
25 February 2009 - Case #140
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Julia Braza, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA).
Case #140
Clinical history:
A 68 year old woman with a history of AML presented with a five month history of progressive eruption of violaceous firm nodules in the umbilicus, groin, trunk and scalp.
A left breast punch biopsy was performed.
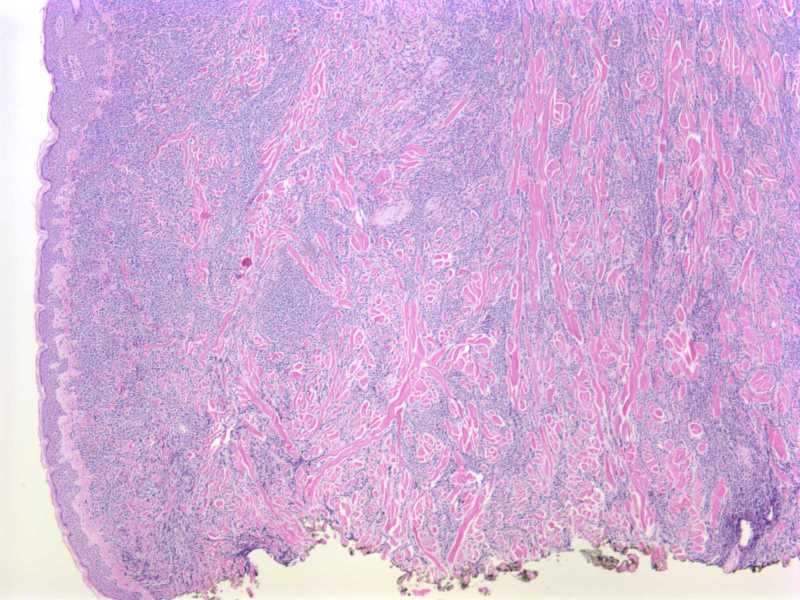
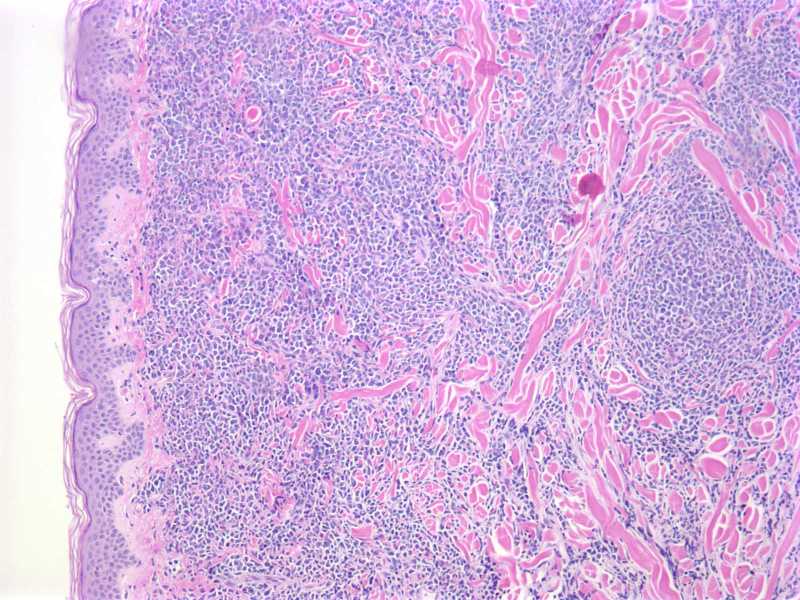
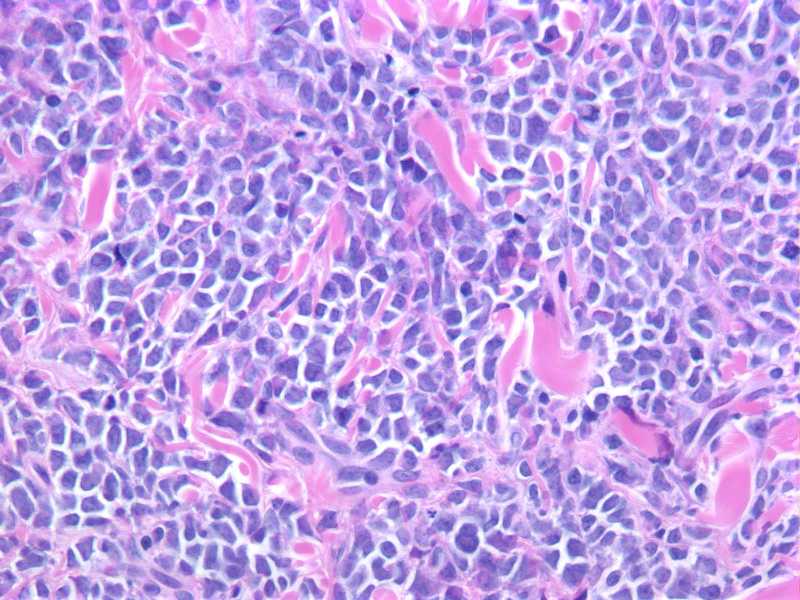
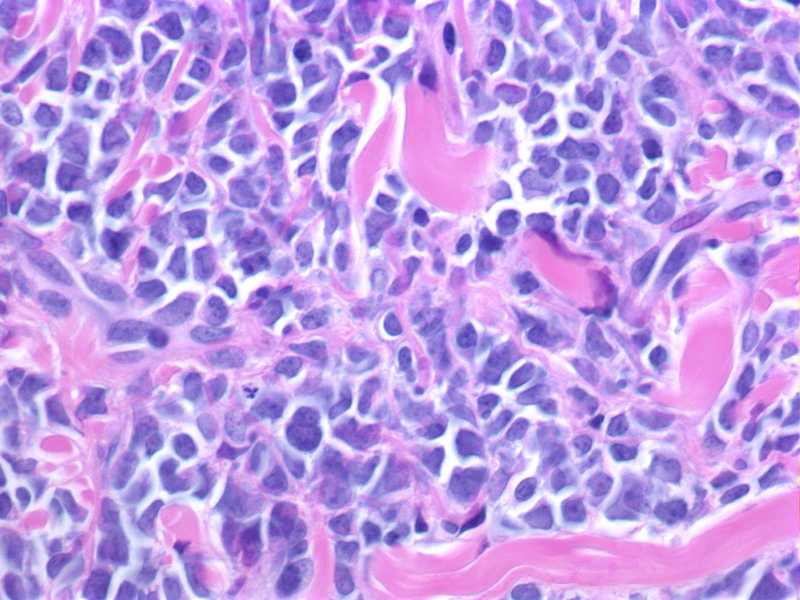
Microscopic images:
What is your diagnosis?
Diagnosis: Leukemia cutis
Immunostains:
Discussion:
The dermis and superficial subcutaneous fat are diffusely infiltrated by a monotonous population of large cells with a high nuclear to cytoplasmic ratio, round to slightly irregular nuclear contours, finely dispersed chromatin and prominent nucleoli. The tumor cells are diffusely immunoreactive for CD45, CD117 and CD43, with focal expression of CD68. Myeloperoxidase (not shown) highlights a small subset of tumor cells. The cells are negative for CD34, TdT, CD20, BCL1 and CD56. CD3 and CD4 (not shown) highlight scant, admixed T lymphocytes.
Overall, the morphologic and immunophenotypic findings are consistent with tissue infiltration by acute myelogenous leukemia. The prior AML subtype is unknown.
Leukemia cutis includes cutaneous manifestations of any type of leukemia. It can be difficult to clinically distinguish from other skin lesions. Patients usually have preexisting systemic leukemia but occasionally skin involvement precedes bone marrow or peripheral blood involvement (Am J Clin Pathol 2008;129:130).
Myeloid leukemia with monocytic differentiation more commonly involves the skin than other types of myeloid leukemia. It may also have an accompanying vasculitis (Am J Clin Pathol 1997;107:637). CD68 and lysozyme immunostains are sensitive for monocytes / macrophages, although not specific (J Cutan Pathol 2008;35:180).
Leukemia cutis is associated with aggressive behavior and short survival (J Am Acad Dermatol 1999;40:966). Treatment is systemic chemotherapy directed at eradicating the leukemic clone.
References: eMedicine: Leukemia Cutis [Accessed 2 May 2024]
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Julia Braza, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA).
Case #140
Clinical history:
A 68 year old woman with a history of AML presented with a five month history of progressive eruption of violaceous firm nodules in the umbilicus, groin, trunk and scalp.
A left breast punch biopsy was performed.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Leukemia cutis
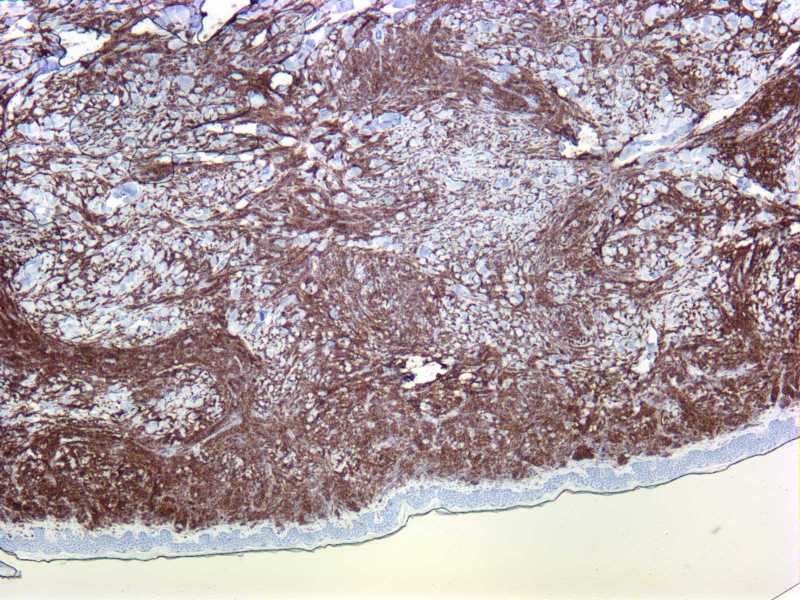
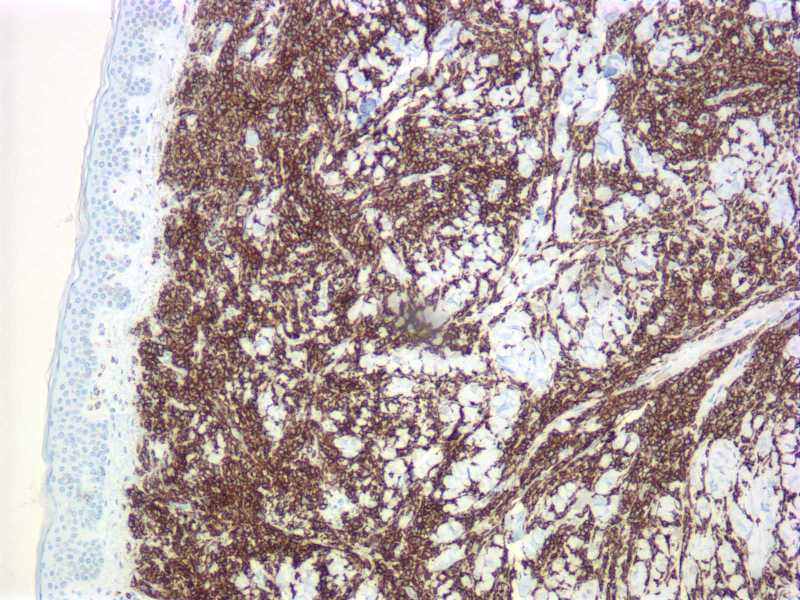
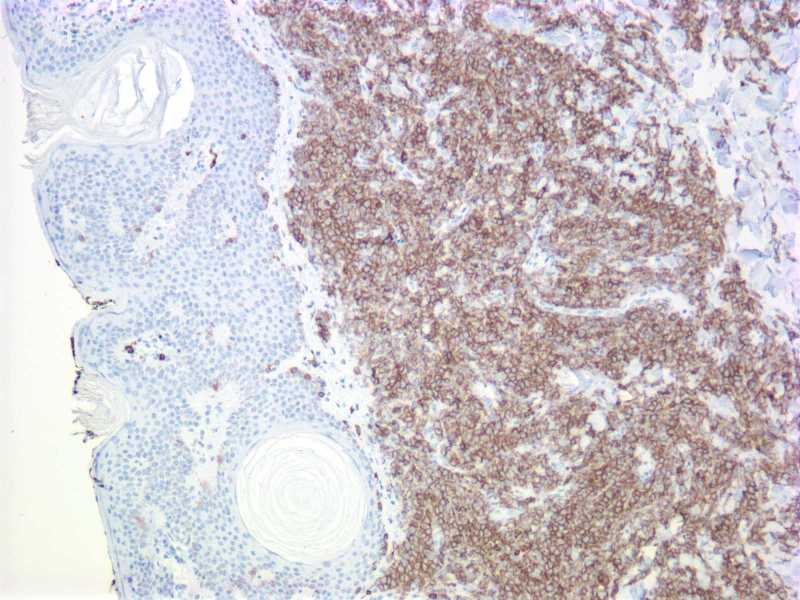
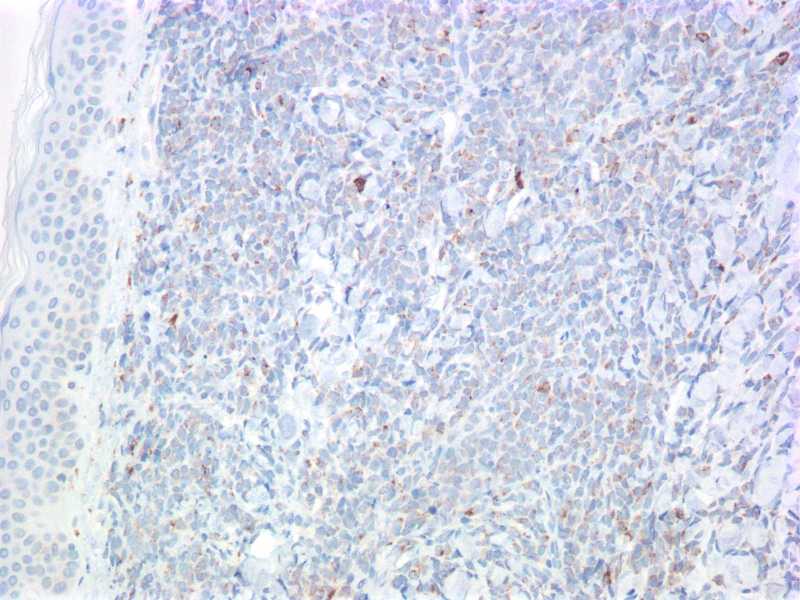
Immunostains:
CD45
CD43
CD43
CD43
Discussion:
The dermis and superficial subcutaneous fat are diffusely infiltrated by a monotonous population of large cells with a high nuclear to cytoplasmic ratio, round to slightly irregular nuclear contours, finely dispersed chromatin and prominent nucleoli. The tumor cells are diffusely immunoreactive for CD45, CD117 and CD43, with focal expression of CD68. Myeloperoxidase (not shown) highlights a small subset of tumor cells. The cells are negative for CD34, TdT, CD20, BCL1 and CD56. CD3 and CD4 (not shown) highlight scant, admixed T lymphocytes.
Overall, the morphologic and immunophenotypic findings are consistent with tissue infiltration by acute myelogenous leukemia. The prior AML subtype is unknown.
Leukemia cutis includes cutaneous manifestations of any type of leukemia. It can be difficult to clinically distinguish from other skin lesions. Patients usually have preexisting systemic leukemia but occasionally skin involvement precedes bone marrow or peripheral blood involvement (Am J Clin Pathol 2008;129:130).
Myeloid leukemia with monocytic differentiation more commonly involves the skin than other types of myeloid leukemia. It may also have an accompanying vasculitis (Am J Clin Pathol 1997;107:637). CD68 and lysozyme immunostains are sensitive for monocytes / macrophages, although not specific (J Cutan Pathol 2008;35:180).
Leukemia cutis is associated with aggressive behavior and short survival (J Am Acad Dermatol 1999;40:966). Treatment is systemic chemotherapy directed at eradicating the leukemic clone.
References: eMedicine: Leukemia Cutis [Accessed 2 May 2024]
