25 June 2009 - Case #150
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Keith Kaplan, Mayo Clinic, Minnesota (USA).

Covance is pleased to announce the release of ACUITYAdvanced, the next generation of ACUITY biotin-free polymer detection and ACUITY Mouse on Mouse biotin-free polymer detection. ACUITYAdvanced offers crisp, clean enhanced staining with shorter incubation times than the previous version detection.
Visit the Covance website at www.covance.com or call to learn more about ACUITYAdvanced detection. 1.800.223.0796
Advertisement
Case #150
Clinical history:
A 37 year old woman presented with shortness of breath and abdominal pain consistent with cholecystitis. A cholecystectomy was planned but during her surgical workup, a pericardial mass was identified.
MRI (see below) showed a 12 x 12 x15-cm heterogeneous intrapericardial mass, which abutted the left ventricle and shifted the heart to the right. Portions of the mass also extended into the transverse sinus. Postcontrast images demonstrated avid arterial enhancement, as can be seen with sarcomas, particularly angiosarcoma. Small bilateral pleural effusions were present
The mass was excised.
Radiology images:

Gross images:

Microscopic images:

What is your diagnosis?
Diagnosis: Synovial sarcoma of the pericardium
Immunostains:


Discussion:
Synovial sarcoma usually affects the soft tissue of the joints and limbs. It can occur in the chest wall and lung but is extremely rare in the heart. It is associated with a t(X;18)(p11.2; q11.2) translocation in 90% of cases, leading to SSX1::SYT, SSX2::SYT or SSX4::SYT fusion genes (Clin Lung Cancer 2008;9:257, Mod Pathol 2002;15:679). Children and adults are equally affected but tumors may be more common in men in the heart (J Am Soc Endochardiogr 2007;20:197.e1).
Grossly, synovial sarcoma often presents as a bulky tumor that infiltrates the myocardium and pericardial surfaces. Histologically, it is biphasic with spindled and epithelioid cells or monophasic with only spindle cells. The spindle cell pattern is somewhat fascicular and has cellular and edematous areas. The spindle cells are small, compact and may be infiltrated by lymphocytes. The epithelioid areas, not prominent in this case, may form glands or nests and have lymphocytic infiltration. Although not obvious in this case, there is often a hemangiopericytoma-like vascular pattern (Am J Surg Pathol 2005;29:569). As in this case, the tumor is often positive for BCL2, CD99, pan-keratin and vimentin.
The differential diagnosis includes:
Synovial sarcoma of the heart has an overall poor prognosis. Treatment is usually excision, although the location of the tumor may make complete excision impossible. Chemotherapy and radiation therapy are often given.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Keith Kaplan, Mayo Clinic, Minnesota (USA).
Covance is pleased to announce the release of ACUITYAdvanced, the next generation of ACUITY biotin-free polymer detection and ACUITY Mouse on Mouse biotin-free polymer detection. ACUITYAdvanced offers crisp, clean enhanced staining with shorter incubation times than the previous version detection.
Visit the Covance website at www.covance.com or call to learn more about ACUITYAdvanced detection. 1.800.223.0796
Website news:
(1) We have updated Soft Tissue-Fibrohistiocytic and Adipose tissue tumors. The topics have our new format, with each topic on a separate page that is accessed by clicking on the link in the Table of Contents or Index. The advantages are faster loading of each page, easier to read pages with less scrolling, and the inclusion of thumbnails for most of the 600+ images.
(2) Congratulations to Dr. Alireza Zarineh, Allegheny General Hospital, Pennsylvania (USA) for completing our survey and being the second winner of $50 for our drawing. We will announce a new contest / drawing at the end of the summer.
Visit and follow our Blog to see recent updates to the website.
(1) We have updated Soft Tissue-Fibrohistiocytic and Adipose tissue tumors. The topics have our new format, with each topic on a separate page that is accessed by clicking on the link in the Table of Contents or Index. The advantages are faster loading of each page, easier to read pages with less scrolling, and the inclusion of thumbnails for most of the 600+ images.
(2) Congratulations to Dr. Alireza Zarineh, Allegheny General Hospital, Pennsylvania (USA) for completing our survey and being the second winner of $50 for our drawing. We will announce a new contest / drawing at the end of the summer.
Visit and follow our Blog to see recent updates to the website.
Case #150
Clinical history:
A 37 year old woman presented with shortness of breath and abdominal pain consistent with cholecystitis. A cholecystectomy was planned but during her surgical workup, a pericardial mass was identified.
MRI (see below) showed a 12 x 12 x15-cm heterogeneous intrapericardial mass, which abutted the left ventricle and shifted the heart to the right. Portions of the mass also extended into the transverse sinus. Postcontrast images demonstrated avid arterial enhancement, as can be seen with sarcomas, particularly angiosarcoma. Small bilateral pleural effusions were present
The mass was excised.
Radiology images:
Gross images:
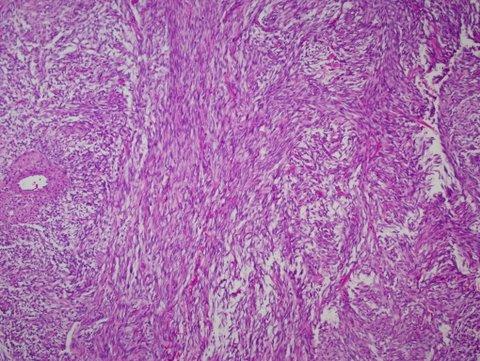
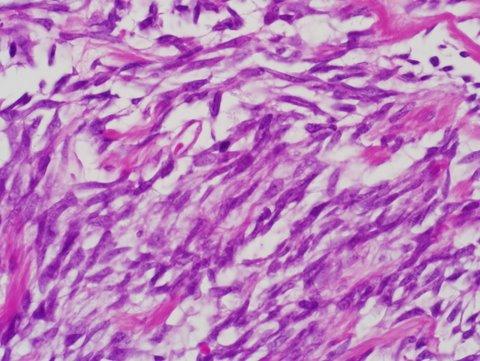
Microscopic images:
10x
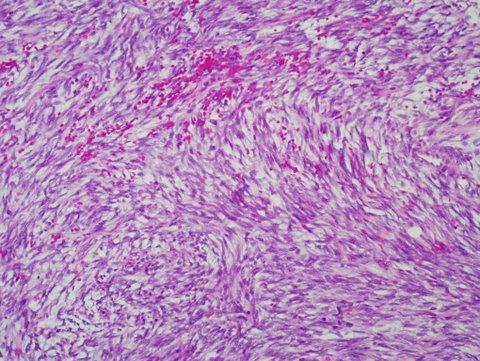
20x
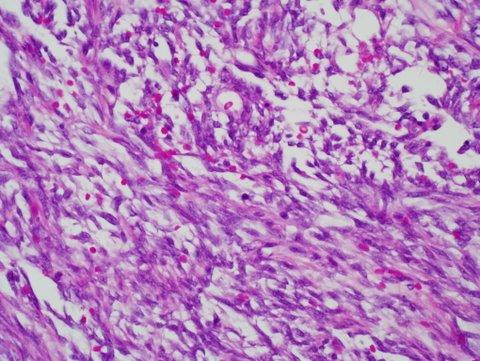
40x
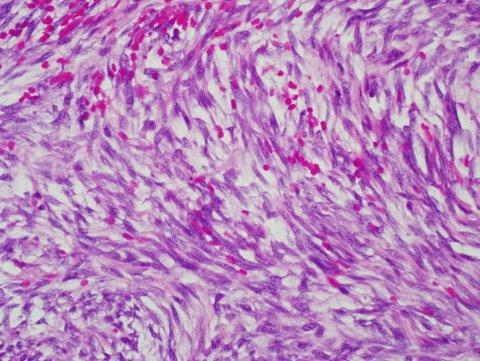
60x
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Synovial sarcoma of the pericardium
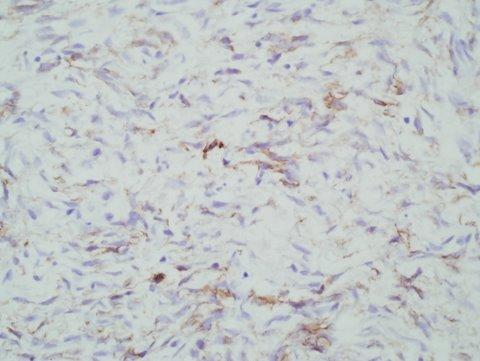
Immunostains:
BCL2
CD99
EMA
Discussion:
Synovial sarcoma usually affects the soft tissue of the joints and limbs. It can occur in the chest wall and lung but is extremely rare in the heart. It is associated with a t(X;18)(p11.2; q11.2) translocation in 90% of cases, leading to SSX1::SYT, SSX2::SYT or SSX4::SYT fusion genes (Clin Lung Cancer 2008;9:257, Mod Pathol 2002;15:679). Children and adults are equally affected but tumors may be more common in men in the heart (J Am Soc Endochardiogr 2007;20:197.e1).
Grossly, synovial sarcoma often presents as a bulky tumor that infiltrates the myocardium and pericardial surfaces. Histologically, it is biphasic with spindled and epithelioid cells or monophasic with only spindle cells. The spindle cell pattern is somewhat fascicular and has cellular and edematous areas. The spindle cells are small, compact and may be infiltrated by lymphocytes. The epithelioid areas, not prominent in this case, may form glands or nests and have lymphocytic infiltration. Although not obvious in this case, there is often a hemangiopericytoma-like vascular pattern (Am J Surg Pathol 2005;29:569). As in this case, the tumor is often positive for BCL2, CD99, pan-keratin and vimentin.
The differential diagnosis includes:
- Mesothelioma: larger spindle cells with more pleomorphism, usually no infiltration of myocardium, no t(X;18) or fusion gene
- Malignant peripheral nerve sheath tumor: 50% associated with neurofibromatosis, also associated with major nerve or continuous with neurofibroma; often palisading with monomorphic serpentine cells, geographic necrosis with tumor palisading at the edges, frequent mitotic figures, often bizarre tumor cells, usually CD99+, variable S100 (62%), CD57, p53
- Fibrosarcoma: often left atrium, herringbone pattern of compact fibroblastic type cells with tapered nuclei in collagenous or myxoid matrix; no intracytoplasmic glycogen, no perinuclear vacuoles, no pleomorphism, no histiocytoid cells
- Myxoma: tumor is dominated by myxoid matrix; also complex structures resembling cords, nests, rings or poorly formed glands, often surrounding blood vessels; composed of stellate or globular myxoma cells with abundant eosinophilic cytoplasm, indistinct cell borders, oval nucleus with open chromatin and indistinct nuclei
Synovial sarcoma of the heart has an overall poor prognosis. Treatment is usually excision, although the location of the tumor may make complete excision impossible. Chemotherapy and radiation therapy are often given.