11 June 2009 - Case #149
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Asmaa Gaber Abdou and Dr. Nancy Youssef Asaad, Menoufiya University, Egypt.
PathLab Coding Solutions SM is designed to assist in minimizing risks associated with over-coding and lack of documentation while maximizing reimbursement through proper coding practices.
Subscribers will be able to resolve simple to complex coding issues and remain up-to-date with changes in coding procedures by utilizing the Automated Coding Assistant, Resource Center and Coding Consultant Dashboard.
To learn more about PathLab Coding Solutions, visit www.PathLabCoding.com or contact Leigh Polk with PSA at 800-832-5270 ext 2941.
Advertisement
Case #149
Clinical history:
A 50 year old woman presented with a thigh mass, which was excised.
Microscopic images:
What is your diagnosis?
Diagnosis: Parachordoma
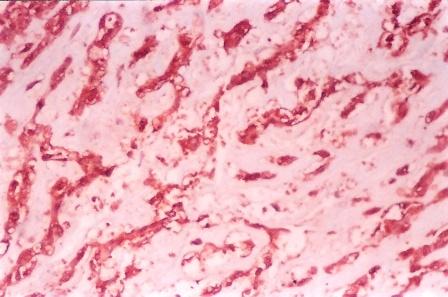
Immunostains:

Discussion:
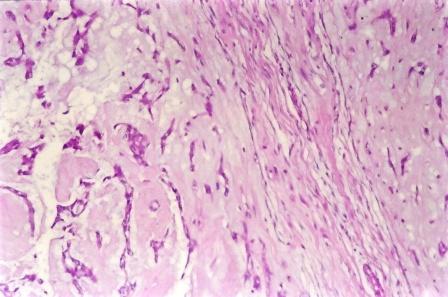
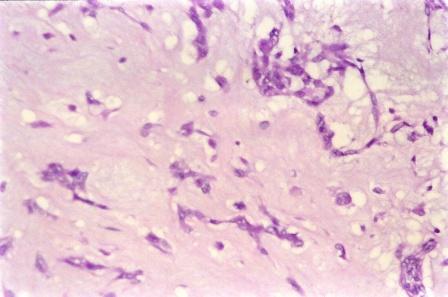
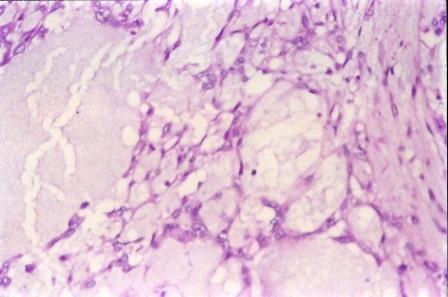
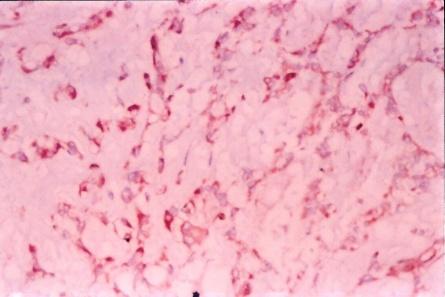
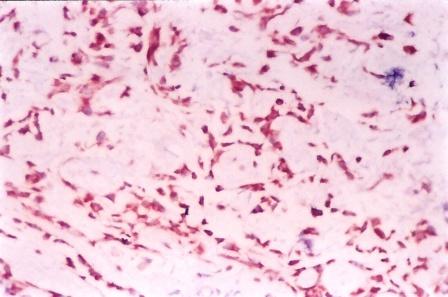
The mass showed cords of cells floating in myxoid or mucoid material, admixed with occasional physaliferous (multivacuolated) cells. The original diagnosis was liposarcoma, but after review immunostains were performed showing tumor cells that were immunoreactive for cytokeratin, EMA, S100 and vimentin, which confirmed the revised diagnosis of parachordoma.
Parachordoma is a rare peripheral tumor which usually affects deep soft tissues adjacent to bones and tendons. It is characterized by myxoid or hyaline material containing large, rounded eosinophilic cells. The tumor almost always contains a small number of physaliferous cells (Am J Surg Pathol 1999;23:1059). It stains positively for S100, vimentin, CK8 / CK18 and EMA and negative for CK1 / CK10. Type 4 collagen is also present around nests of cells.
The differential diagnosis includes:
Parachordomas typically have benign behavior. Wide resection is usually adequate treatment and recurrences are rare (Adv Anat Pathol 2000;7:141). However, to date, 5 cases of metastatic tumor have been reported (J Cutan Pathol 2009;36:270).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Asmaa Gaber Abdou and Dr. Nancy Youssef Asaad, Menoufiya University, Egypt.
PathLab Coding Solutions SM is designed to assist in minimizing risks associated with over-coding and lack of documentation while maximizing reimbursement through proper coding practices.
Subscribers will be able to resolve simple to complex coding issues and remain up-to-date with changes in coding procedures by utilizing the Automated Coding Assistant, Resource Center and Coding Consultant Dashboard.
To learn more about PathLab Coding Solutions, visit www.PathLabCoding.com or contact Leigh Polk with PSA at 800-832-5270 ext 2941.
Website news:
(1) Congratulations to Dr. Roopa Paulose, Hatton Health, United Kingdom. She received a check for $50 for completing our survey and winning our drawing. Thanks to all who completed the survey, which helps us improve our website.
(2) We are changing the format of our textbook so each topic has a separate page. The advantages are (a) easier to read, (b) ability to include thumbnails of images, (c) better targeting of search engines to the correct topic, (d) pages will load faster with less scrolling.
Visit and follow our Blog to see recent updates to the website.
(1) Congratulations to Dr. Roopa Paulose, Hatton Health, United Kingdom. She received a check for $50 for completing our survey and winning our drawing. Thanks to all who completed the survey, which helps us improve our website.
(2) We are changing the format of our textbook so each topic has a separate page. The advantages are (a) easier to read, (b) ability to include thumbnails of images, (c) better targeting of search engines to the correct topic, (d) pages will load faster with less scrolling.
Visit and follow our Blog to see recent updates to the website.
Case #149
Clinical history:
A 50 year old woman presented with a thigh mass, which was excised.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Parachordoma
Immunostains:
Cytokeratin
EMA
S100
Vimentin
Discussion:
The mass showed cords of cells floating in myxoid or mucoid material, admixed with occasional physaliferous (multivacuolated) cells. The original diagnosis was liposarcoma, but after review immunostains were performed showing tumor cells that were immunoreactive for cytokeratin, EMA, S100 and vimentin, which confirmed the revised diagnosis of parachordoma.
Parachordoma is a rare peripheral tumor which usually affects deep soft tissues adjacent to bones and tendons. It is characterized by myxoid or hyaline material containing large, rounded eosinophilic cells. The tumor almost always contains a small number of physaliferous cells (Am J Surg Pathol 1999;23:1059). It stains positively for S100, vimentin, CK8 / CK18 and EMA and negative for CK1 / CK10. Type 4 collagen is also present around nests of cells.
The differential diagnosis includes:
- Liposarcoma: these tumors have variable lipoblasts, which are also multivacuolated but have atypical nuclei. They also have a prominent component indicated by the subtype (well differentiated, dedifferentiated, myxoid / round cell, pleomorphic or sclerosing) and are keratin negative.
- Extraskeletal myxoid chondrosarcoma: these tumors have a neoplastic cartilaginous component with long chains of cells, are keratin negative and have a characteristic t(9;22).
- Chordoma (primary or metastatic): primary chordomas occur on the craniospinal axis, and have prominent physaliferous cells. Some authors consider the immunostaining pattern to be similar to parachordoma but some believe that CK1 / CK10 staining is helpful to differentiate these entities (Pathol Int 2004;54:364). Metastatic chordoma must be ruled out clinically.
Parachordomas typically have benign behavior. Wide resection is usually adequate treatment and recurrences are rare (Adv Anat Pathol 2000;7:141). However, to date, 5 cases of metastatic tumor have been reported (J Cutan Pathol 2009;36:270).