
Lymph nodes & spleen, nonlymphoma
Lymph nodes-inflammatory / reactive disorders
Rosai-Dorfman disease (RDD)
Authors: Aishwarya Ravindran, M.D., Karen L. Rech, M.D.
Editorial Board Member: Elizabeth Courville, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 6 August 2021
Last staff update: 12 February 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Rosai-Dorfman disease [TI] Lymph nodes free full text[sb]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ravindran A, Rech KL. Rosai-Dorfman disease (RDD). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphnodessinushistiocytosiswithmassivelymph.html. Accessed April 24th, 2024.
Definition / general
- Rare, non-Langerhans cell histiocytosis with heterogeneous clinical features
- Described in 1960s as a self limiting condition involving the lymph nodes (Arch Pathol 1969;87:63)
- Extranodal involvement in approximately 40% of cases; may be limited or disseminated disease (Blood 2018;131:2877)
- May be familial or associated with neoplasia or immune disease (Blood 2016;127:2672)
Essential features
- Clinical features depend on the site(s) involved and disease associations
- Classic (nodal) Rosai-Dorfman disease (RDD) and cutaneous RDD often self limited and benign
- Disseminated RDD may have an aggressive clinical course necessitating systemic therapies (Haematologica 2020;105:348, Blood 2018;131:2877)
- Approximately 33% of cases harbor clonal mitogen activated protein kinase / extracellular signal regulated kinase (MAPK / ERK) pathway alterations (Mod Pathol 2017;30:1367, Haematologica 2020;105:e5)
Terminology
- Initially described by Destombes as adenitis with lipid excess (Bull Soc Pathol Exot Filiales 1965;58:1169)
- Rosai and Dorfman described as sinus histiocytosis with massive lymphadenopathy (Arch Pathol 1969;87:63)
- Classified in the R group (nodal and extranodal disease) and the C group (cutaneous disease only) under the revised classification of histiocytic disorders (Blood 2016;127:2672)
ICD coding
- ICD-10: D76.3 - Rosai-Dorfman disease
Epidemiology
- Mean age at diagnosis: 50 years (range 2 - 79) (Haematologica 2020;105:348)
- F:M = 1.5:1
Sites
- Lymph node involvement common (30 - 50%) (Am J Surg Pathol 2021;45:35, Blood 2018;131:2877)
- Skin is the most common extranodal site (50%)
- Other extranodal sites include bone, upper respiratory tract (sinus), central nervous system including dura and parenchymal lesions, orbit, retroperitoneum (Mayo Clin Proc 2019;94:2054)
Etiology
- Pathogenesis unclear and likely multifactorial
- Association with immune disease suggests that immune dysregulation may play a role in pathogenesis
- Subset harbor MAPK / ERK pathway alterations, suggesting a pathogenesis similar to Langerhans cell histiocytosis and Erdheim-Chester disease (Mod Pathol 2017;30:1367, Cancer Discov 2016;6:154)
Clinical features
- Heterogeneous clinical course, depending on the site of involvement
- Associated conditions include autoimmune disorders (systemic lupus erythematosus, idiopathic juvenile arthritis, autoimmune hemolytic anemia), neoplasia such as lymphomas and myeloid neoplasms and IgG4 related RDD characterized by increased IgG4 positive plasma cells (Blood 2018;131:2877, Haematologica 2020;105:348)
- Classic (nodal) RDD presents as enlarged lymph nodes, most commonly involving bilateral cervical nodes in young males
- Extranodal RDD manifests with diverse clinical presentations (Blood 2018;131:2877)
- Cutaneous lesions present as slow growing, painless nodules, papules or plaques
- Neurologic involvement may present with headache, seizures, motor / sensory abnormalities and gait disturbances
- Orbital involvement may present with exophthalmos or visual disturbance
- Sinus involvement may display nasal congestion or obstruction
- Pulmonary RDD can present with dry cough, dyspnea and may mimic primary lung cancer, interstitial lung disease and other inflammatory / infectious conditions
- Retroperitoneal involvement may present as diffuse infiltration and less commonly a discrete mass with or without hydronephrosis and ureteral obstruction
- Multisystem involvement in approximately 20% cases and prognosis related to the number of extranodal sites
- Rosai-Dorfman disease may be a component of mixed histiocytosis with Langerhans cell histiocytosis or Erdheim-Chester disease (Mod Pathol 2010;23:1616, Haematologica 2020;105:e5)
Diagnosis
- Comprehensive evaluation, including clinical history, physical examination and imaging studies in conjunction with morphologic features
- RDD may be associated with other histiocytic neoplasms, including Langerhans cell histiocytosis and Erdheim-Chester disease, which should be confirmed by biopsy in the setting of atypical clinical manifestations (Mod Pathol 2010;23:1616, Haematologica 2020;105:e5)
Radiology description
- Nodal involvement on PET CT harboring RDD shows increased central intake with a photopenic halo (Mayo Clin Proc 2019;94:2054)
- Extranodal involvement may show the following findings:
- CNS involvement often presents as hyperattenuating meningeal based mass showing contrast enhancement on CT (Asian J Neurosurg 2010;5:19)
- Skeletal RDD lesions are usually lytic and centered in medullary space (Mayo Clin Proc 2019;94:2054)
- Pulmonary involvement may present as cystic change, interstitial lung disease, nodules, focal pulmonary infiltrate or airway disease
- Sinus involvement may present with maxillary wall thickening
- Retroperitoneum involvement may present as renal hilar masses, subcapsular hypodense infiltration or renal cortical hypodense nodules
- CNS involvement often presents as hyperattenuating meningeal based mass showing contrast enhancement on CT (Asian J Neurosurg 2010;5:19)
Radiology images
Images hosted on other servers:

Imaging findings in RDD
Prognostic factors
- Optimal duration of treatment with systemic therapy is individualized, depending on the extent of involvement
- Usually favorable outcomes in cases with nodal and cutaneous involvement
- Subset may demonstrate aggressive clinical course usually associated with multifocal involvement (Haematologica 2020;105:348)
Case reports
- 10 year old boy with polyuria and polydipsia (Front Med (Lausanne) 2020;7:613756)
- 12 year old boy with dyspnea and left sided chest pain presented with interatrial septal mass (J Radiol Case Rep 2012;6:1)
- 29 year old woman with arthralgias in the hands and knees and lytic lesions of the left distal radius (Curr Rheumatol Rep 2017;19:29)
- 41 year old man with paravertebral mass (J Int Med Res 2017;45:875)
- 53 year old man with diminished vision of right eye associated with a palpable mass (J Microsc Ultrastruct 2019;7:50)
- 57 year old woman with progressive vision loss (Head Neck Pathol 2016;10:414)
Treatment
- Management varies, depending on the site of involvement and the presence / absence of symptoms (Blood 2018;131:2877)
- Nodal / cutaneous involvement usually self limited and requires only observation
- Surgical resection may be considered in symptomatic cases with single site of involvement
- Multifocal and refractory cases may require systemic therapy (first line therapy with cladribine, cytarabine, methotrexate or prednisone)
- Targeted therapy with MEK inhibitors is under investigation in those with MAPK / ERK pathway alterations (Haematologica 2020;105:348)
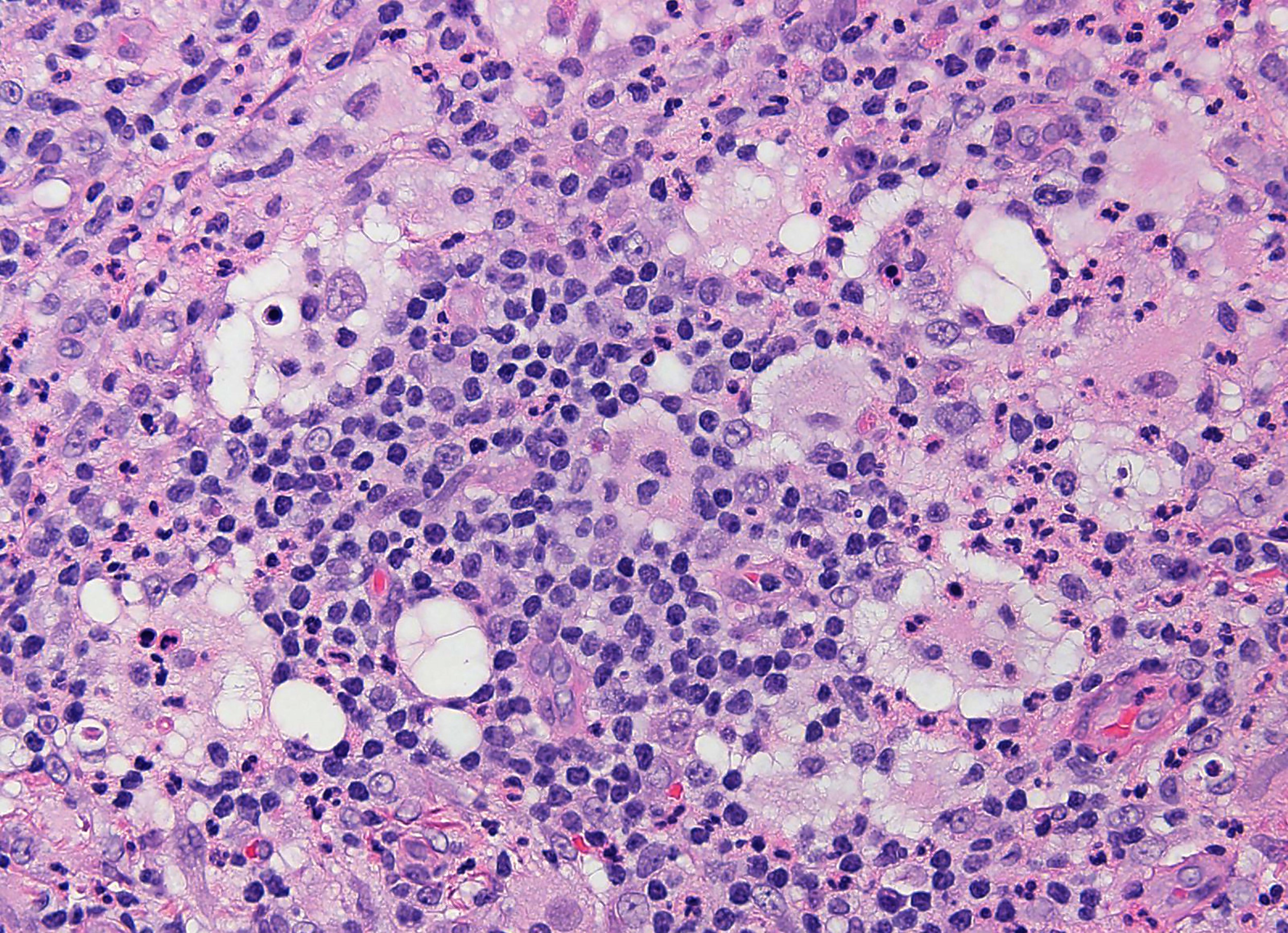
Microscopic (histologic) description
- Characterized by the accumulation of histiocytes with enlarged, round to oval hypochromatic nuclei and abundant eosinophilic cytoplasm, often containing engulfed intact inflammatory cells known as emperipolesis (Am J Surg Pathol 2021;45:35)
- Lesional histiocytes usually associated with fibrosis and prominent inflammatory infiltrate comprised of plasma cells and lymphocytes
- Occasional neutrophilic infiltrates are present
- Nodal involvement is characterized by distended sinuses with lesional histiocytes
- Rosai-Dorfman disease is rarely detected as an incidental finding concomitantly with lymphoma in the same biopsy specimen (Mod Pathol 2019;32:16)
Microscopic (histologic) images
Contributed by Aishwarya Ravindran, M.B.B.S. and Karen L. Rech, M.D.
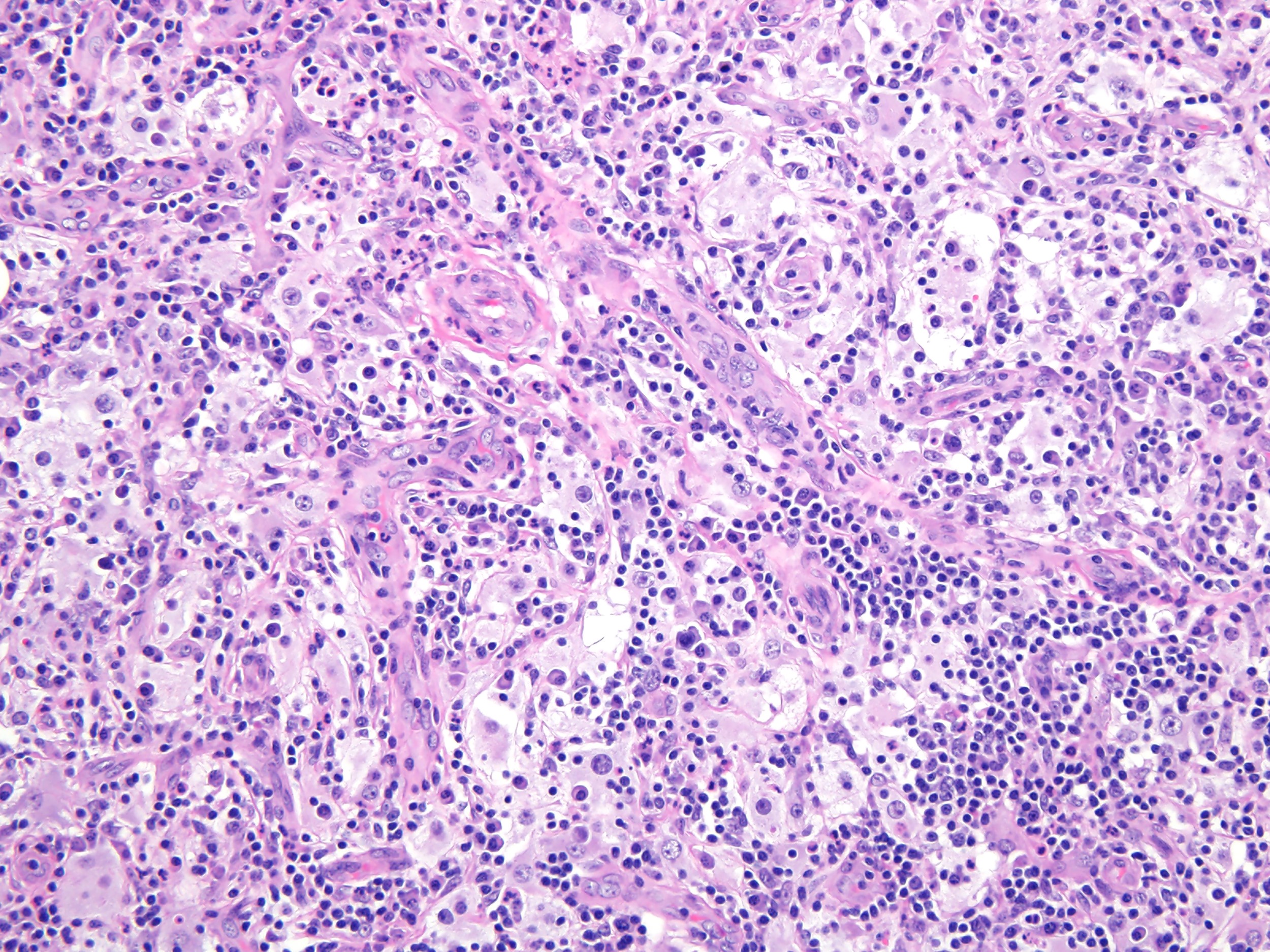
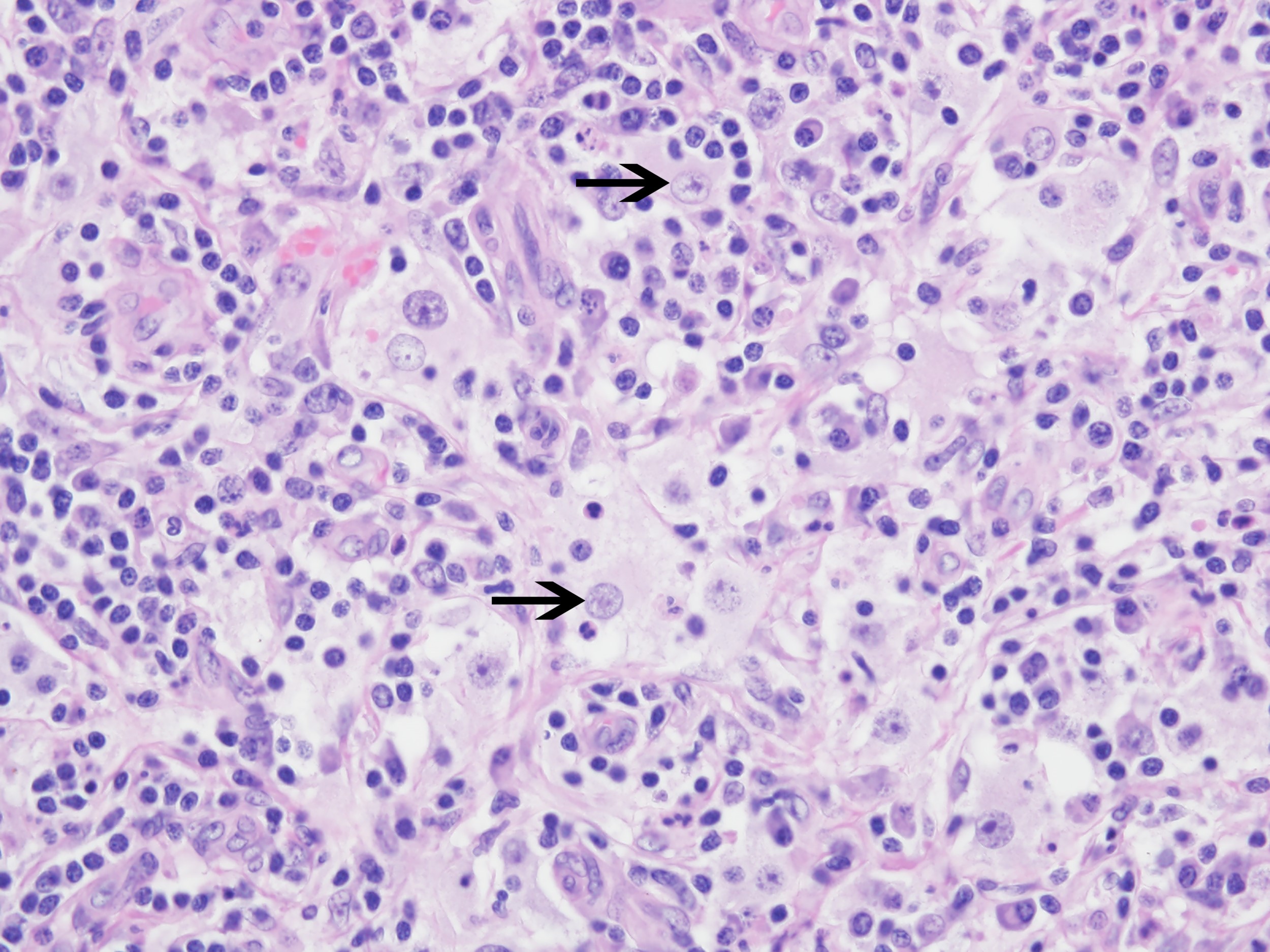
Excisional biopsy of
subcutaneous mass
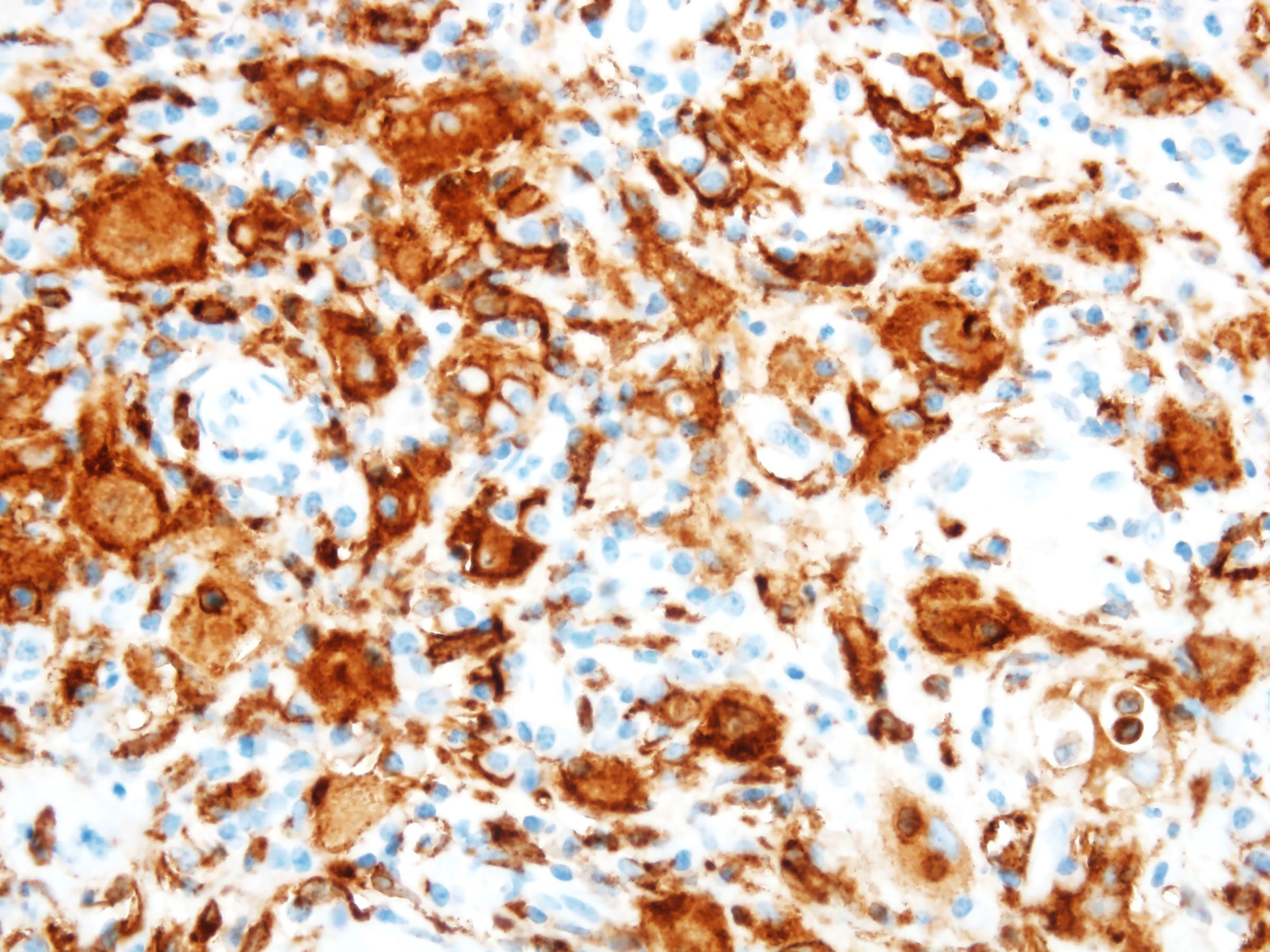
CD163
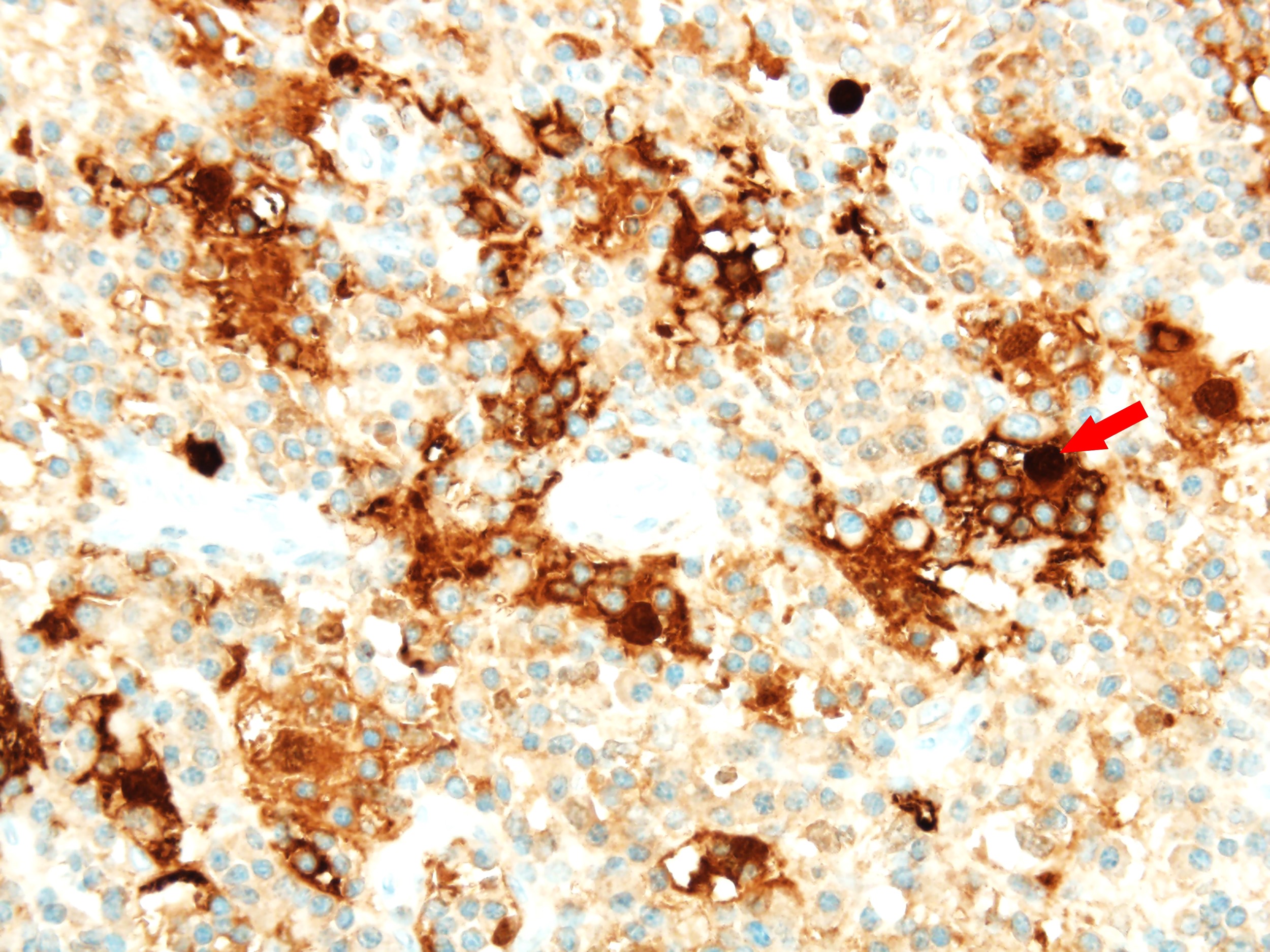
S100
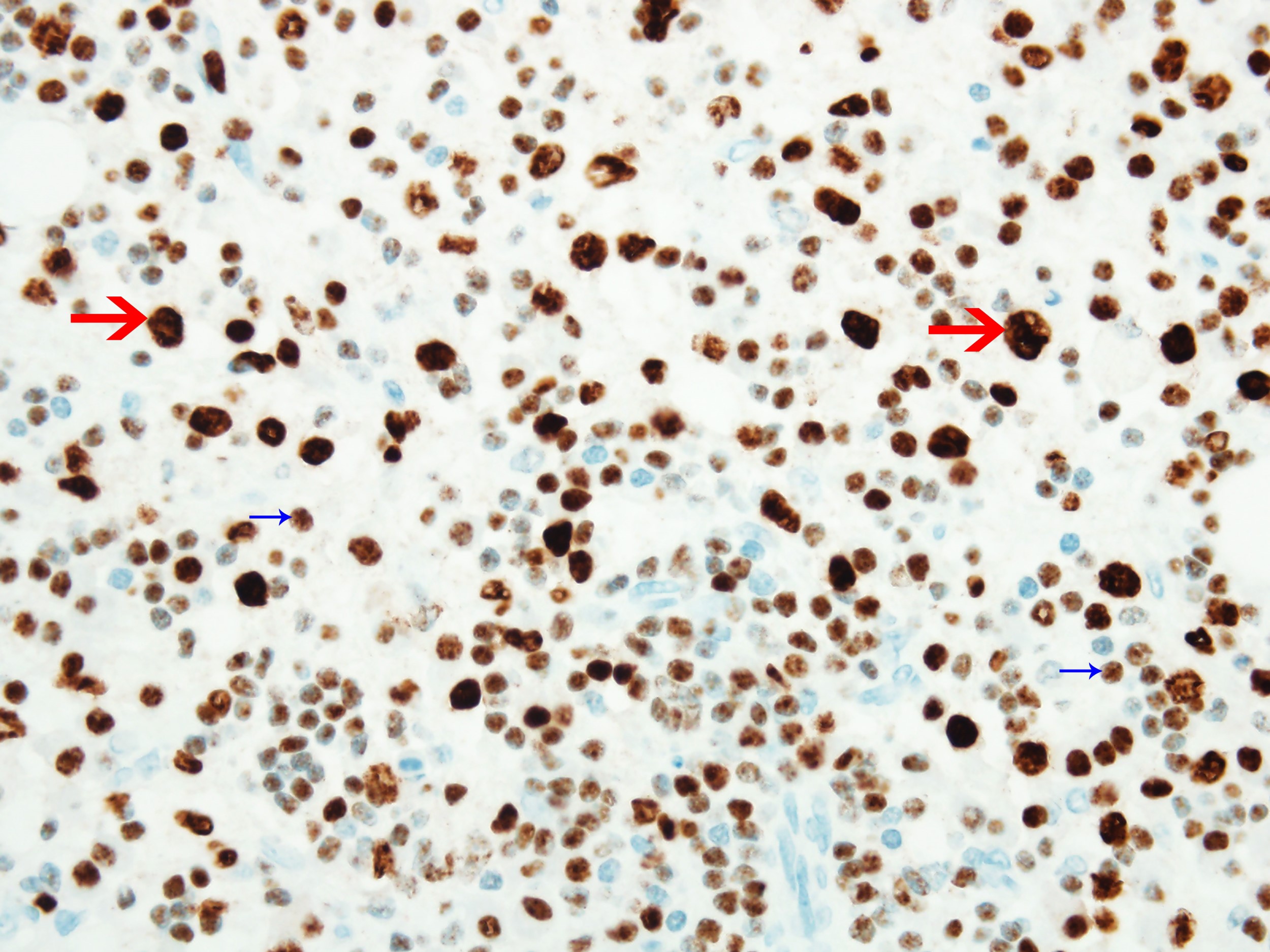
OCT2
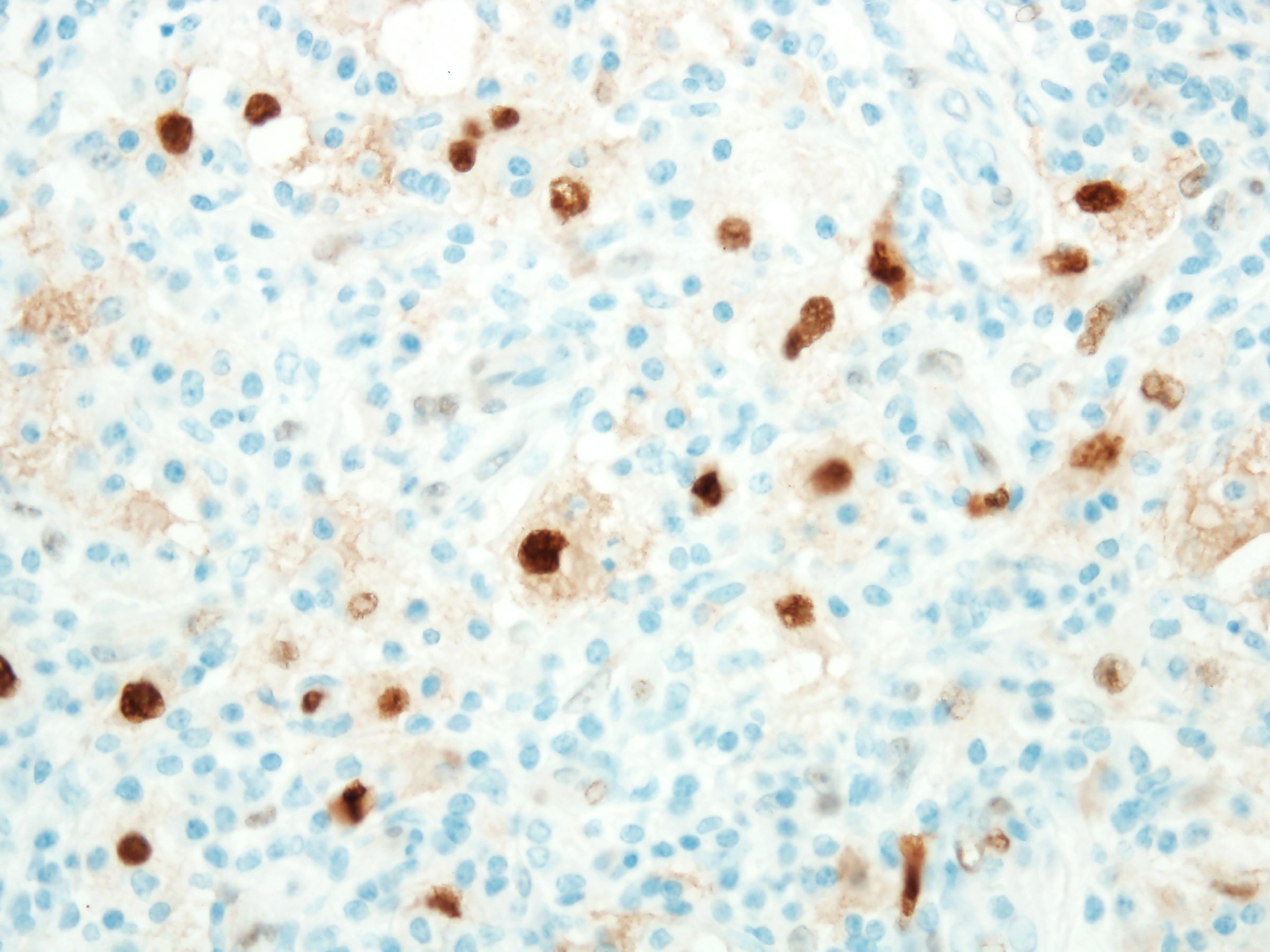
Cyclin D1
Positive stains
- Monocyte / macrophage markers: CD68, CD163, OCT2
- S100, cyclin D1 / BCL1
- Reference: Am J Surg Pathol 2021;45:35
Negative stains
- CD1a, langerin
- BRAF V600E
- Reference: Am J Surg Pathol 2021;45:35
Molecular / cytogenetics description
- Approximately 33% of cases harbor mutually exclusive recurrent KRAS and MAP2K1 mutations (Mod Pathol 2017;30:1367)
- Germline mutations in SLC29A3 gene may be present in familial cases of RDD (Blood 2016;127:2672)
Sample pathology report
- Lymph node, right axillary, excisional biopsy:
- Rosai-Dorfman disease (sinus histiocytosis with massive lymphadenopathy) (see comment)
- Comment: Histologic examination shows distended lymph node sinuses containing a prominent population of histiocytes characterized by large, round nuclei and voluminous cytoplasm showing emperipolesis with engulfment of lymphocytes. The lymphoplasmacytic infiltrate within the lymph node parenchyma is cytologically unremarkable. Immunohistochemistry shows that the atypical histiocytes within the lymph node sinuses are positive for CD68, CD163 with coexpression of S100, OCT2 and cyclin D1. They are negative for BRAF V600E by immunohistochemistry. There is no increase in the number of IgG4 positive plasma cells or an abnormal IgG4/IgG ratio. CD3 and CD20 reveal an appropriate mixture of T cells and B cells, respectively. Kappa and lambda immunoglobulin light chains reveal polytypic plasma cells. CD1a and langerin are negative.
Differential diagnosis
- Sinus histiocytosis:
- Langerhans cell histiocytosis:
- Langerhans cells are characterized by their irregular, grooved, folded or indented nuclei with fine chromatin, inconspicuous nucleoli and abundant pale eosinophilic cytoplasm
- Positive for CD1a and langerin
- Erdheim-Chester disease:
- Bland appearing histiocytes characterized by abundant foamy (xanthomatous) cytoplasm with surrounding fibrosis (Mod Pathol 2018;31:581)
- Touton giant cells are frequently present
- Positive for CD68, CD163, factor XIIIa and negative for OCT2 expression by immunohistochemistry (Am J Surg Pathol 2021;45:35)
- Clinical, radiologic and morphologic correlation required (Mayo Clin Proc 2019;94:2054)
- Juvenile xanthogranuloma:
- Usually in infants and young children
- Histologically and phenotypically similar to Erdheim-Chester disease
- Low grade B cell lymphoma:
Board review style question #1
A 47 year old woman presented with multiple skin nodules on bilateral arms that were gradually increasing in size over 6 months. Based on the morphology, which of the following is the most likely diagnosis?
- Follicular dendritic cell sarcoma
- Juvenile xanthogranuloma
- Langerhans cell histiocytosis
- Reactive process
- Rosai-Dorfman disease
Board review style answer #1
Board review style question #2
Lesional cells in sinus histiocytosis with massive lymphadenopathy show positive expression of which of the following immunostains?
- AE1 / AE3, CAM5.2, CK34βE12
- CD117, DOG1, muscle specific actin
- Cyclin D1, S100 and OCT2
- Desmin, MyoD1, myogenin
- SMA, p63, p40
Board review style answer #2
C. Cyclin D1, S100 and OCT2 (Am J Surg Pathol 2021;45:35)
Comment Here
Reference: Rosai-Dorfman disease (RDD)
Comment Here
Reference: Rosai-Dorfman disease (RDD)
