109:961