7 August 2008 - Case #126
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Renuka Agrawal, Loma Linda University Medical Center, California (USA).
Case #126
Clinical history:
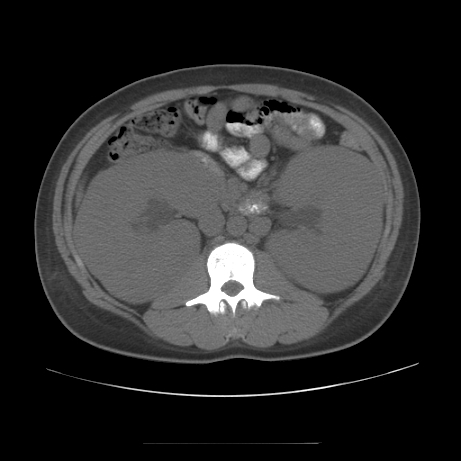
A 19 year old Hispanic man presented with hypertension and renal insufficiency (serum creatinine of 7.1 mg/dl). The peripheral blood smear showed pancytopenia but no circulating blasts. A CT scan demonstrated bilateral renal enlargement with lymphadenopathy in the retroperitoneum and neck.
A core biopsy was obtained and immunostains were performed (CD10, CD34, CD79a, TdT).
Radiology images:
Microscopic images:
What is your diagnosis?
Diagnosis: Pre-B acute lymphoblastic lymphoma involving the kidneys
Immunostains:

Discussion:
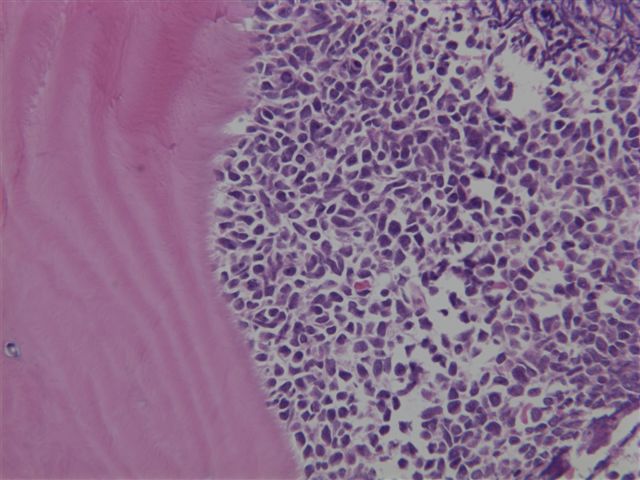
A bone marrow biopsy was also obtained, which showed a diffuse infiltration by tumor cells with a similar morphology as the renal biopsy.
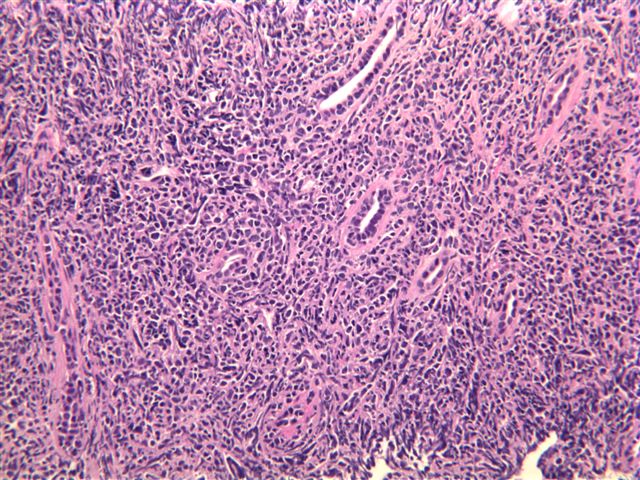
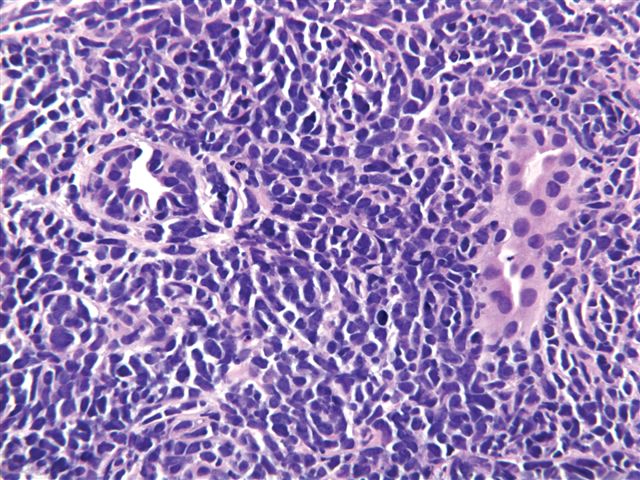
The renal biopsy showed a diffuse infiltrate of monotonous blastoid cells obliterating the normal renal architecture. The bone marrow biopsy showed a similar population of cells replacing most of the marrow. Immunophenotyping by flow cytometry and immunohistochemistry showed that the tumor cells coexpress CD19, CD20, CD10, CD34, CD38, CD79a, HLA-DR and TdT.
Precursor B cell acute lymphoblastic leukemia / lymphoma (ALL) is a common pediatric hematologic malignancy. Although renal failure due to tumor lysis is a recognized complication of treatment, initial presentation with renal failure is distinctly uncommon. ALL must be considered among the causes of acute renal failure when the kidneys are enlarged. Careful morphologic study and immunophenotyping by flow cytometry or immunohistochemistry is helpful to arrive at the correct diagnosis and to avoid confusion with other small blue cell tumors which may involve the kidney, such as Wilm tumor, small cell carcinoma or Ewing sarcoma / primitive neuroectodermal tumor (J Pediatr Hematol Oncol 2008;30:471).
References: DeVita: Lymphomas and Leukemias: Cancer: Principles & Practice of Oncology, 10th Edition, 2015, Pediatr Nephrol 2005;20:679, Indian Pediatr 2001;38:407, J Urol 1983;129:364, Pathologe 2003;24:460, DeVita: Cancer: Principles and Practices of Oncology, 4th Edition, 1993
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Renuka Agrawal, Loma Linda University Medical Center, California (USA).
Case #126
Clinical history:
A 19 year old Hispanic man presented with hypertension and renal insufficiency (serum creatinine of 7.1 mg/dl). The peripheral blood smear showed pancytopenia but no circulating blasts. A CT scan demonstrated bilateral renal enlargement with lymphadenopathy in the retroperitoneum and neck.
A core biopsy was obtained and immunostains were performed (CD10, CD34, CD79a, TdT).
Radiology images:
Microscopic images:
Bone marrow biopsy
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Pre-B acute lymphoblastic lymphoma involving the kidneys
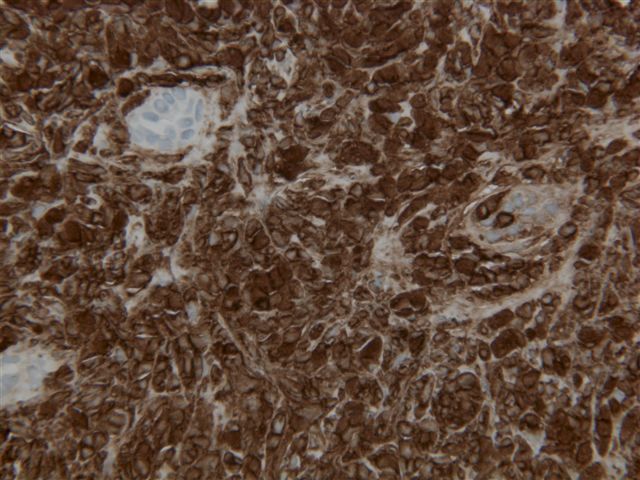
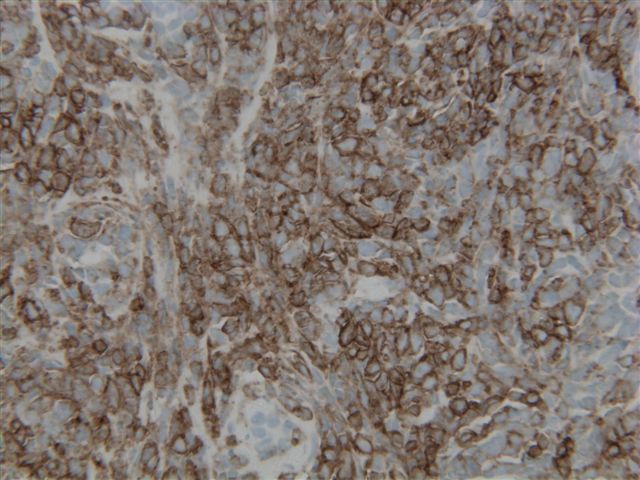
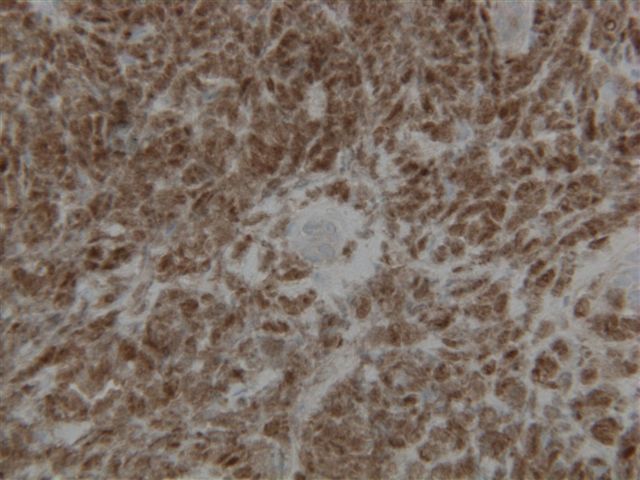
Immunostains:
CD10
CD34
CD79a
TdT
Discussion:
A bone marrow biopsy was also obtained, which showed a diffuse infiltration by tumor cells with a similar morphology as the renal biopsy.
The renal biopsy showed a diffuse infiltrate of monotonous blastoid cells obliterating the normal renal architecture. The bone marrow biopsy showed a similar population of cells replacing most of the marrow. Immunophenotyping by flow cytometry and immunohistochemistry showed that the tumor cells coexpress CD19, CD20, CD10, CD34, CD38, CD79a, HLA-DR and TdT.
Precursor B cell acute lymphoblastic leukemia / lymphoma (ALL) is a common pediatric hematologic malignancy. Although renal failure due to tumor lysis is a recognized complication of treatment, initial presentation with renal failure is distinctly uncommon. ALL must be considered among the causes of acute renal failure when the kidneys are enlarged. Careful morphologic study and immunophenotyping by flow cytometry or immunohistochemistry is helpful to arrive at the correct diagnosis and to avoid confusion with other small blue cell tumors which may involve the kidney, such as Wilm tumor, small cell carcinoma or Ewing sarcoma / primitive neuroectodermal tumor (J Pediatr Hematol Oncol 2008;30:471).
References: DeVita: Lymphomas and Leukemias: Cancer: Principles & Practice of Oncology, 10th Edition, 2015, Pediatr Nephrol 2005;20:679, Indian Pediatr 2001;38:407, J Urol 1983;129:364, Pathologe 2003;24:460, DeVita: Cancer: Principles and Practices of Oncology, 4th Edition, 1993