10 July 2008 - Case #124
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. John W. Turner, Commonwealth Laboratory Consultants, Richmond, Virginia (USA).
Case #124
Clinical history:
A 50 year old man presented with an 8 cm duodenal polyp. Five years ago, he complained of gastric pain and blood in his stool. At endoscopy, he had a 5 cm duodenal polyp, diagnosed as benign. However, removal of the polyp was delayed for years because a CT scan found a renal cell carcinoma, which was excised. At his recent surgery for the duodenal polyp, a wet villous mass was found that abutted the ampulla of Vater.
Gross images:




Microscopic images:
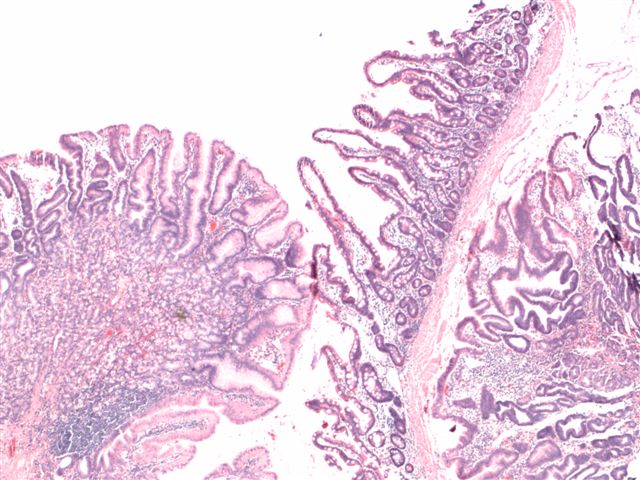
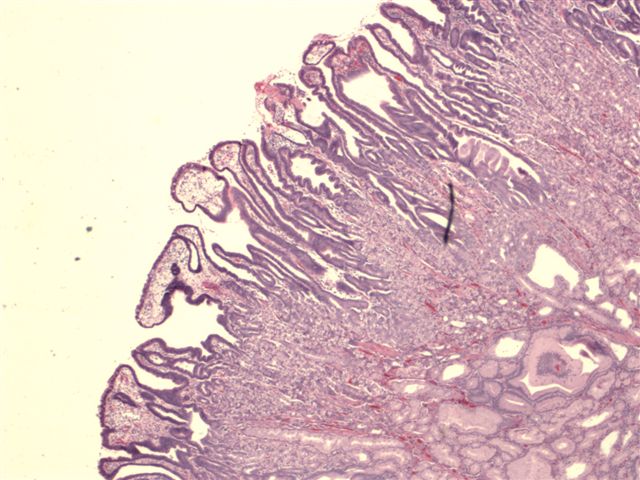
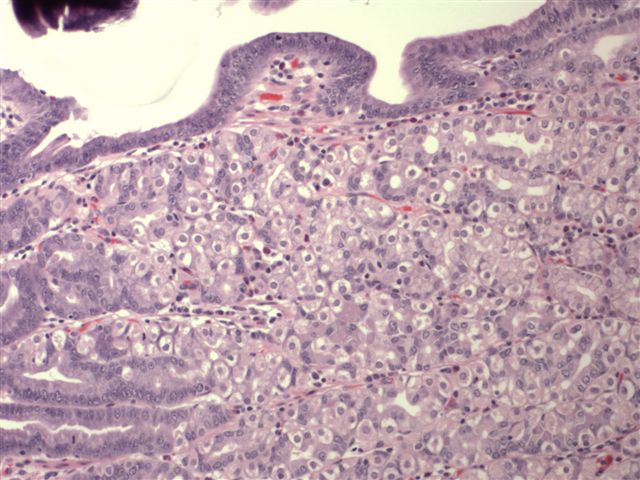

What is your diagnosis?
Diagnosis: Hyperplastic polyp of gastric metaplasia / gastric heterotopia
Discussion:
This case demonstrates the presence of mature gastric tissue in the duodenum. Heterotopia is a developmental anomaly, defined as the presence of mature tissue in a location where it is not normally found. Gastric heterotopia has been described in the esophagus (inlet patch), duodenum, gallbladder, Meckels diverticulum and other sites in the bowel. It is associated with diarrhea, obstruction, dyspepsia, ulceration and GI bleeding (Pediatr Dev Pathol 2000;3:277).
Grossly, heterotopia usually presents as one or more nodules or sessile polyps. Microscopically, it consists of fundic type mucosa with chief and parietal cells, lined by foveolar epithelium, with a full mucosal thickness, forming a mucosal island. It is rarely associated with gastric type adenomas (Virchows Arch 1999;435:452).
Heterotopia differs from metaplasia. Metaplasia is the change from one type of fully differentiated tissue to another fully differentiated tissue, usually due to chronic inflammation. The lower esophagus and duodenal bulb are common sites of gastric metaplasia, which may occur as a protective response to gastric acid. Gastric metaplasia only occupies part of the mucosal thickness and intermingles with native tissue. It typically is microscopic and does not present with any gross findings. Histologically, it lacks the specialized cells of fundic type mucosa. It may be important to distinguish gastric metaplasia from heterotopia, because metaplasia is associated with duodenitis and often H. pylori, which may require treatment (Braz J Med Biol Res 2007;40:897, Dig Liver Dis 2002;34:16).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. John W. Turner, Commonwealth Laboratory Consultants, Richmond, Virginia (USA).
Case #124
Clinical history:
A 50 year old man presented with an 8 cm duodenal polyp. Five years ago, he complained of gastric pain and blood in his stool. At endoscopy, he had a 5 cm duodenal polyp, diagnosed as benign. However, removal of the polyp was delayed for years because a CT scan found a renal cell carcinoma, which was excised. At his recent surgery for the duodenal polyp, a wet villous mass was found that abutted the ampulla of Vater.
Gross images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Hyperplastic polyp of gastric metaplasia / gastric heterotopia
Discussion:
This case demonstrates the presence of mature gastric tissue in the duodenum. Heterotopia is a developmental anomaly, defined as the presence of mature tissue in a location where it is not normally found. Gastric heterotopia has been described in the esophagus (inlet patch), duodenum, gallbladder, Meckels diverticulum and other sites in the bowel. It is associated with diarrhea, obstruction, dyspepsia, ulceration and GI bleeding (Pediatr Dev Pathol 2000;3:277).
Grossly, heterotopia usually presents as one or more nodules or sessile polyps. Microscopically, it consists of fundic type mucosa with chief and parietal cells, lined by foveolar epithelium, with a full mucosal thickness, forming a mucosal island. It is rarely associated with gastric type adenomas (Virchows Arch 1999;435:452).
Heterotopia differs from metaplasia. Metaplasia is the change from one type of fully differentiated tissue to another fully differentiated tissue, usually due to chronic inflammation. The lower esophagus and duodenal bulb are common sites of gastric metaplasia, which may occur as a protective response to gastric acid. Gastric metaplasia only occupies part of the mucosal thickness and intermingles with native tissue. It typically is microscopic and does not present with any gross findings. Histologically, it lacks the specialized cells of fundic type mucosa. It may be important to distinguish gastric metaplasia from heterotopia, because metaplasia is associated with duodenitis and often H. pylori, which may require treatment (Braz J Med Biol Res 2007;40:897, Dig Liver Dis 2002;34:16).