

Thyroid & parathyroid
Other thyroid malignancies
Thyroid metastases

Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: metastases thyroid gland
- Tumors arising in thyroid by direct extension from adjacent structures or by vascular spread from nonthyroidal sites (Lloyd: WHO Classification of Tumours of Endocrine Organs, 4th Edition, 2017)
- Despite being highly vascularized, the thyroid is a rare site for distant metastases
- The frequency of metastasis in routine practice is < 0.2% of thyroid malignancies (Endocr Pathol 2017;28:112)
- Direct extension common from tumors of larynx, pharynx, trachea, esophagus and neck - usually are squamous cell carcinoma
- FNA is useful for diagnosis of solitary metastases (Cytojournal 2007;4:5)
- More than 1400 cases have been published in series and individual case reports (Endocr Pathol 2013;24:116)
- Tumor to tumor metastasis localized within a primary thyroid neoplasm are very rare with 30+ cases reported
- Thyroid is highly vascularized but secondary metastases to the gland are very uncommon
- Secondary tumors arise from direction extension of head and neck squamous cell carcinoma and distant metastases from kidney, lung, GI and breast
- Tumors preoperatively diagnosed by FNA, cytology, histopathology and immunophenotype are matched with a primary tumor
- Recent series found metastases in up to 0.5% of surgical specimens of thyroid cancer, 0.15% of
thyroidectomies, 0.07% of thyroid FNA and in 0.2% of hospital autopsies (Endocr Pathol 2013;24:116, Clin Endocrinol (Oxf) 2007;66:565, Cytojournal 2017;14:16, Am J Clin Oncol 2015;38:338)
- Old series reported higher prevalence - 0.5% of thyroidectomies and 1.2 - 3% of thyroid malignancies are metastases (Cancer 1997;79:574, Arch Pathol Lab Med 1998;122:37)
- Metastases were found in autopsy of thyroid in up to 25% of patients dying of disseminated malignancies
- Slight predominance in women (1.2:1), mean age over 60 years (Am J Clin Oncol 2015;38:338)
- Direct invasion of thyroid by head neck malignancies
- Squamous cell carcinoma originated from the adjacent organs (larynx, esophagus, hypopharynx and trachea)
- Soft tissue malignancies of the neck
- Parathyroid carcinoma
- Primary sites for distant metastases to thyroid are kidney (34%), lung (15%), gastrointestinal tract (14%) and breast (14%) (Endocr Pathol 2013;24:116)
- Lung cancer is the most common primary for thyroid metastasis in Asian series (Arch Pathol Lab Med 1998;122:37, Endocr Pathol 2015;26:80)
- Infradiaphragmatic primaries are more common than supradiaphragmatic (Endocr Pathol 2017;28:11)
- Renal cell carcinoma is the most common primary in clinical series, while lung cancer is the most common in autopsy studies (Ann Surg Oncol 2017;24:1533)
- Two major hypotheses explain the rarity of metastases in the highly vascularized thyroid (Thyroid 2012;22:258):
- Relatively rapid arterial flow through the thyroid may discourage adhesion and seeding of metastases
- High oxygen saturation and iodine content of the thyroid gland itself may directly inhibit the growth of malignant cells
- Fine needle aspiration after incidental discovery by ultrasound (Ann Surg Oncol 2017;24:1533)
- Accurate morphological diagnosis is facilitated by clinical history
- Discovered at the time of diagnosis of the primary tumor, after preoperative investigation of a neck mass, on histologic examination of a thyroidectomy specimen or at autopsy (Ann Surg Oncol 2017;24:1533)
- Most nodules are asymptomatic
- Solitary metastasis to the thyroid gland may be the initial presentation of malignancy
- Nonspecific symptoms of neck mass and compression, including dysphagia, dysphonia, pain and airway compromise (Otolaryngol Head Neck Surg 2016;155:961)
- When widespread metastatic disease is present, manifestations in the thyroid gland are typically clinically insignificant (Wartofsky: Thyroid Cancer - A Comprehensive Guide to Clinical Management, 3rd Edition, 2016) )
- Metachronous vs. synchronous metastases = 2:1 (Endocr Pathol 2017;28:11)
- Latency (time from diagnosis of primary tumour to detection of thyroid metastasis) is 20 - 24 months (Clin Endocrinol (Oxf) 2007;66:565)
- Metastases from kidney are generally solitary, occurring a mean 9.2 years after nephrectomy; in 36%, metastasis to thyroid was initial presentation of renal cell carcinoma (Cancer 2002;95:1869)
- Solitary hypofunctioning nodule on RAI scan
- Sonographic characteristics are similar to benign and malignant thyroid diseases (J Ultrasound Med 2017;36:69)
Images hosted on other servers:



CT scan


Sonography

PET - CT

Metastatic renal cell carcinoma
- Determined by the underlying primary tumor (site of origin, aggressiveness, extent of metastatic spread), time
interval between initial diagnosis and metastasis, extrathyroidal extent of disease and completeness or
resection (Ann Surg Oncol 2017;24:1533)
- Metachronous / delayed presentation is associated with improved survival duration (Otolaryngol Head Neck Surg 2016;155:961, Endocr Pathol 2015;26:80)
- Overall 5 year survival after detection of thyroid metastasis or postthyroidectomy is 20 - 30%
- Median survival: 20 months
- Patients who undergo thyroid resection: 30 - 39 months
- Without thyroid surgery: 12 - 24 months
- In one study survival was not different from patients diagnosed with the same primary tumours but without thyroid metastases (Clin Endocrinol (Oxf) 2007;66:565)
- Supradiaphragmatic primaries
- 37 year old woman with metastatic breast carcinoma (Arch Pathol Lab Med 2004;128:804)
- 50 year old woman with severe thyrotoxicosis induced by thyroid metastasis of lung adenocarcinoma (Thyroid 2001;11:883)
- 54 year old woman with intrathyroidal metastasis of breast carcinoma (Int J Surg Pathol 2017;25:319)
- 59 year old man with thyroid metastasis from pulmonary adenocarcinoma (BMC Res Notes 2017;10:130)
- 61 year old man with a solitary thyroid metastasis of nasopharyngeal carcinoma (Indian J Palliat Care 2017;23:104)
- 64 year old man with a metachronous solitary metastasis to the thyroid gland from squamous cell carcinoma of the lung (Tumori 2017;103:e12)
- 85 year old woman with thyroid metastasis of malignant melanoma of the nasal mucosa (Arch Endocrinol Metab 2017;61:193)
- Infradiaphragmatic primaries
- 28 year old woman with thyroid metastasis as initial presentation of cervical carcinoma (Indian J Pathol Microbiol 2017;60:298)
- 42 year old woman with a colon cancer metastasis to the thyroid gland (Clin Case Rep 2016;4:549)
- 50 year old woman with metastasis of tibial osteosarcoma to the thyroid gland (JAMA Oncol 2017;3:853)
- 51 year old Caucasian woman with metastases of renal cell carcinoma (Case Rep Oncol Med 2013;2013:485025)
- 54 year old woman with 2 thyroid nodules-uterine leiomyosarcoma (Case of the Week #342)
- 54 year old woman with metastatic endometrial carcinosarcoma (Gynecol Endocrinol 2007;23:562)
- 54 year old man with metastatic hepatocellular carcinoma (World J Surg Oncol 2007;5:144)
- 54 year old man with multinodular goiter as initial presentation of renal cell carcinoma (BMC Endocr Disord 2006;6:6)
- 55 year old woman with metastatic ovarian carcinoma (Gynecol Oncol 2006;102:394)
- 56 year old woman with thyroid metastasis from cancer of the uterine cervix (Acta Medica (Hradec Kralove) 2016;59:97)
- 64 year old woman with colon cancer metastatic to the thyroid gland (Int J Surg Case Rep 2017;37:221)
- 64 year old man with thyroid metastasis of prostate adenocarcinoma (J Clin Diagn Res 2017;11:ED19)
- 65 year old man with renal cell carcinoma metastic to thyroid (Univ Pittsburgh: Case #454 [Accessed 16 October 2017])
- 67 year old man presented with a thyroid mass (Case of the Week #461)
- 71 year old woman with intrathyroidal metastasis of renal clear cell carcinoma in goiter (Thyroid Res 2008;1:6)
- Tumor to tumor metastases
- 52 year old man with rectal carcinoma metastatic to poorly differentiated thyroid carcinoma (World J Surg Oncol 2008;6:122)
- 55 year old man with small cell carcinoma of lung metastasizing to follicular adenoma of thyroid (Indian J Pathol Microbiol 2017;60:133)
- 65 year old man with poorly differentiated carcinoma of lung metastatic to follicular adenoma (Patholog Res Int 2011;2011:238693)
- Two cases of prostatic and breast carcinoma metastasizing to follicular adenoma (Arch Pathol Lab Med 1994;118:551)
- Three patients with tumor to tumor metastases to follicular variant of papillary thyroid carcinoma (Arch Pathol Lab Med 1999;123:703)
- Patient with history of melanoma presented with a thyroid nodule and had a total thyroidectomy (Case of the Month #513)
- Surgical resection (total or subtotal thyroidectomy) if patient presents with an isolated metastasis diagnosed during followup of indolent disease (Thyroid 2007;17:49)
- For patients with widespread metastases in the setting of an aggressive malignancy, surgery is rarely indicated (Ann Surg Oncol 2017;24:1533)
- Single, more often than multiple, diffuse or bilateral (Arch Pathol Lab Med 1998;122:37)
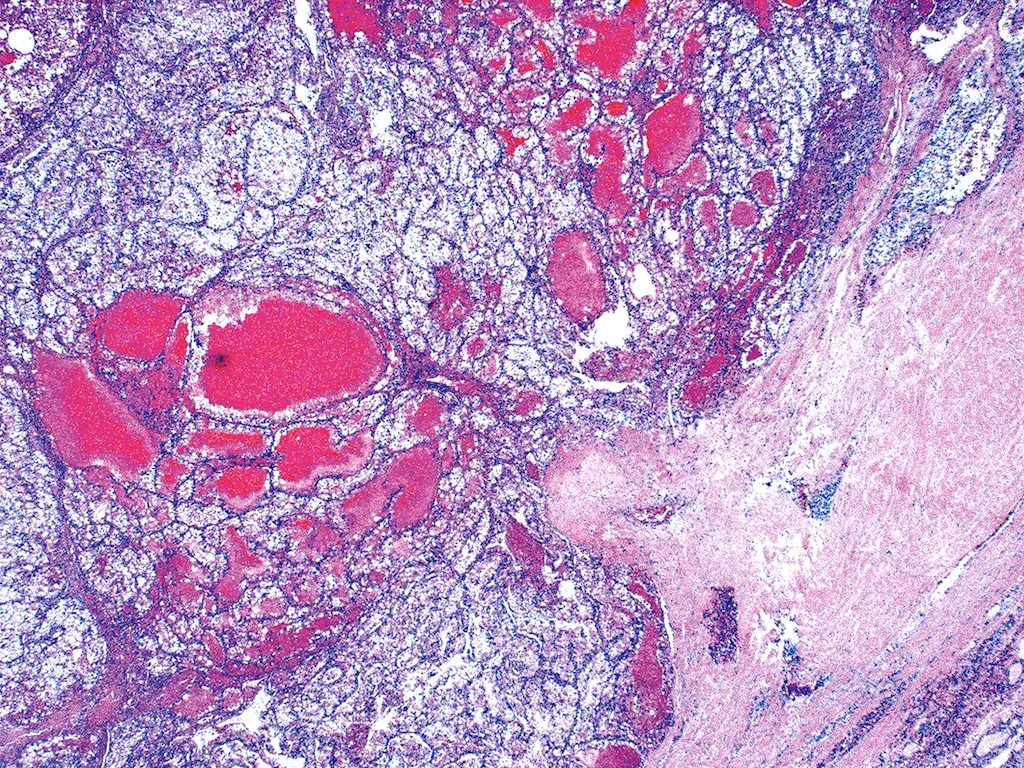
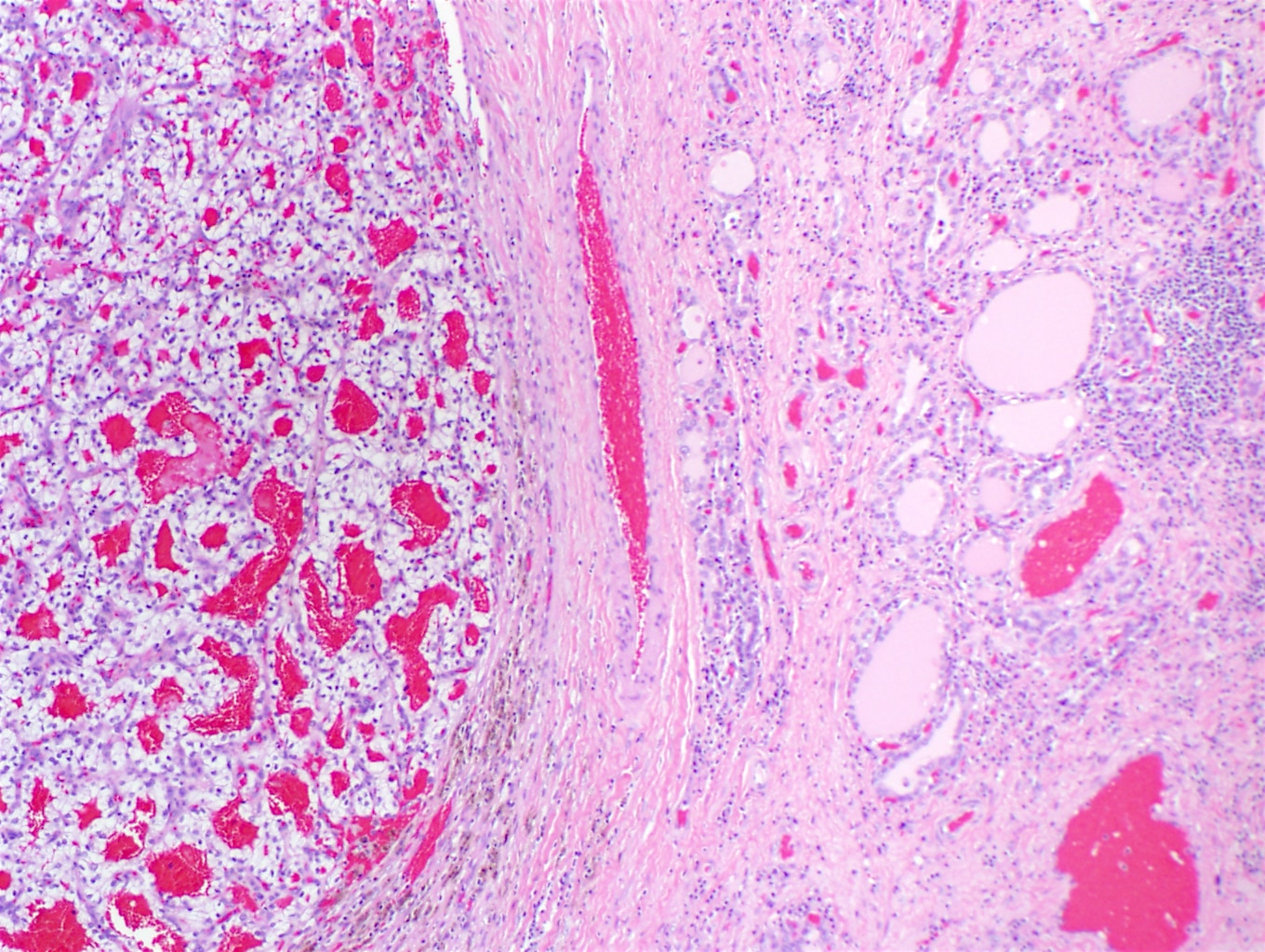
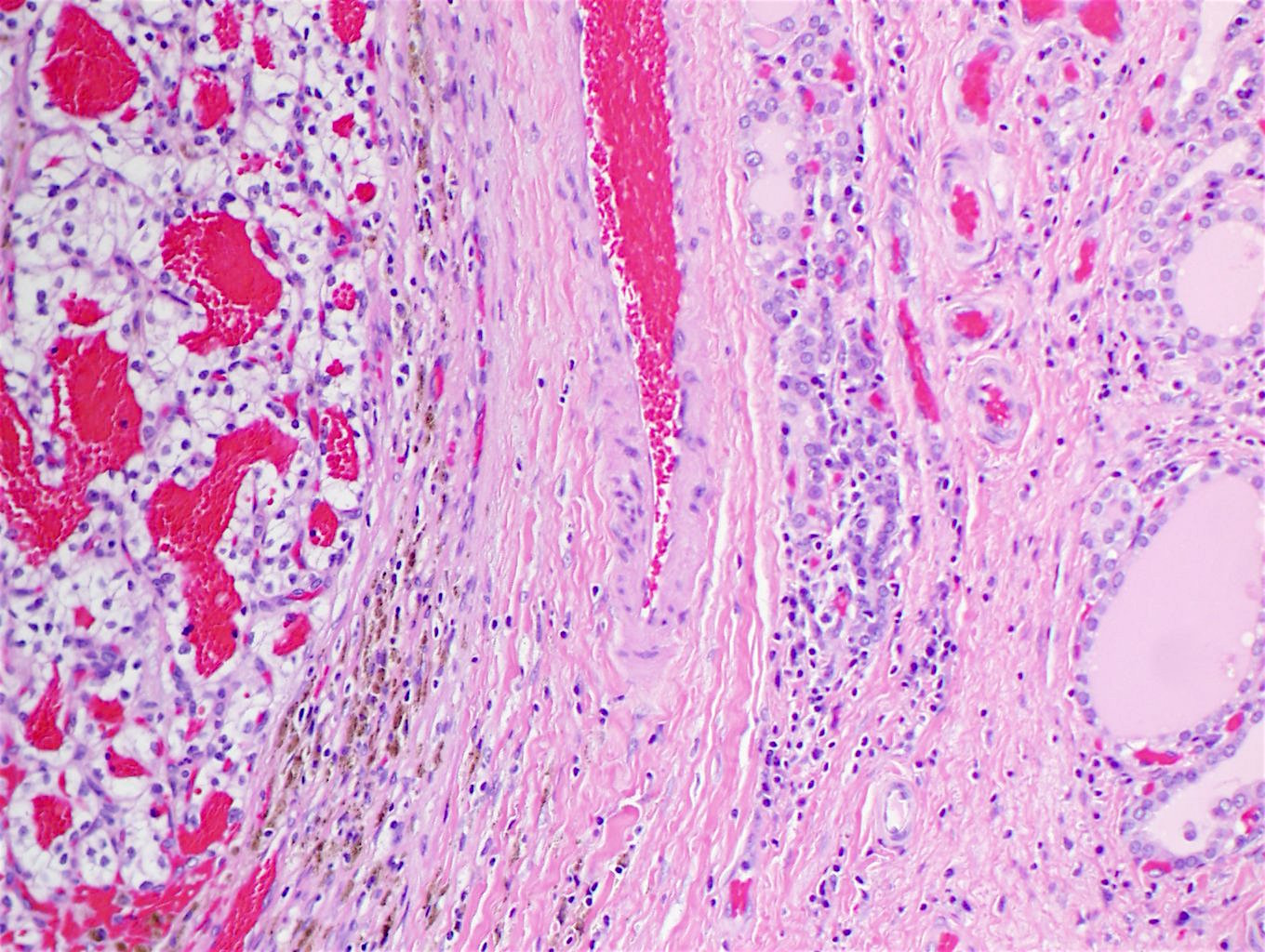
- Gross features consistent with the primary tumour (e.g., yellow, hemorrhagic appearance of a renal cell primary or mucin pools of a gastrointestinal primary) may be helpful to suspect metastasis (Lloyd: WHO Classification of Tumours of Endocrine Organs, 4th Edition, 2017)
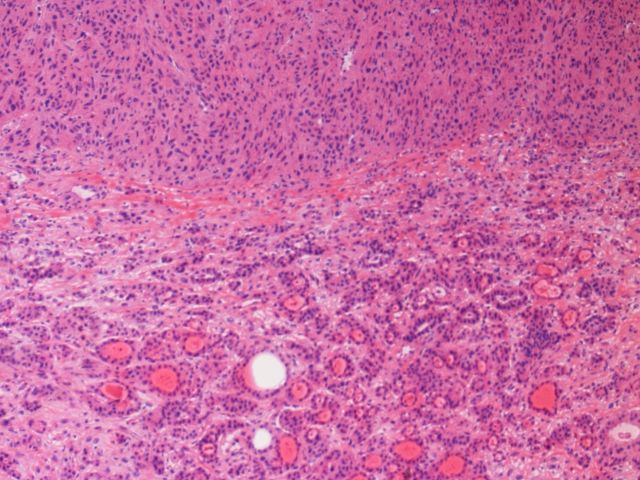
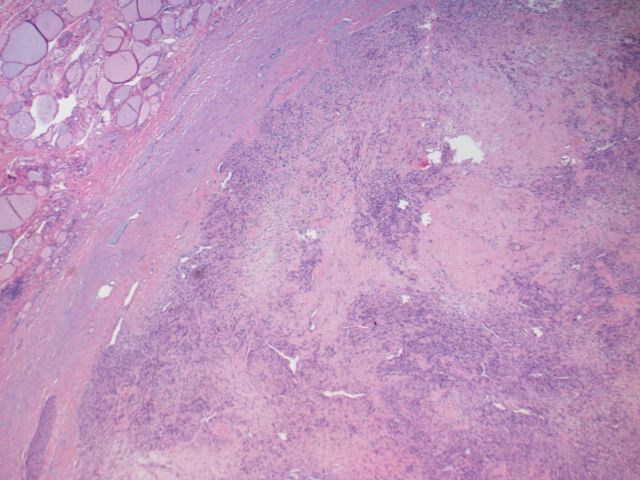
- If primary arises from an adjacent structure, direct invasion is generally clear
- Multinodular metastasis may be indistinguishable from a nodular goiter (Ann Surg Oncol 2014;21:434)
Contributed by Mark R. Wick, M.D., Jose G. Mantilla, M.D. (Case #513) and AFIP

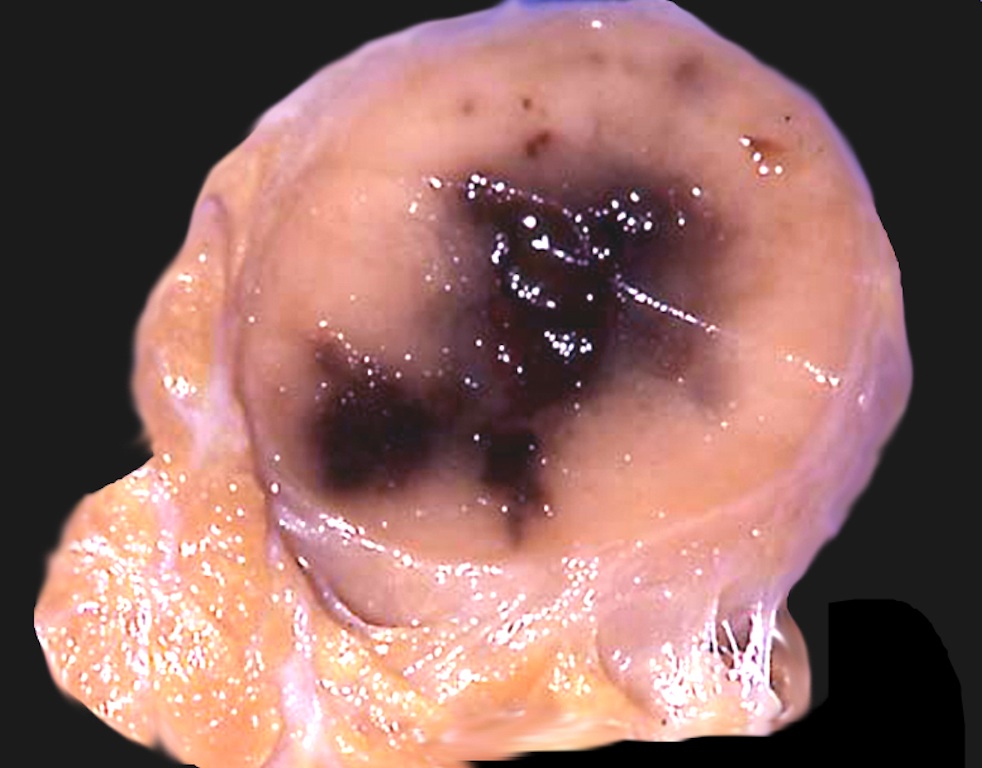
Metastatic renal cell carcinoma

Melanoma in OFA
Melanoma metastatic from skin primary
Images hosted on other servers:

Invasion by squamous cell carcinoma of larynx

Renal papillary carcinoma

Metastatic renal cell carcinoma



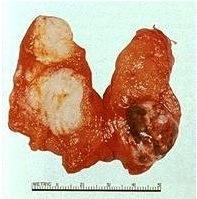
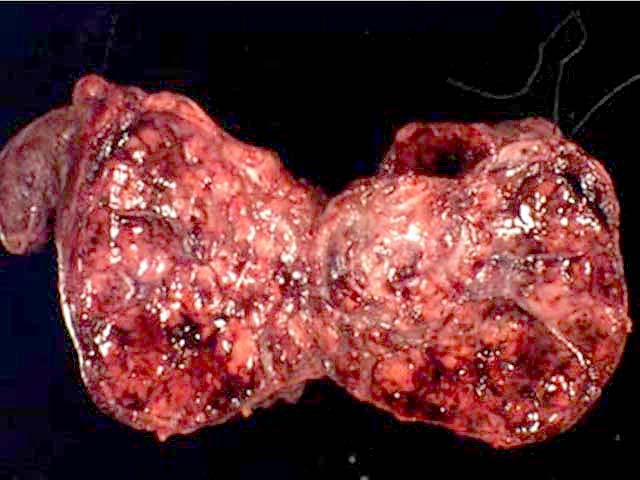
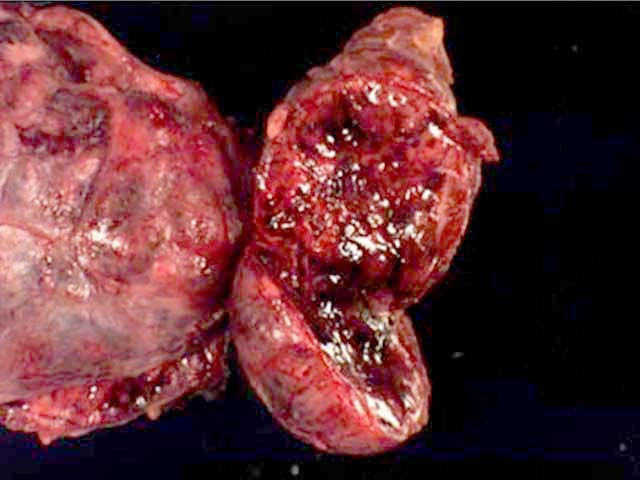
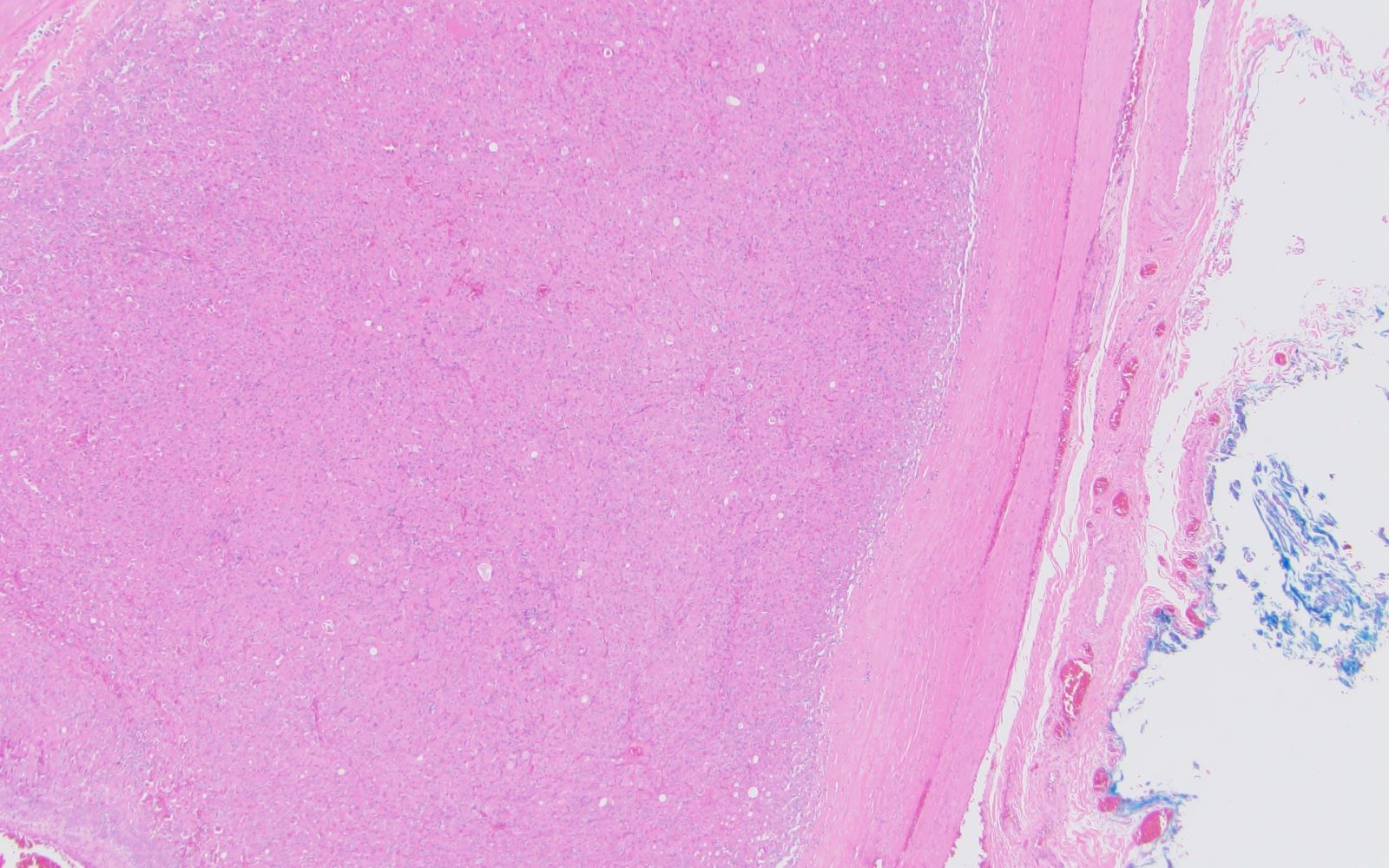
Surgical specimens

Surgical specimens
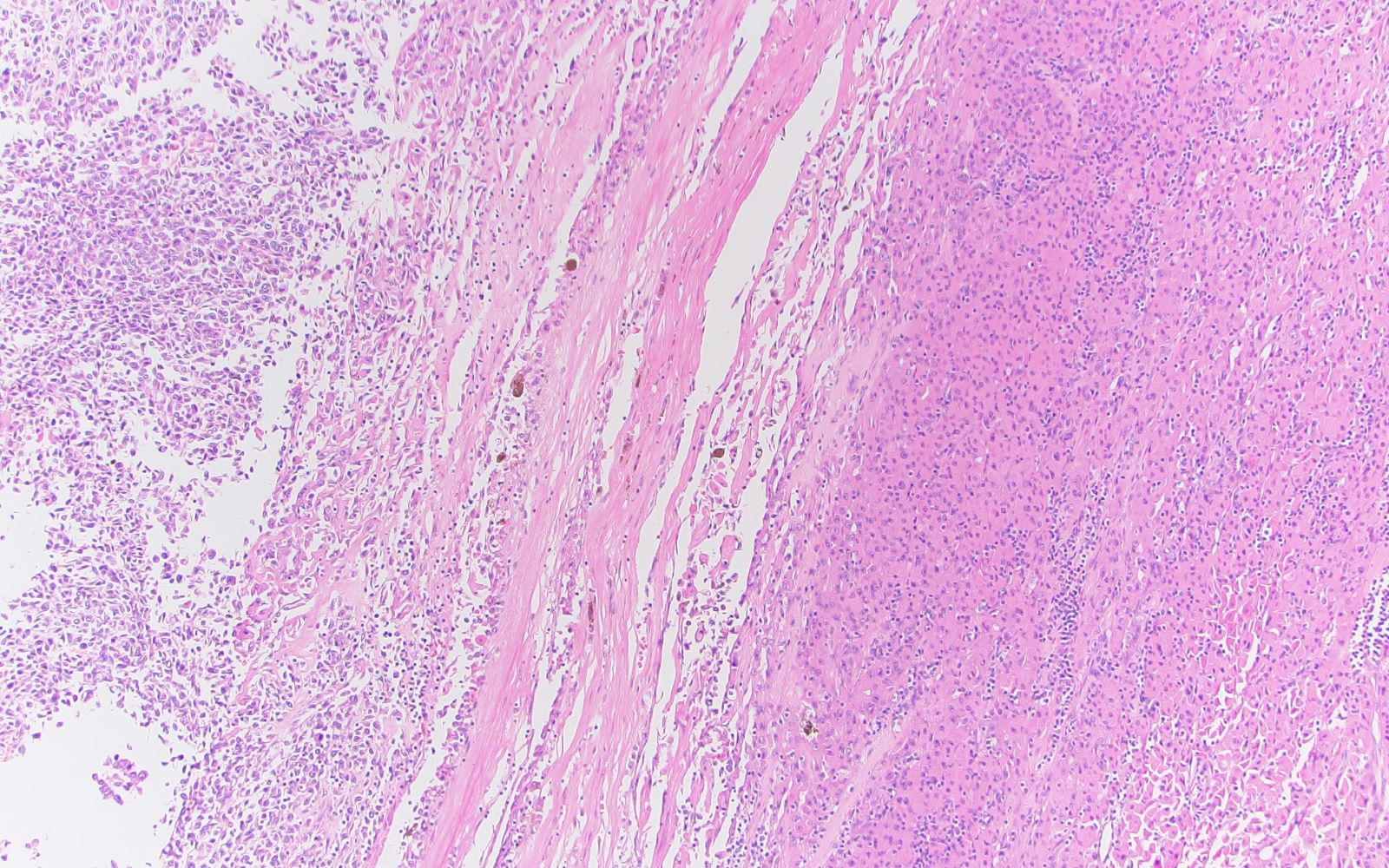
- May involve multiple areas of thyroid gland
- Can be small deposits within lymphovascular spaces or large mass
- Often moderate or poorly differentiated adenocarcinoma (Arch Pathol Lab Med 1998;122:37)
- Tumor to tumor metastasis appears as thyroid neoplasm (usually follicular adenoma) containing a nodule with contrasting morphology
Scroll to see all images:
Contributed by Mark R. Wick, M.D.
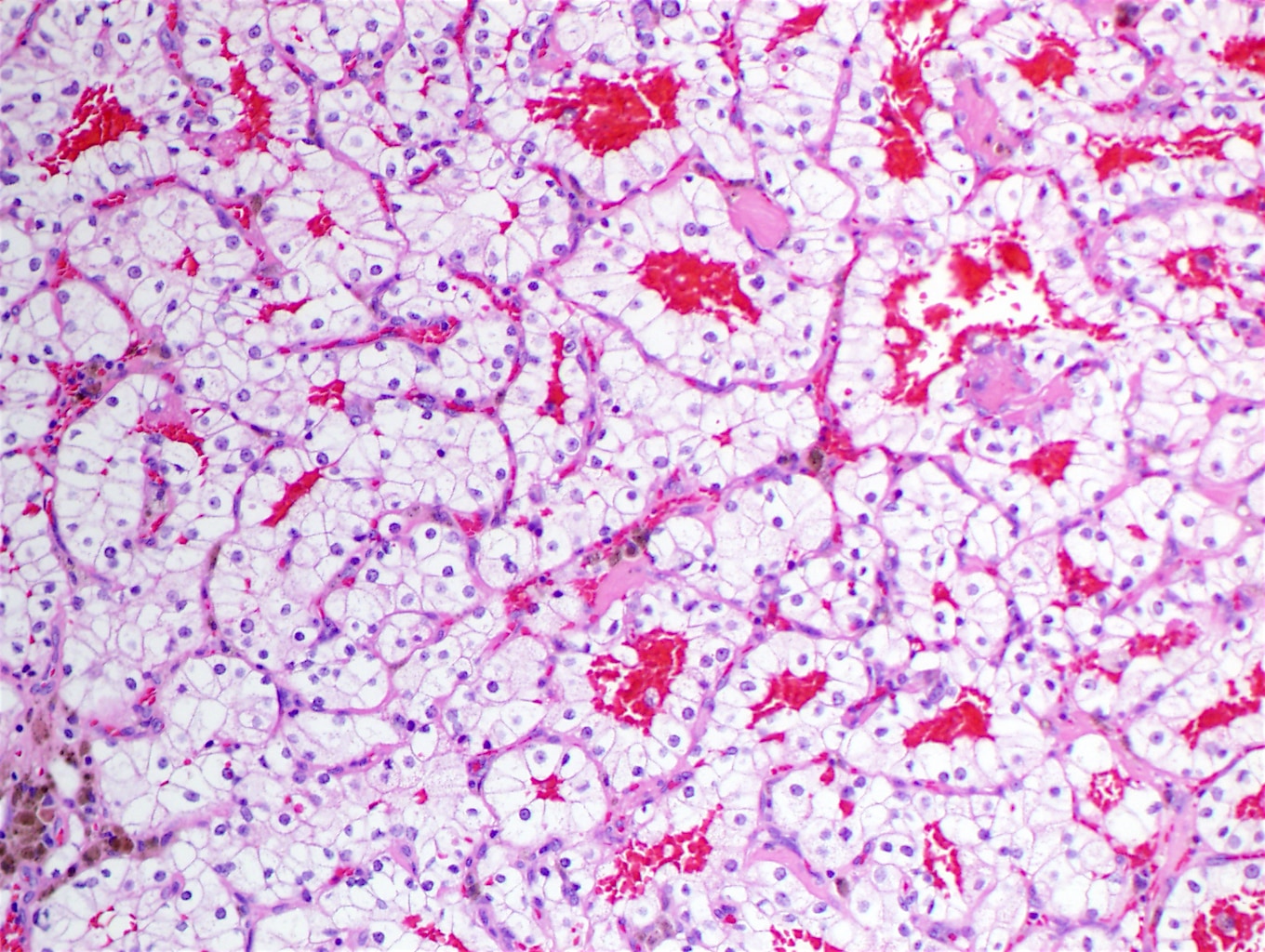
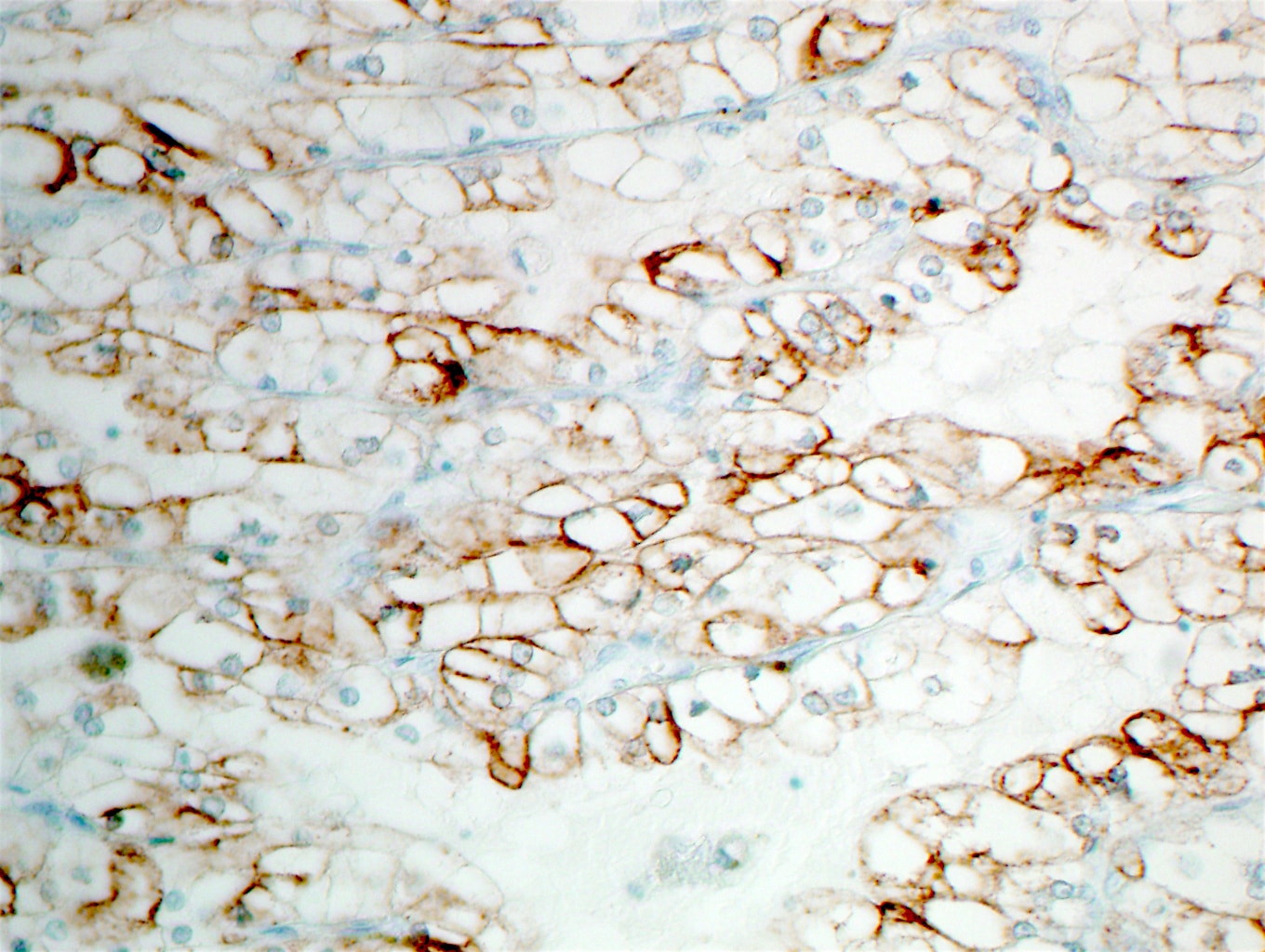
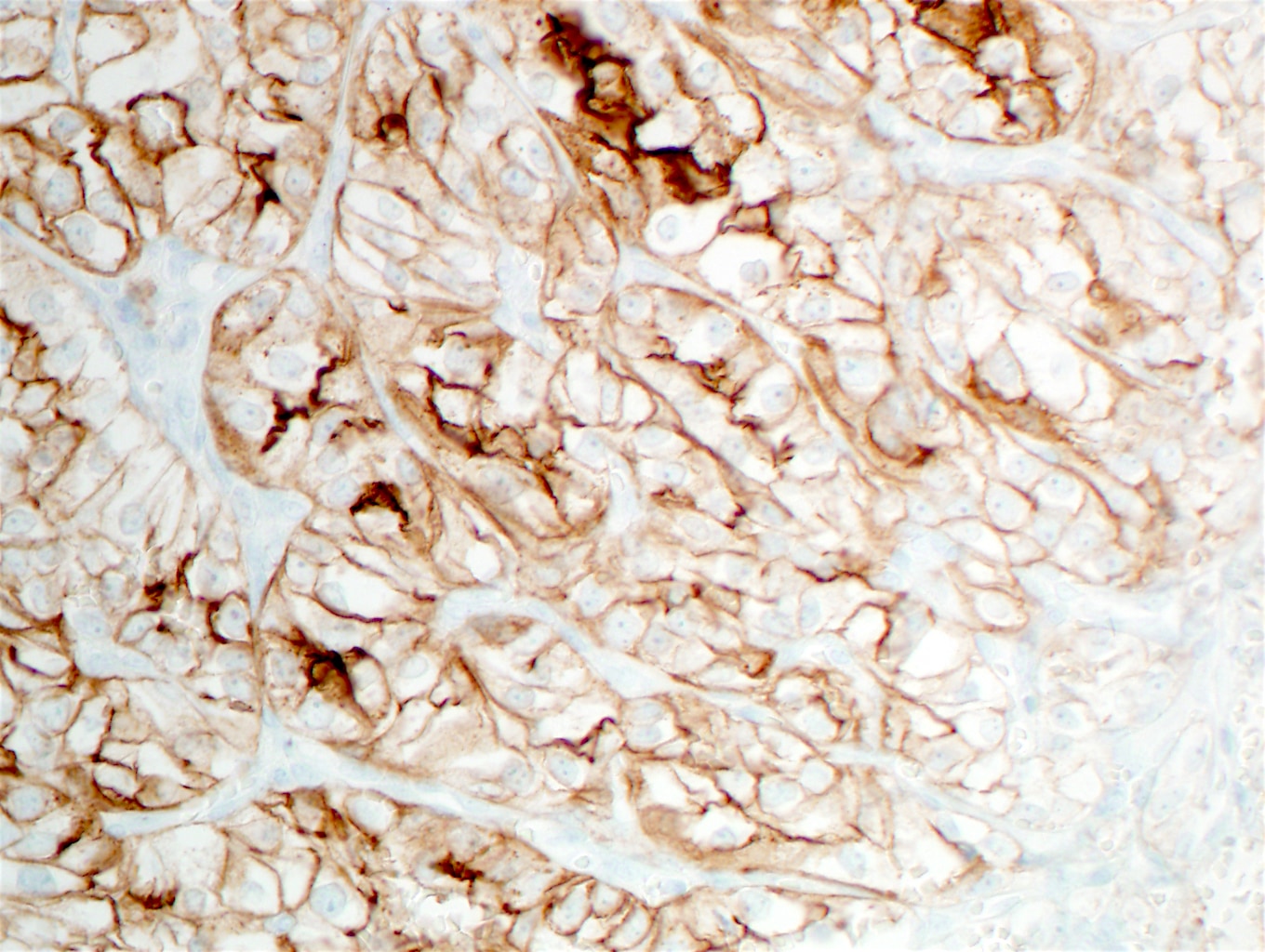
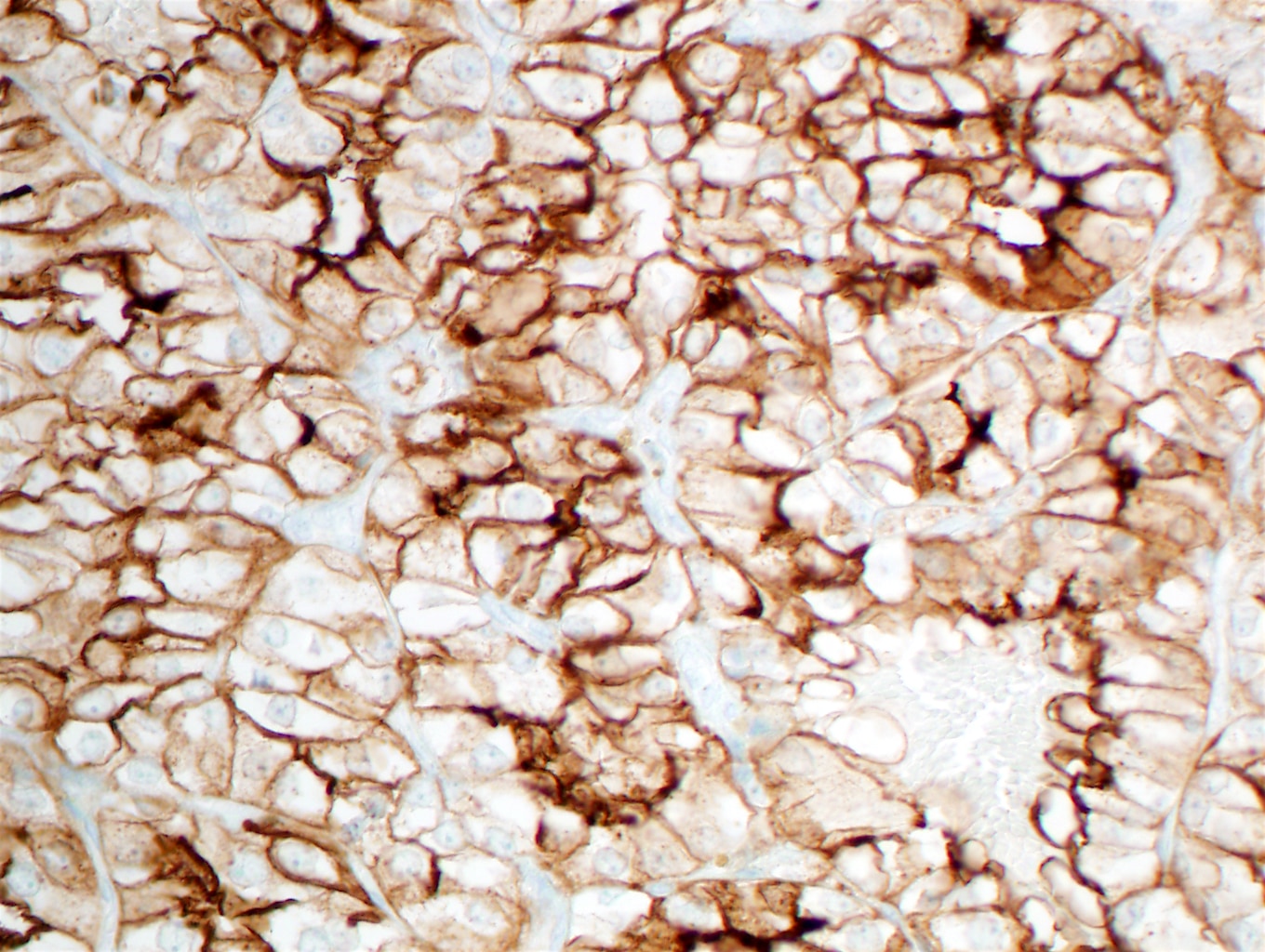
Metastatic renal cell carcinoma
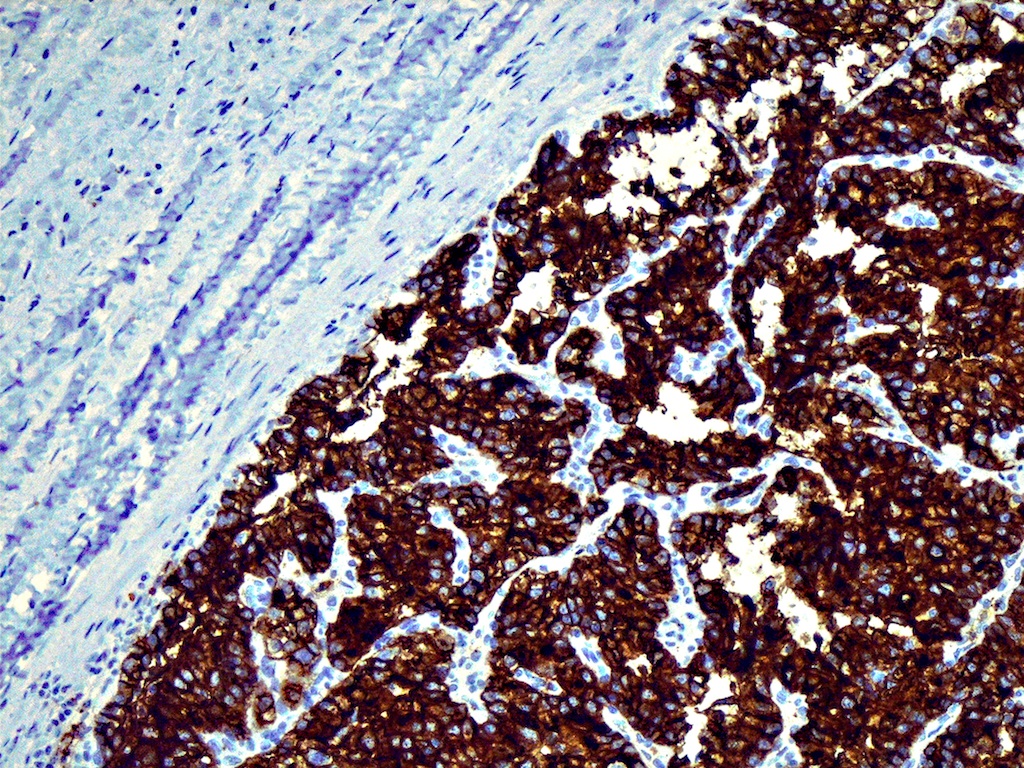

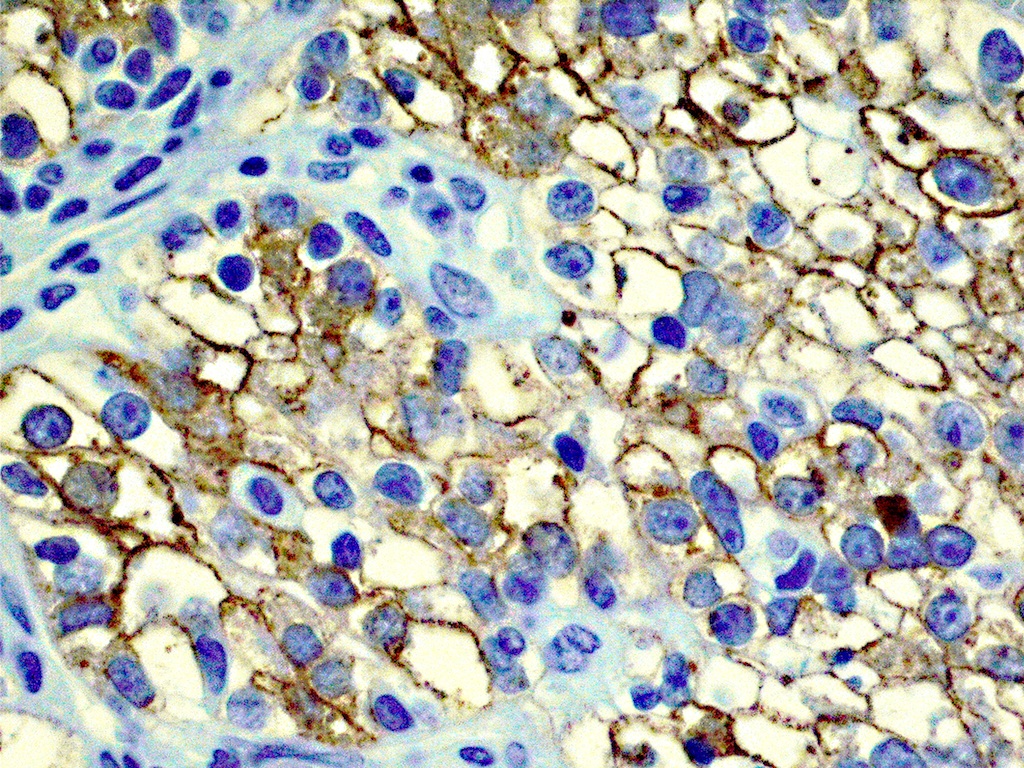
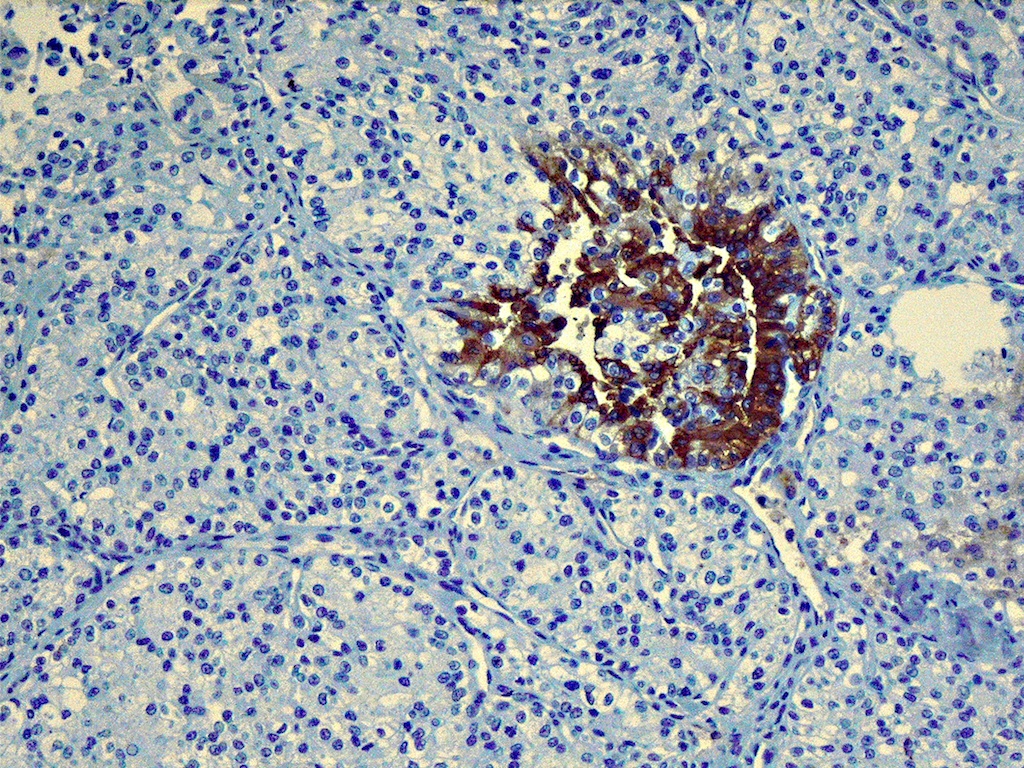
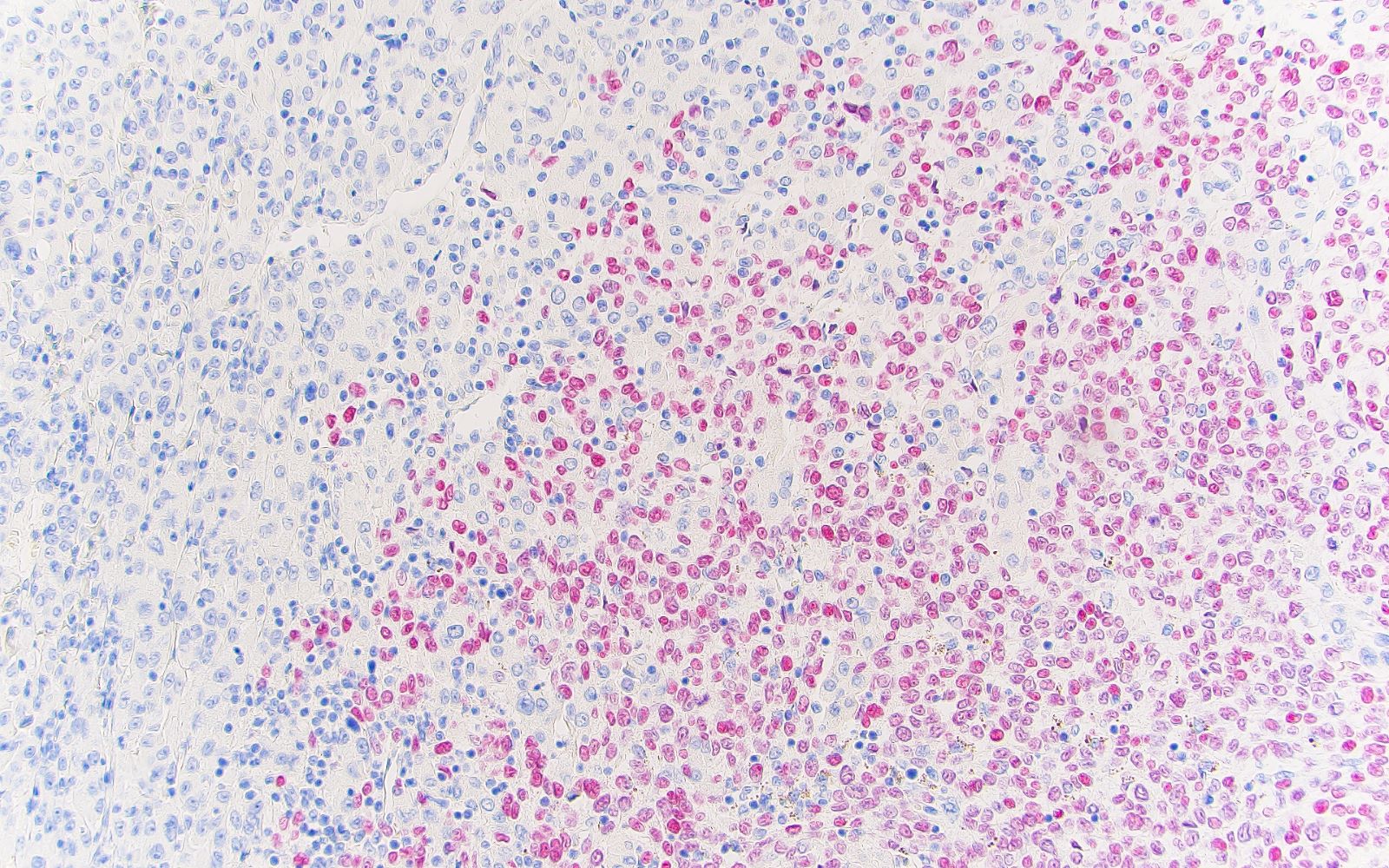
CD10, Keratin 8, RCC, thyroglobulin
Contributed by Jose G. Mantilla, M.D. (Case #513)
HCA capsule
Interface between components

Pigmented component
Hürthle cell component
Melanoma in OFA interface
Melanoma in OFA SOX10
Case #461


Clear cell RCC metastatic to the thyroid
CD10, 400x
RCC, 400x
Case #342
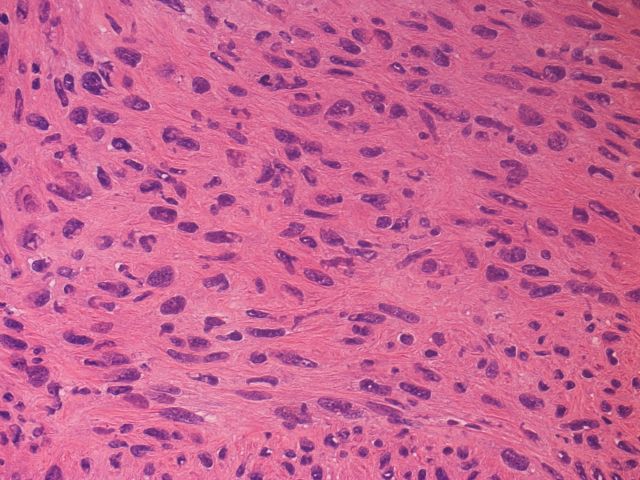
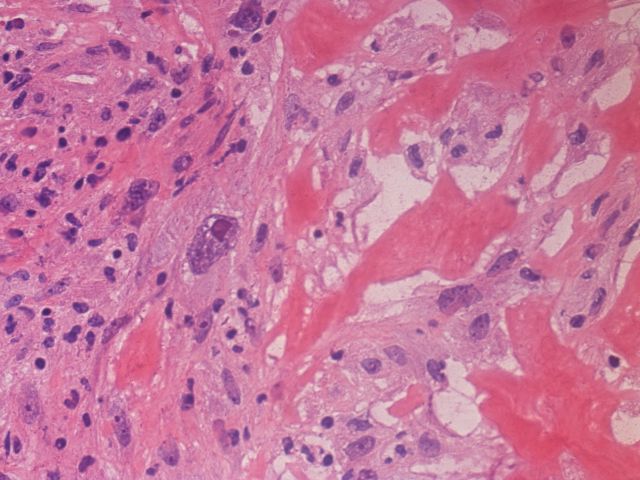
Metastatic leiomyosarcoma (frozen section slides)
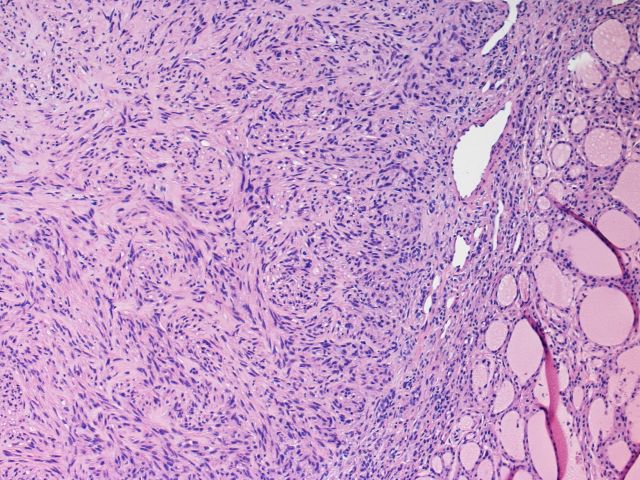
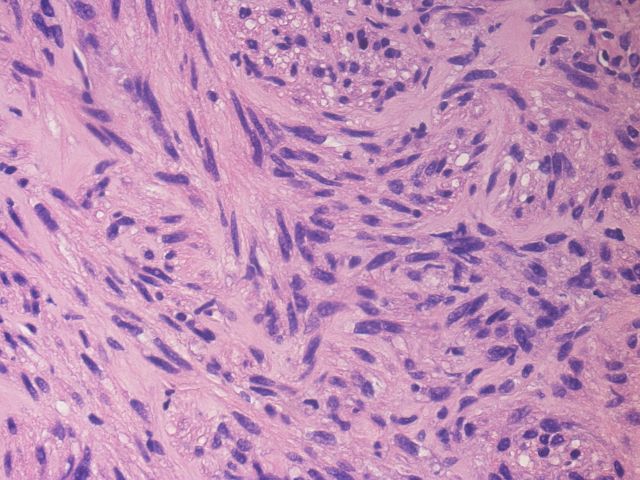

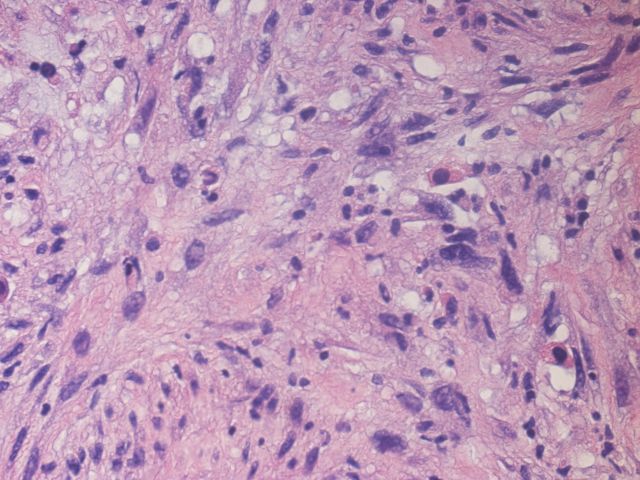
Metastatic leiomyosarcoma (permanent sections)
AFIP images

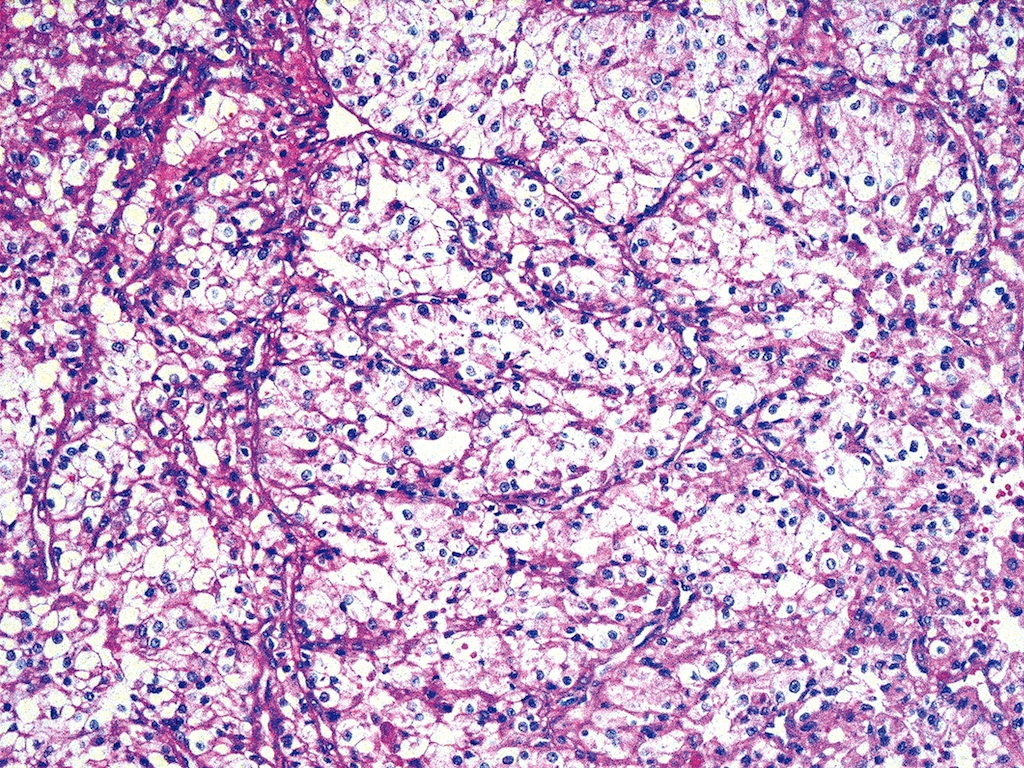
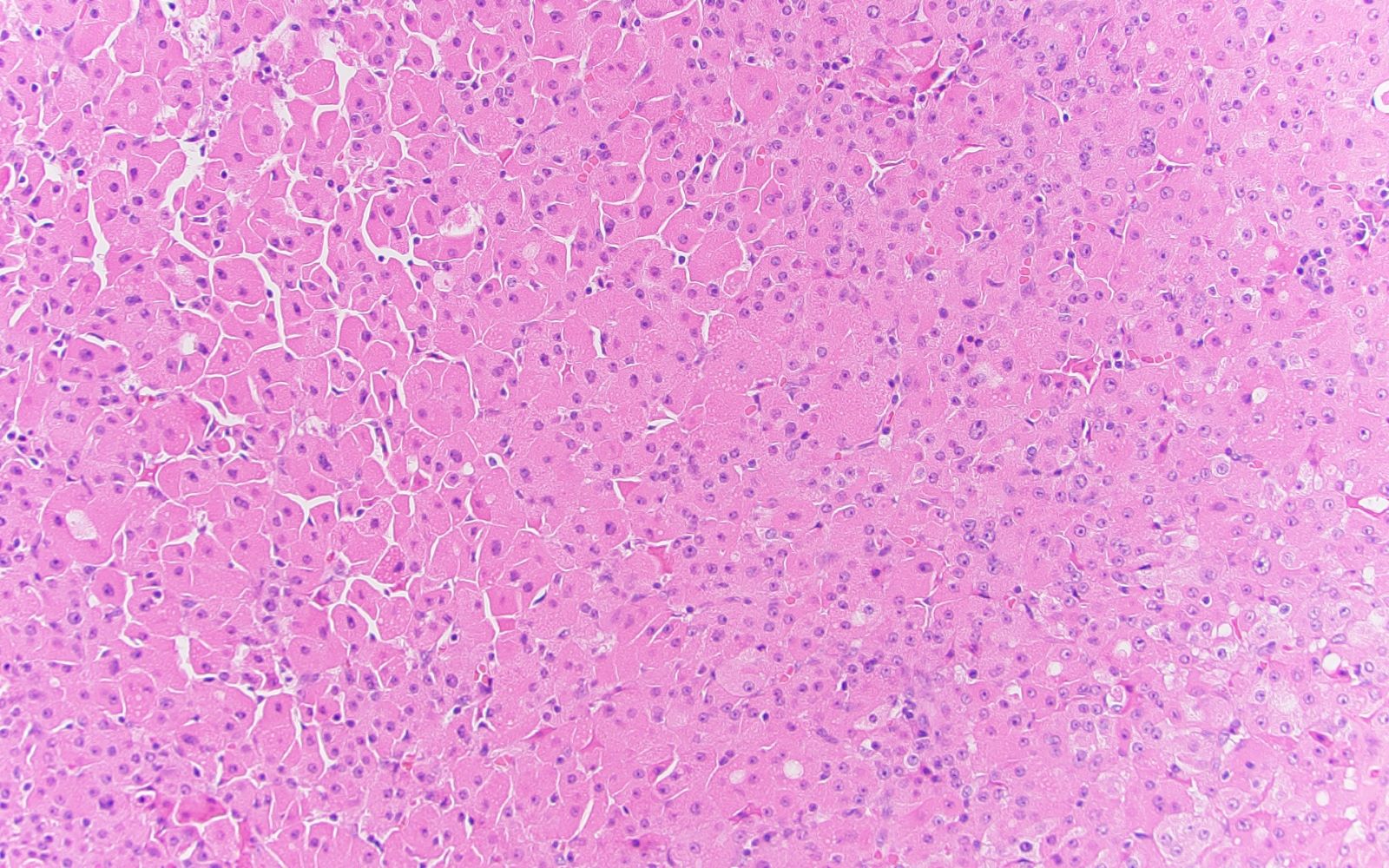
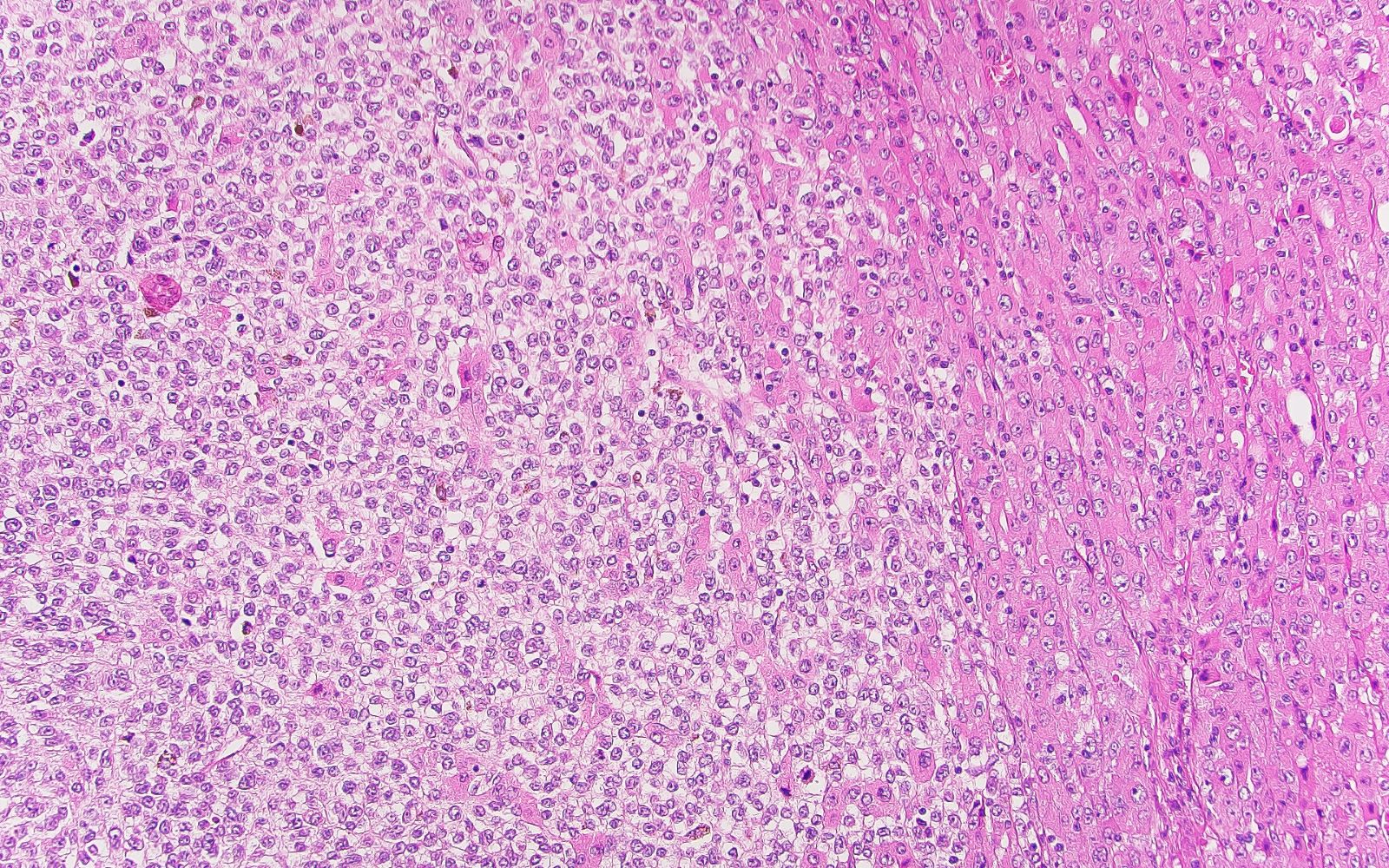
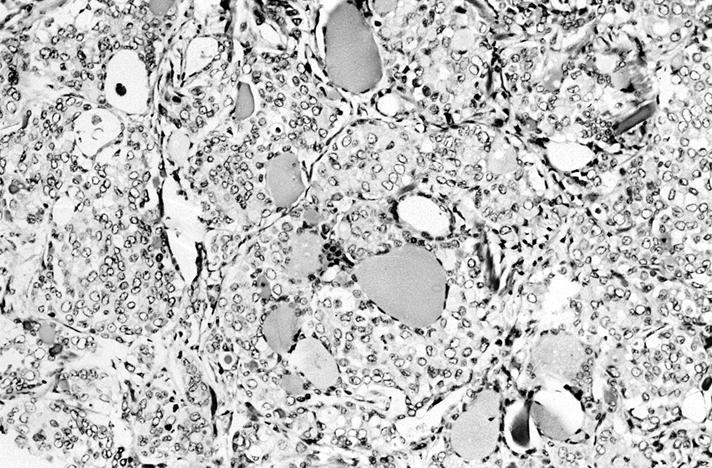
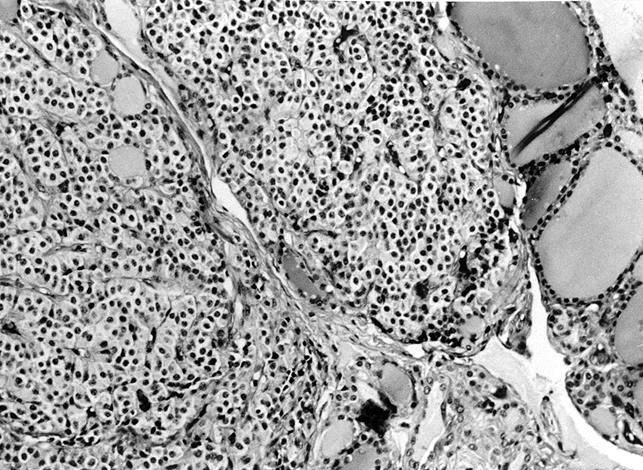
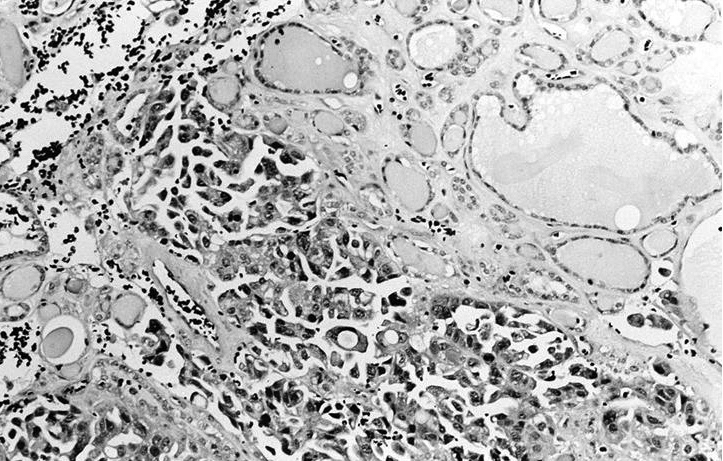
Clear cell type

Cytoplasm is abundant and completely clear
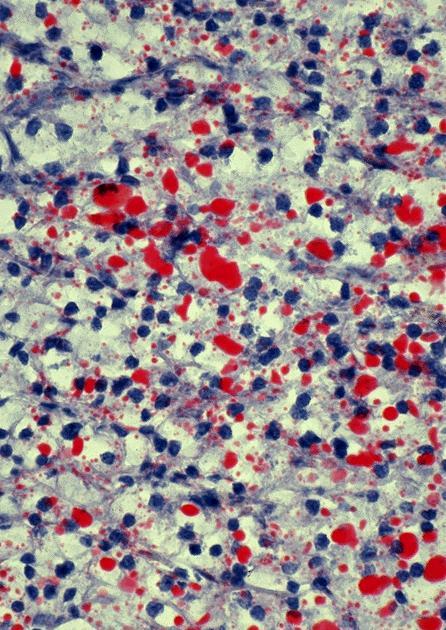
Oil Red O stains cytoplasm strongly
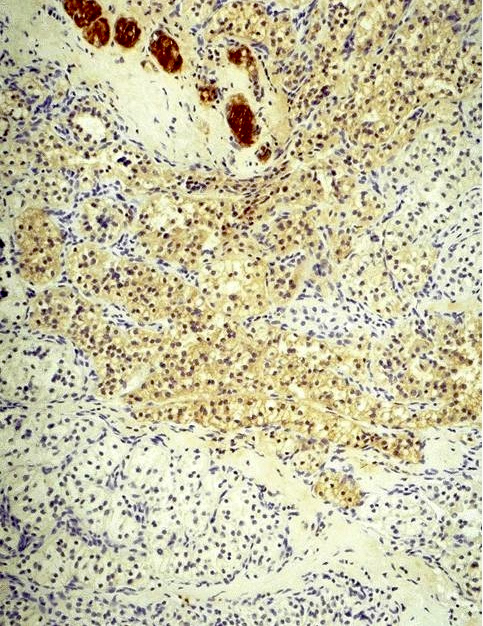
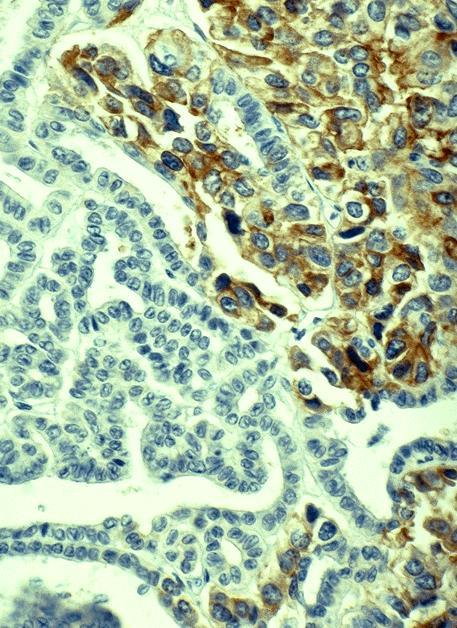
False positive thyroglobulin staining
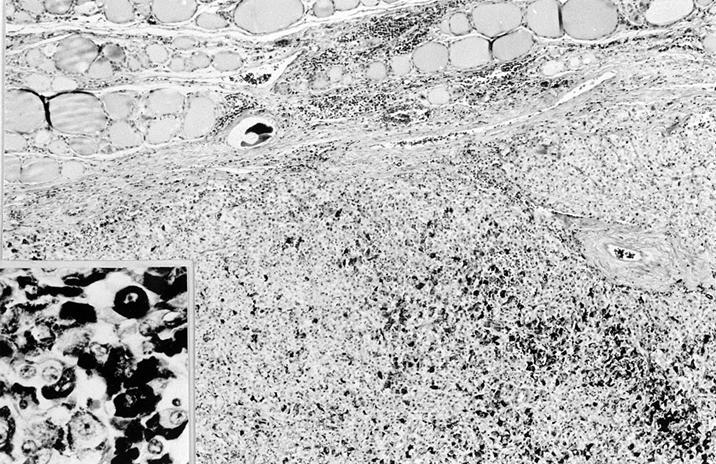
Breast carcinoma:
Lobular carcinoma and entrapped thyroid follicles
ER stains breast tumor but not papillary carcinoma

Falsely positive thyroglobulin staining
Lung:
Carcinoid tumor with well defined nesting pattern
Carcinoma metastatic to mediastinal thyroid gland
Skin:
Melanoma
Images hosted on other servers:

From rectum

Metastatic HCC in the thyroid gland

HCC stains for AFP


Clear cell type

Metastasis to goiter

Concurrent RCC and thyroid carcinoma

Central lesions inside
hyperplastic adenomatoid
nodules

FNA, histology and stains

CD10 and H&E

Tumor to tumor metastases


Lung-small cell carcinoma

Lung-squamous cell carcinoma

Melanoma

Parotid adenoid cystic carcinoma

Rectal carcinoma
to poorly
differentiated
thyroid carcinoma
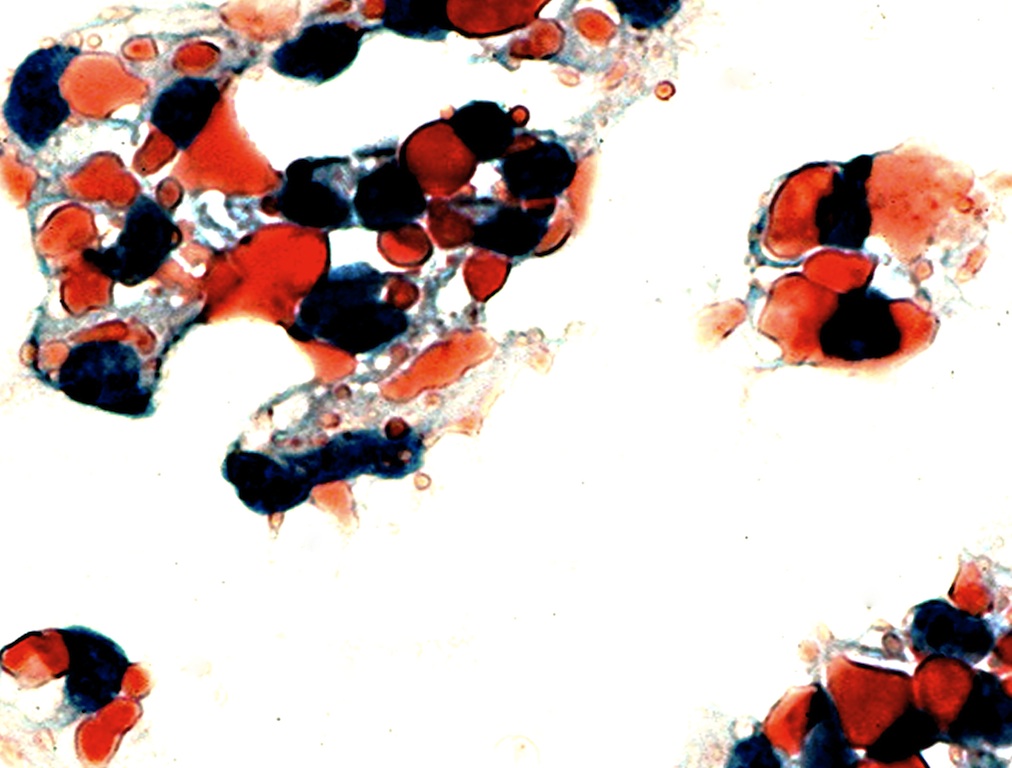
- Presence of unusual cells, not typical for thyroid, admixed with normal thyroid follicular cells (Yang: Thyroid Fine Needle Aspiration, 1st Edition, 2013)
- Cytological features of keratin, mucin or melanin are the clues to the extrathyroidal origin of the tumor
Contributed by Mark R. Wick, M.D.
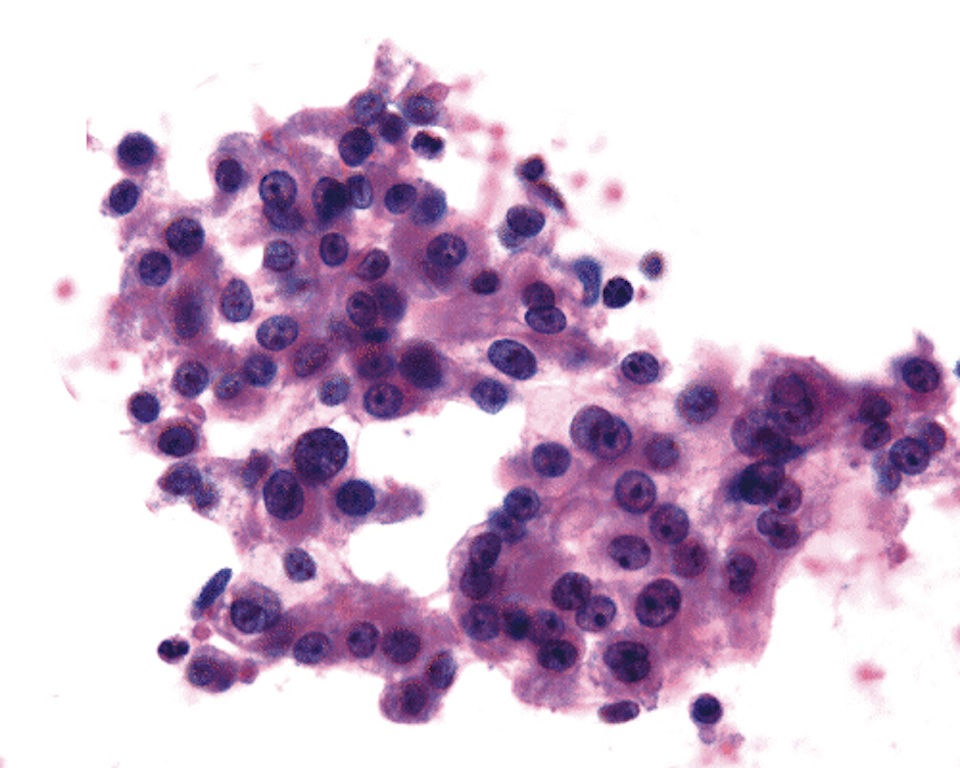
FNA: metastatic renal cell carcinoma
Images hosted on other servers:

Kidney: metastatic renal cell carcinoma, clear cell type

Kidney: bloody background with clusters of atypical cells; nuclei are somewhat pleomorphic with prominent nucleoli

Lung squamous cell carcinoma

Melanoma

Melanoma - HMB45


Parotid gland adenoid cystic carcinoma
- Thyroglobulin (may be spuriously positive due to the permeating colloid), TTF1 (but is positive in lung or small cell carcinoma)
- Secondary tumors have genetic signature matching with primary sites and mutation testing or miRNA profiling may be helpful (Lloyd: WHO Classification of Tumours of Endocrine Organs, 4th Edition, 2017)
- Various primary thyroid tumors with clear cell changes vs. clear cell renal cell carcinoma: RCC has sinusoidal blood vessels and hemorrhage in lumen, is RCC+, CD10+, CAIX+, TTF1-, thyroglobulin-; note that PAX8 is positive in both tumors
- Medullary carcinoma vs neuroendocrine neoplasm: calcitonin can be seen in small cell carcinoma
- Poorly differentiated metastatic carcinoma vs. Poorly differentiated thyroid carcinoma: the latter is thyroglobulin+, TTF1+, PAX8+ (may be focal)
- Undifferentiated metastatic carcinoma vs. Undifferentiated thyroid carcinoma: the latter is PAX8+/-, thyroglobulin+/-, TTF1+/-
- Metastasis from renal cell carcinoma is generally a solitary mass
- Metastatic clear cell renal cell carcinoma can have a very long latency after nephrectomy
- Metastatic clear cell renal cell carcinoma can have a spurious thyroglobulin stain
- TTF1 and PAX8 can be used to differentiate tumors of renal and thyroid origins
- Metastatic tumor to the thyroid gland is the initial manifestation of renal cell carcinoma in 33% of cases
Comment Here
Reference: Secondary tumors / metastases
- Metastases to the thyroid are a common finding
- Most patients with thyroid metastases have no known primary
- Melanoma is a common primary that metastasizes to the thyroid
- PAX8 may be positive in both thyroid and renal tumors
Comment Here
Reference: Secondary tumors / metastases
- Carcinomas of the breast are among the most common "donor" tumors
- Melanoma is the most common "recipient" tumor
- Most "recipient" tumors are benign
- Sarcomas are the most common "donor" tumor
- Their definition includes metastasis to lymph nodes affected by lymphoma
Comment Here
Reference: Secondary tumors / metastases

