17 July 2009 - Case #152
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Siobhan O'Connor and Dr. Mamatha Chivukula, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania (USA), for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Case #152
Clinical history:
A 54 year old woman presented with cough, vomiting and headache. Her medical history was significant for smoking cigarettes for 40 years. A urinary tract infection was suspected and she was treated with Ciprofloxacin but her symptoms did not improve.
An abdominopelvic ultrasound showed multiple leiomyomata and a normal right ovary. The left ovary was not visualized, but a large complex mass was seen in the left adnexa, 11.8 x 7.5 x 9.4 cm. A CT scan revealed a 1.4 cm nodule in the left lower lobe of the lung, multiple necrotic conglomerate lymph node masses within the mediastinum up to 3.7 cm, a 1.5 cm necrotic right pretracheal lymph node and the pelvic mass. Colonoscopy showed tubular and tubulovillous adenomas. Mammography was negative.
The patient underwent a total abdominal hysterectomy and bilateral salpingo-oophorectomy, appendectomy and pelvic biopsies.
Microscopic images:
What is your diagnosis?
Diagnosis: Pulmonary adenocarcinoma metastatic to ovary
Immunostains:
Discussion:
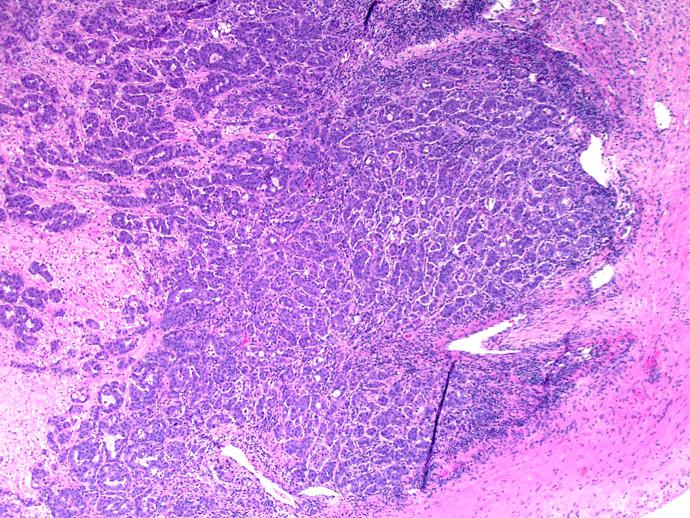
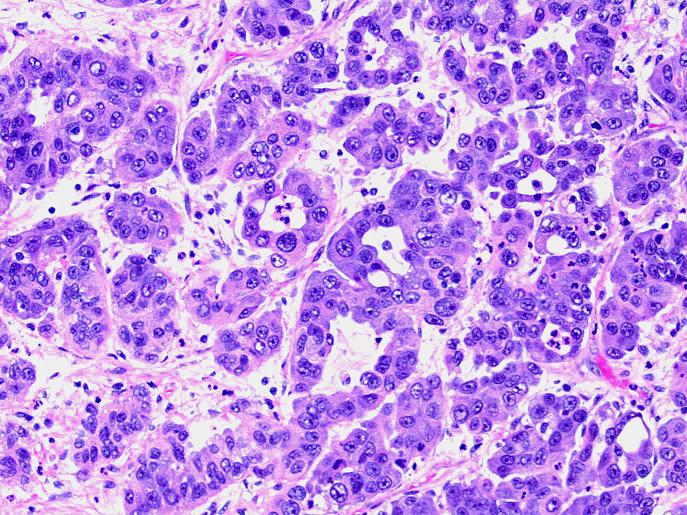
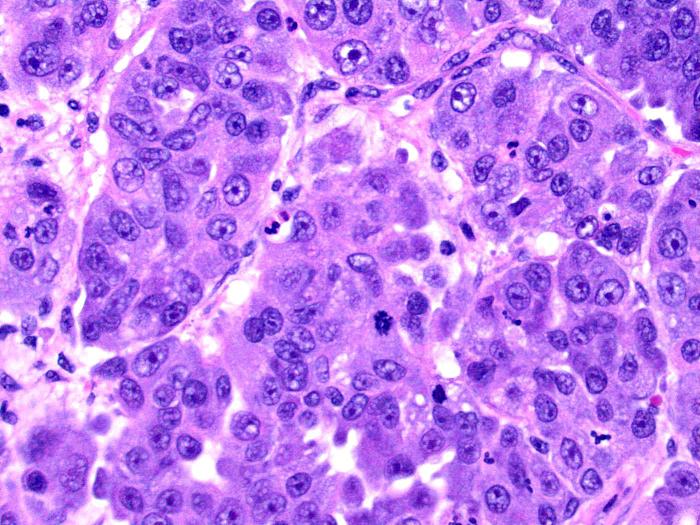
The tumor consists of cells arranged in nests and in some areas, forming glandular structures. The cells show high grade morphology with pleomorphism and prominent nucleoli.
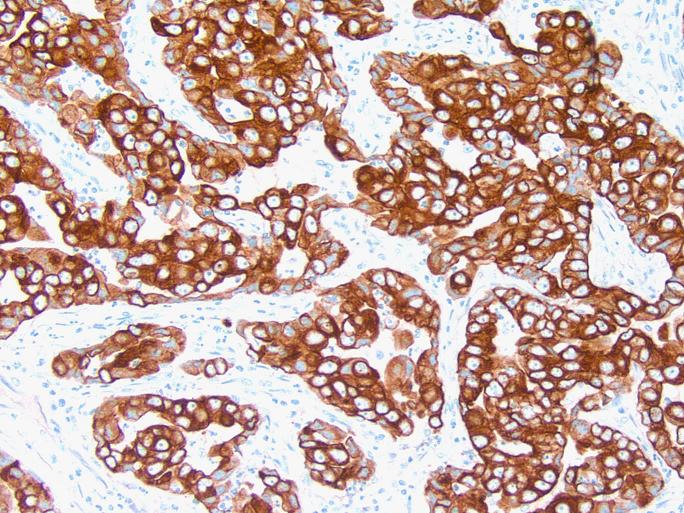
CK7 showed strong, diffusely staining. CEA and ER (not shown) were focally positive, though ER was weak. TTF1 showed moderately strong, diffusely positive staining. p16 (not shown) also showed positive staining. CK20, mammaglobin, GCDFP, CDX2, villin, WT1, CD10 and vimentin all showed negative staining.
Based on histology, the tumor is a high grade adenocarcinoma and the staining pattern suggests lung origin.
While metastases to the ovary are common, metastasis of pulmonary adenocarcinoma to ovary is rare. In one study of 325 metastases to the female genital tract, only one lung primary was identified (Cancer 1984;53:1978). The metastasis was the first evidence of disease in only 21 cases. In autopsy series, pulmonary metastases to ovary may account for up to 2 - 5% of ovarian metastases (Gyn Oncol 1985;21:337). For diagnostic and treatment purposes, it is important to distinguish between primary ovarian cancer and metastases to the ovary. Metastatic papillary adenocarcinomas may be difficult to discriminate from ovarian primaries because of their resemblance to papillary serous adenocarcinoma of the ovary. When the adenocarcinoma is poorly differentiated, as in this case, the differential is broad, since it may include an ovarian primary as well as metastasis from any glandular organ.
Several case studies have demonstrated ovarian metastases from lung (Jpn J Clin Oncol 2003;33:404). In one study, the pulmonary origin was confirmed by immunohistochemical positivity for carcinoembryonic antigen, E-cadherin and surfactant in combination with negativity for CA125, N-cadherin and vimentin (Arch Pathol Lab Med 2002;126:1101). Another group demonstrated positive immunohistochemical staining for CK7 and TTF1 along with negativity for CK20, similar to the pattern in this case. Sensitivity and specificity of TTF1 for lung adenocarcinoma have been reported at 62% and 100%, respectively (Pathol Res Prac 2000;196:835). Another study documented the usefulness of TTF1, CK7, CK20 and PE-10 (Cancer 2001;93:330). When a poorly differentiated adenocarcinoma is located in the ovary, a large panel may be required to identify its origin and if the tumor is positive for CK7 and TTF1, while being negative for CK20, it is most likely a metastasis from lung but a mesonephric or mesonephric-like carcinoma must also be excluded (Pathology 2018;50:141).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Siobhan O'Connor and Dr. Mamatha Chivukula, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania (USA), for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Website news:
(1) We have posted the Skin-Melanocytic Tumors chapter in our new format. We have also posted these new / revised markers in the Stains chapter: HE4 (serum marker for ovarian carcinoma), Oscar Keratin (wide-spectrum keratin) and GCDFP-15 (marker of apocrine function). We are starting to update Soft Tissue Tumors 3 - Muscle, Vascular, Nerve, Other.
(2) Thanks to Dr. Angel Fernandez-Flores, Hospital El Bierzo and Clinica Ponferrada, Spain, for contributing images of folliculitis decalvans for the Skin-nontumor chapter under Alopecia. Thanks to Jennifer Stumph, MD, Spectrum Health, for contributing images of schistosomiasis to the Parasitology chapter.
Visit and follow our Blog to see recent updates to the website.
(1) We have posted the Skin-Melanocytic Tumors chapter in our new format. We have also posted these new / revised markers in the Stains chapter: HE4 (serum marker for ovarian carcinoma), Oscar Keratin (wide-spectrum keratin) and GCDFP-15 (marker of apocrine function). We are starting to update Soft Tissue Tumors 3 - Muscle, Vascular, Nerve, Other.
(2) Thanks to Dr. Angel Fernandez-Flores, Hospital El Bierzo and Clinica Ponferrada, Spain, for contributing images of folliculitis decalvans for the Skin-nontumor chapter under Alopecia. Thanks to Jennifer Stumph, MD, Spectrum Health, for contributing images of schistosomiasis to the Parasitology chapter.
Visit and follow our Blog to see recent updates to the website.
Case #152
Clinical history:
A 54 year old woman presented with cough, vomiting and headache. Her medical history was significant for smoking cigarettes for 40 years. A urinary tract infection was suspected and she was treated with Ciprofloxacin but her symptoms did not improve.
An abdominopelvic ultrasound showed multiple leiomyomata and a normal right ovary. The left ovary was not visualized, but a large complex mass was seen in the left adnexa, 11.8 x 7.5 x 9.4 cm. A CT scan revealed a 1.4 cm nodule in the left lower lobe of the lung, multiple necrotic conglomerate lymph node masses within the mediastinum up to 3.7 cm, a 1.5 cm necrotic right pretracheal lymph node and the pelvic mass. Colonoscopy showed tubular and tubulovillous adenomas. Mammography was negative.
The patient underwent a total abdominal hysterectomy and bilateral salpingo-oophorectomy, appendectomy and pelvic biopsies.
Microscopic images:
Low power
Medium power
High power
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Pulmonary adenocarcinoma metastatic to ovary
Immunostains:
CK7
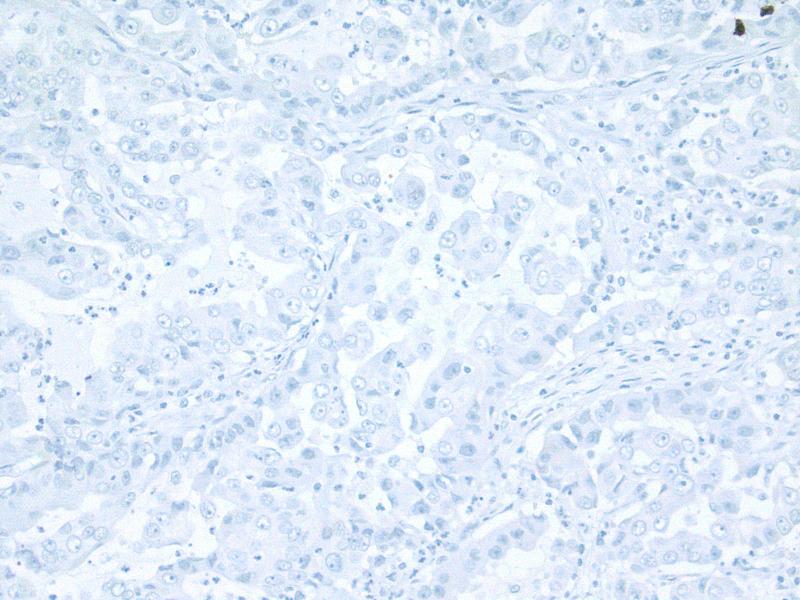
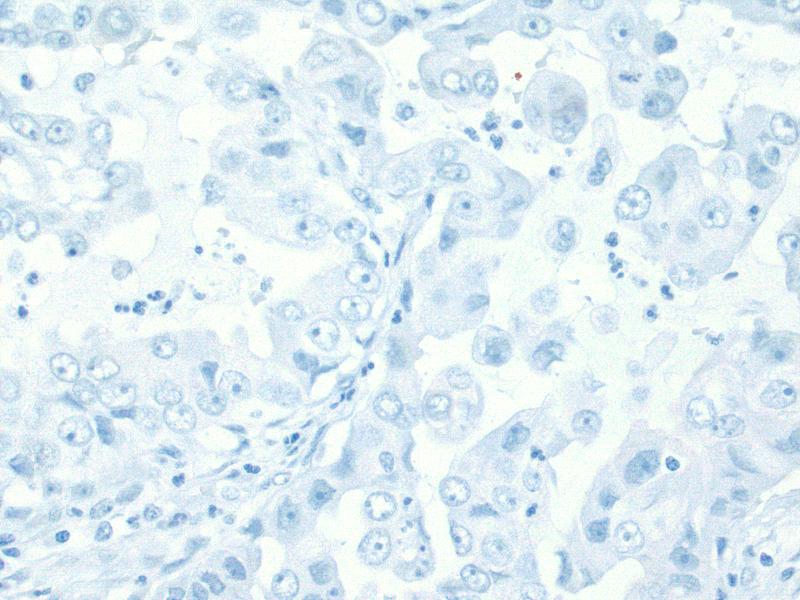
CK20 low power
CK20 high power
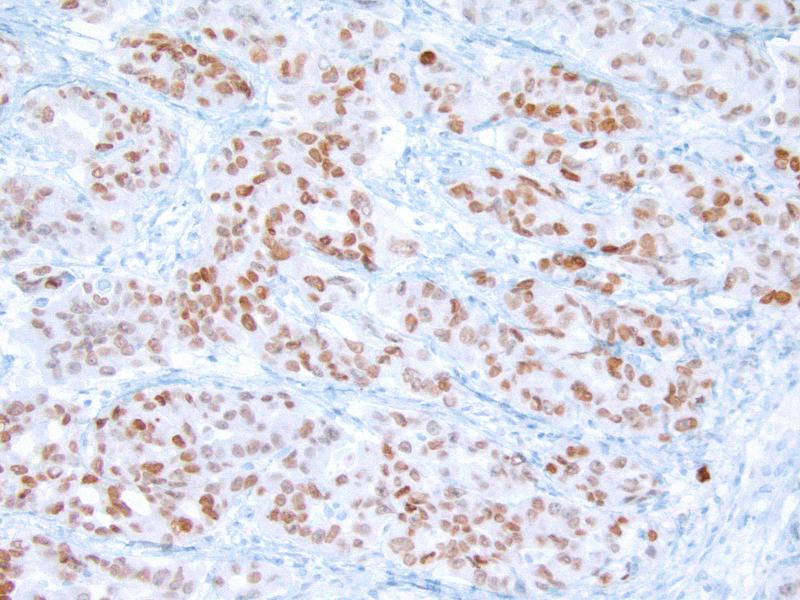
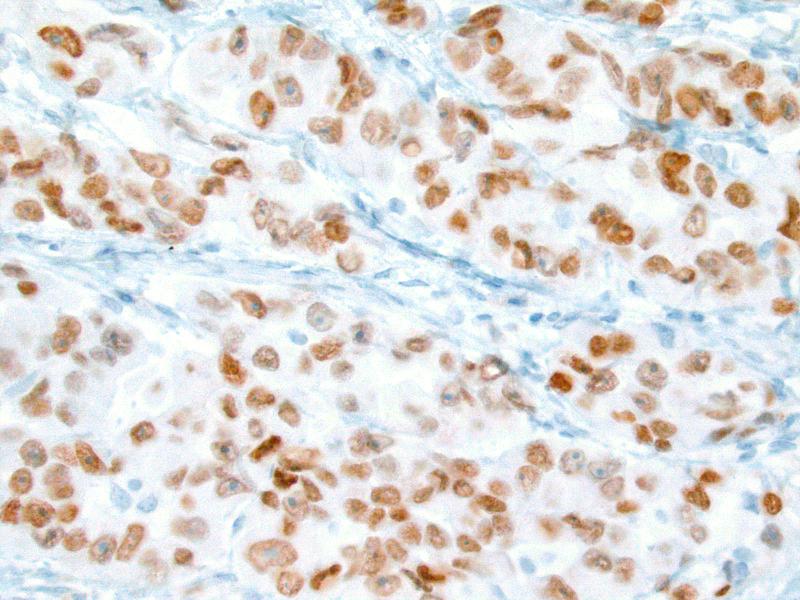
TTF low power
TTF high power
Discussion:
The tumor consists of cells arranged in nests and in some areas, forming glandular structures. The cells show high grade morphology with pleomorphism and prominent nucleoli.
CK7 showed strong, diffusely staining. CEA and ER (not shown) were focally positive, though ER was weak. TTF1 showed moderately strong, diffusely positive staining. p16 (not shown) also showed positive staining. CK20, mammaglobin, GCDFP, CDX2, villin, WT1, CD10 and vimentin all showed negative staining.
Based on histology, the tumor is a high grade adenocarcinoma and the staining pattern suggests lung origin.
While metastases to the ovary are common, metastasis of pulmonary adenocarcinoma to ovary is rare. In one study of 325 metastases to the female genital tract, only one lung primary was identified (Cancer 1984;53:1978). The metastasis was the first evidence of disease in only 21 cases. In autopsy series, pulmonary metastases to ovary may account for up to 2 - 5% of ovarian metastases (Gyn Oncol 1985;21:337). For diagnostic and treatment purposes, it is important to distinguish between primary ovarian cancer and metastases to the ovary. Metastatic papillary adenocarcinomas may be difficult to discriminate from ovarian primaries because of their resemblance to papillary serous adenocarcinoma of the ovary. When the adenocarcinoma is poorly differentiated, as in this case, the differential is broad, since it may include an ovarian primary as well as metastasis from any glandular organ.
Several case studies have demonstrated ovarian metastases from lung (Jpn J Clin Oncol 2003;33:404). In one study, the pulmonary origin was confirmed by immunohistochemical positivity for carcinoembryonic antigen, E-cadherin and surfactant in combination with negativity for CA125, N-cadherin and vimentin (Arch Pathol Lab Med 2002;126:1101). Another group demonstrated positive immunohistochemical staining for CK7 and TTF1 along with negativity for CK20, similar to the pattern in this case. Sensitivity and specificity of TTF1 for lung adenocarcinoma have been reported at 62% and 100%, respectively (Pathol Res Prac 2000;196:835). Another study documented the usefulness of TTF1, CK7, CK20 and PE-10 (Cancer 2001;93:330). When a poorly differentiated adenocarcinoma is located in the ovary, a large panel may be required to identify its origin and if the tumor is positive for CK7 and TTF1, while being negative for CK20, it is most likely a metastasis from lung but a mesonephric or mesonephric-like carcinoma must also be excluded (Pathology 2018;50:141).