25 November 2008 - Case #135
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
We thank Dr. Suma B. Pillai, PSG Institute of Medical Science and Research, Peelamedu, Coimbatore, Tamil Nadu (India) for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
2nd Annual Winter Update in Clinical and Laboratory Medicine:
Clinical Chemistry, Immunology, Microbiology and Molecular Medicine
This 24 hour review and update in the areas of clinical chemistry, immunology, microbiology, and molecular medicine is intended to improve knowledge about the pathogenesis and clinical manifestations of a wide variety of metabolic, infectious, immunologic, and genetic disorders along with the selection, performance, and interpretation of clinical laboratory tests.
Approximately 60% of the diagnoses in medicine are based on the results of laboratory testing. The 2nd Annual Winter Update program will address this major gap in knowledge and inform the participant about developments in clinical laboratory testing and their relevance to clinical medicine. The conference is held at The Canyons in Park City, Utah.
Advertisement
Case #135
Clinical history:
A 50 year old woman presented with vaginal bleeding for 25 days. She had two children with a normal full term vaginal delivery. There was no history of abortion or curettage. Vaginal examination showed an elongated cervix and a small polyp in the anterior lip. The uterus was bulky and retroverted. Fornices were unremarkable. Abdominal ultrasound was normal. A polypectomy was performed, and produced gray-white tissue measuring 0.5 x 0.3 x 0.2 cm.
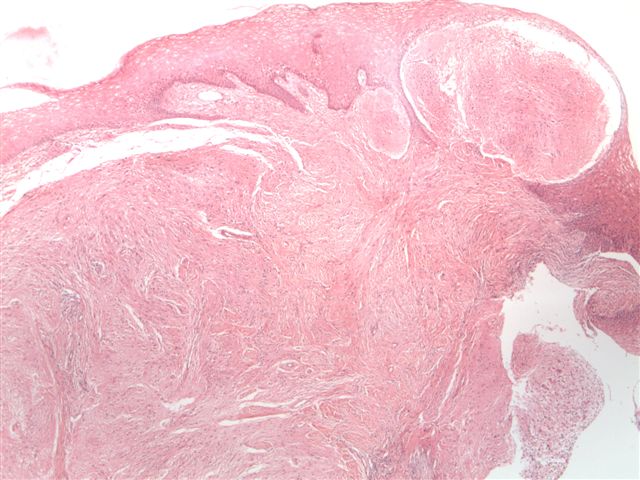
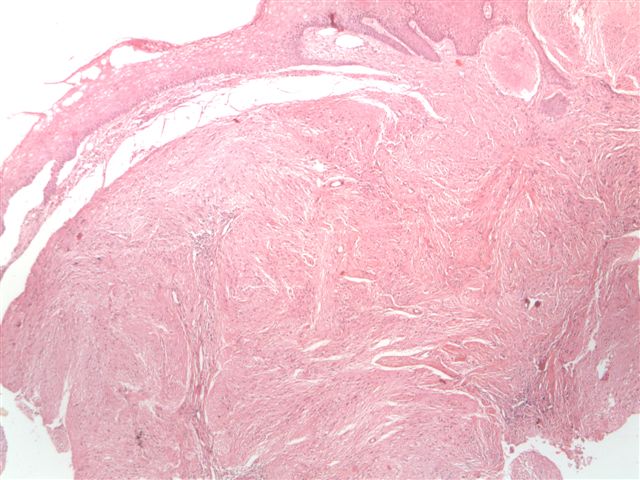
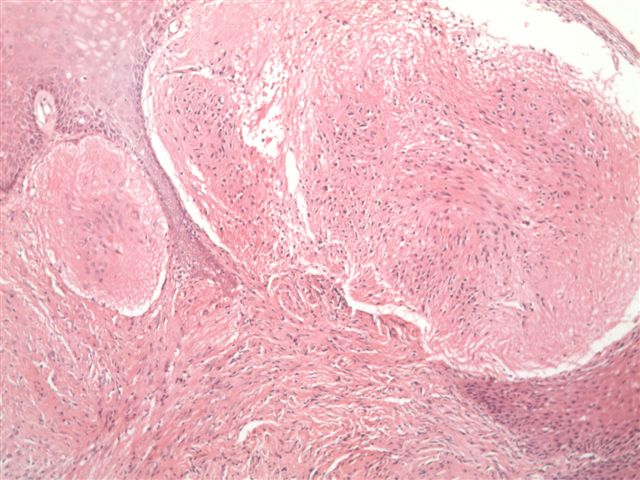
Microscopic images:


What is your diagnosis?
Diagnosis: Glial polyp of cervix
Discussion:
These features are classic for a glial polyp of the cervix. The polyp was covered by stratified squamous epithelium and was composed of mature glial tissue with moderate cellularity. The glial cells were bland with round / oval nuclei in a fibrillary background. There was no atypia or mitotic figures. GFAP stained the glial cells and stroma. The fibrillary processes are typically immunoreactive for PTAH (not performed in this case). In some cases, bone and cartilage have been found.
Cervical glial polyps are rare, with < 100 cases reported. Generally they are endocervical but ectocervical polyps have been reported (Obstet Gynecol 1983;61:261).
How does glial tissue appear in the cervix? The most widely accepted theory is implantation of fetal brain tissue during abortion or curettage, as illustrated in an 18 year old woman post curettage for spontaneous abortion (Am J Clin Pathol 1980;73:718). Other possible mechanisms include development of a teratoma, ectopic glial tissue or neoplasia of Müllerian origin.
Cervical glial polyps are benign and excision is generally curative, although it may recur. No cases of malignant behavior have been reported.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
We thank Dr. Suma B. Pillai, PSG Institute of Medical Science and Research, Peelamedu, Coimbatore, Tamil Nadu (India) for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Clinical Chemistry, Immunology, Microbiology and Molecular Medicine
This 24 hour review and update in the areas of clinical chemistry, immunology, microbiology, and molecular medicine is intended to improve knowledge about the pathogenesis and clinical manifestations of a wide variety of metabolic, infectious, immunologic, and genetic disorders along with the selection, performance, and interpretation of clinical laboratory tests.
Approximately 60% of the diagnoses in medicine are based on the results of laboratory testing. The 2nd Annual Winter Update program will address this major gap in knowledge and inform the participant about developments in clinical laboratory testing and their relevance to clinical medicine. The conference is held at The Canyons in Park City, Utah.
Case #135
Clinical history:
A 50 year old woman presented with vaginal bleeding for 25 days. She had two children with a normal full term vaginal delivery. There was no history of abortion or curettage. Vaginal examination showed an elongated cervix and a small polyp in the anterior lip. The uterus was bulky and retroverted. Fornices were unremarkable. Abdominal ultrasound was normal. A polypectomy was performed, and produced gray-white tissue measuring 0.5 x 0.3 x 0.2 cm.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Glial polyp of cervix
Discussion:
These features are classic for a glial polyp of the cervix. The polyp was covered by stratified squamous epithelium and was composed of mature glial tissue with moderate cellularity. The glial cells were bland with round / oval nuclei in a fibrillary background. There was no atypia or mitotic figures. GFAP stained the glial cells and stroma. The fibrillary processes are typically immunoreactive for PTAH (not performed in this case). In some cases, bone and cartilage have been found.
Cervical glial polyps are rare, with < 100 cases reported. Generally they are endocervical but ectocervical polyps have been reported (Obstet Gynecol 1983;61:261).
How does glial tissue appear in the cervix? The most widely accepted theory is implantation of fetal brain tissue during abortion or curettage, as illustrated in an 18 year old woman post curettage for spontaneous abortion (Am J Clin Pathol 1980;73:718). Other possible mechanisms include development of a teratoma, ectopic glial tissue or neoplasia of Müllerian origin.
Cervical glial polyps are benign and excision is generally curative, although it may recur. No cases of malignant behavior have been reported.