
Thyroid & parathyroid
Low risk thyroid tumors
Hyalinizing trabecular tumor
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Andrey Bychkov, M.D., Ph.D.

Last author update: 20 January 2023
Last staff update: 20 January 2023
Copyright: 2014-2025, PathologyOutlines.com, Inc.
PubMed Search: Hyalinizing trabecular tumor

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: LiVolsi VA. Hyalinizing trabecular tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidhtn.html. Accessed March 28th, 2025.
Definition / general
- Neoplasm of follicular cells showing a trabecular growth pattern of large cells with pale to eosinophilic cytoplasm containing stromal hyaline material; the nuclear features show elongation, grooves and intranuclear inclusions (Am J Surg Pathol 1987;11:583)
Essential features
- Trabecular architecture
- Yellow bodies
- MIB1 membrane staining of tumor cells
- GLIS translocation is unique to this thyroid tumor
Terminology
- Hyalinizing trabecular neoplasm, hyalinizing trabecular adenoma
ICD coding
- ICD-O: 8336/0 - hyalinizing trabecular adenoma
Epidemiology
- Hyalinizing trabecular tumor (HTT) comprises fewer than 1% of thyroid neoplasms, shows a female preponderance > 80% and occurs in adults (mean age 50 years) (Am J Surg Pathol 2008;32:1877)
Sites
- Thyroid
Etiology
- Unknown
Clinical features
- HTT occurs in asymptomatic individuals and is usually an incidental finding on ultrasonography or by clinical examination
- In approximately 30% of cases, chronic lymphocytic thyroiditis is present (Thyroid 2011;21:253)
Diagnosis
- Neither ultrasound nor radioactive scans can diagnose HTT; fine needle aspiration results are often characterized as atypia of undetermined significance; definitive diagnosis is rarely made preoperatively (J Clin Pathol 2017;70:641, Diagn Cytopathol 2015;43:710, Cancer Cytopathol 2019;127:390)
Laboratory
- Thyroid function tests are usually within normal limits; no specific preoperative test is definitive
Prognostic factors
- Overwhelming majority of HTT are benign neoplasms; very rare examples showing capsular or vascular invasion have been reported (Am J Surg Pathol 2008;32:1877, Histopathology 1996;28:357)
Case reports
- 44 year old woman with thyroid nodule (Ultrasound Int Open 2017;3:E42)
- 54 year old woman with chronic lymphocytic thyroiditis (J Surg Case Rep 2021;2021:rjab324)
- 70 year old woman with incidental right lobe nodule (Thyroid Res 2017;10:7)
Treatment
- Surgery with removal of the affected thyroid lobe is curative
Gross description
- Lesion is circumscribed or encapsulated without gross evidence of invasion
- Tumor ranges in size from 5 mm - 7.5 cm; half of the tumors measure 3 cm or less
- On section, the tumor is yellow to white in color
- Cut surface is solid, slightly bulging and may show lobulation
Gross images
Images hosted on other servers:

Encapsulated gray white nodular lesion

Gray white with one area showing cystic degeneration
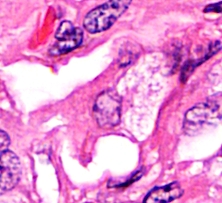
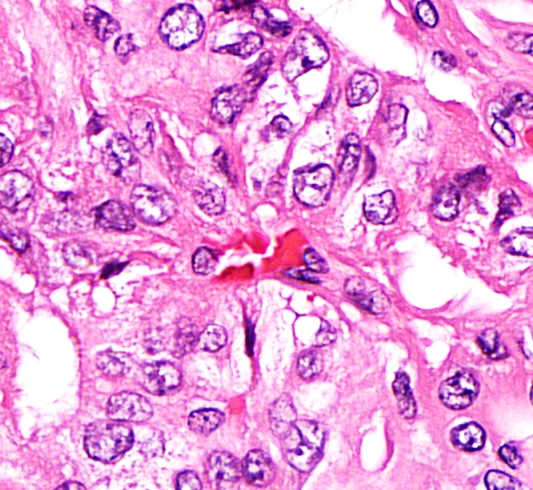
Microscopic (histologic) description
- Trabecular growth pattern
- Large, elongated cells with voluminous eosinophilic cytoplasm
- > 50% of cases show intracytoplasmic 2 - 5 micron yellow perinuclear inclusions (yellow bodies) with surrounding clear halo; these represent giant lysosomes (Am J Surg Pathol 1999;23:118, Arch Pathol Lab Med 2003;127:715)
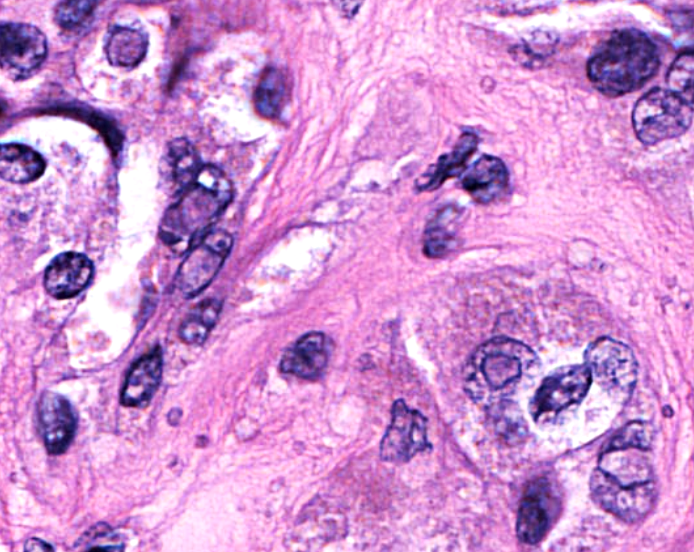
- Nuclei are enlarged and elongated or oval
- Nuclear grooves and intranuclear inclusions are seen in all cases
- Hyaline material seen in extracellular space
- Stromal calcifications are frequent
- No vascular or capsular invasions are noted (Am J Surg Pathol 1987;11:583, Arch Pathol Lab Med 2003;127:715, Am J Surg Pathol 1999;23:118, Am J Surg Pathol 2008;32:1877)
Microscopic (histologic) images
Contributed by Virginia A. Livolsi, M.D.
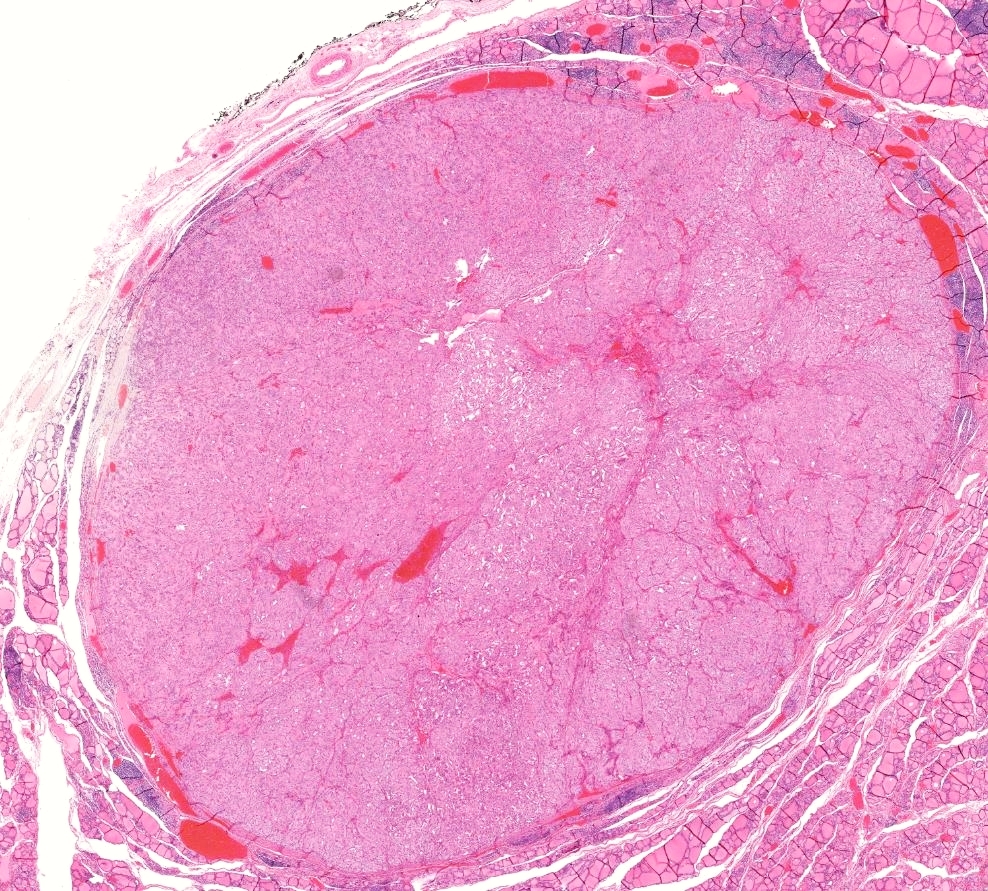
HTT thinly encapsulated
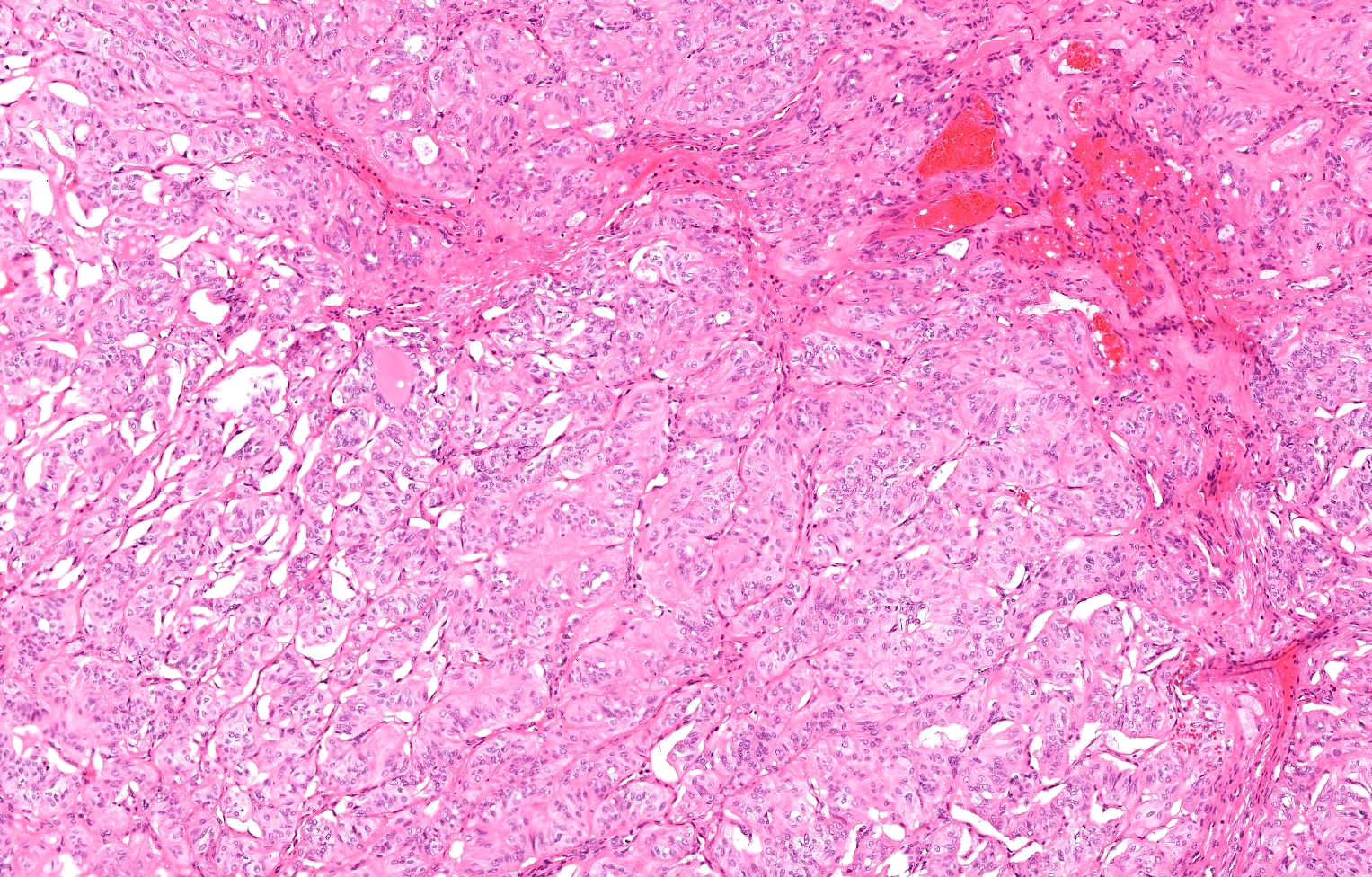
Solid trabecular growth
Trabecular pattern noted
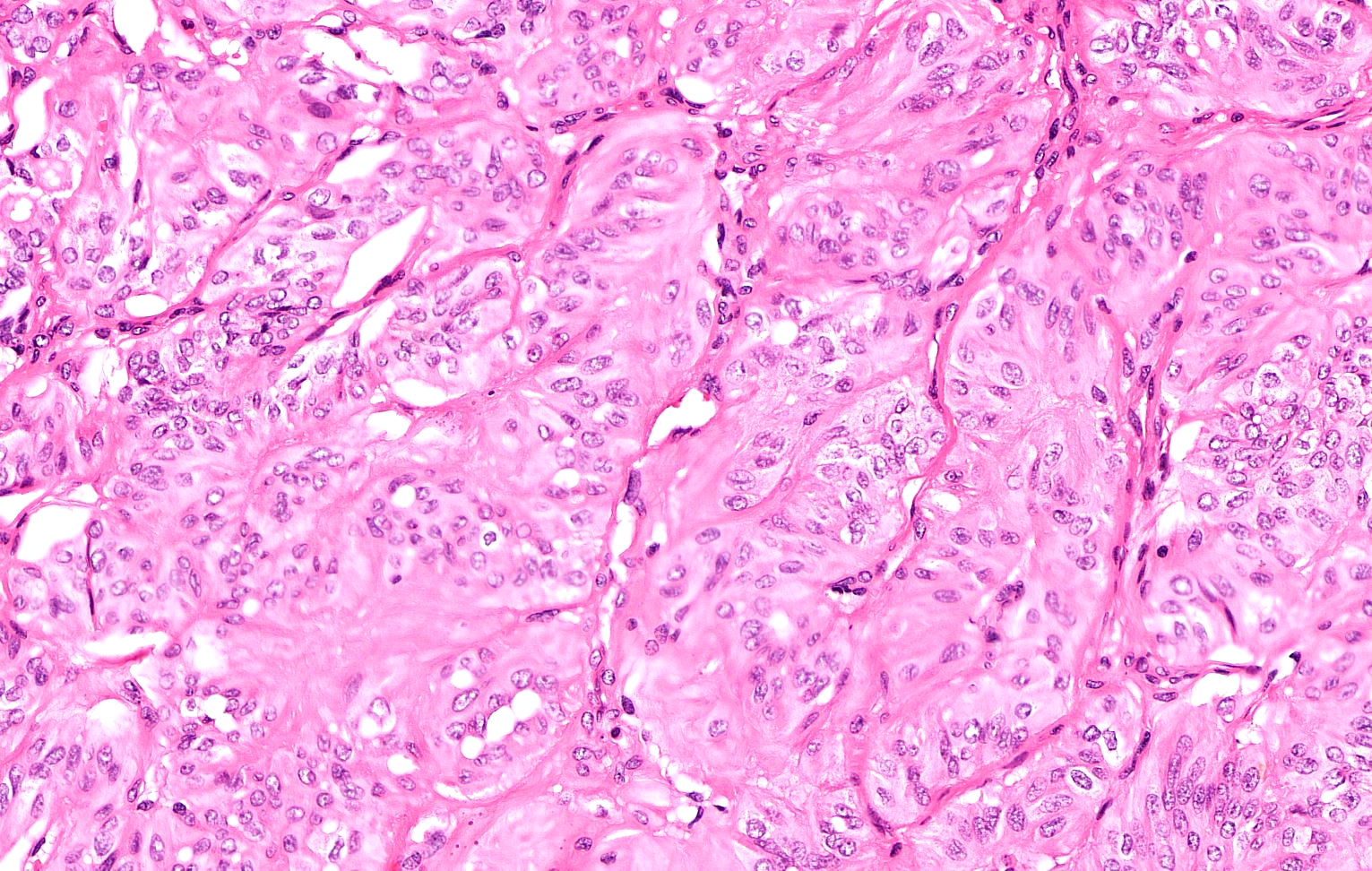
Elongated nuclei
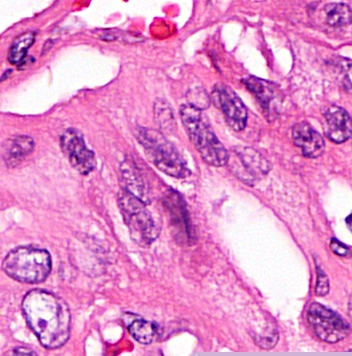
Prominent intranuclear inclusion
Nuclear clearing and grooves
Yellow bodies
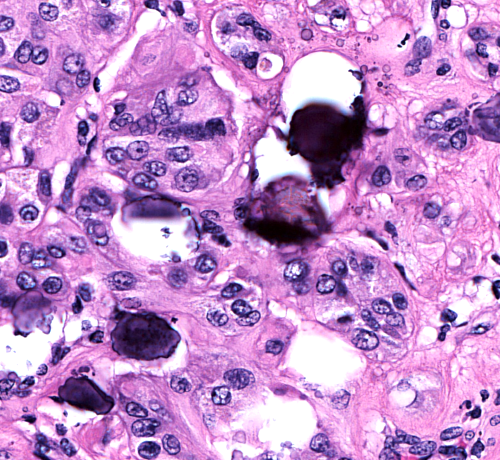
Calcification in tumor stroma
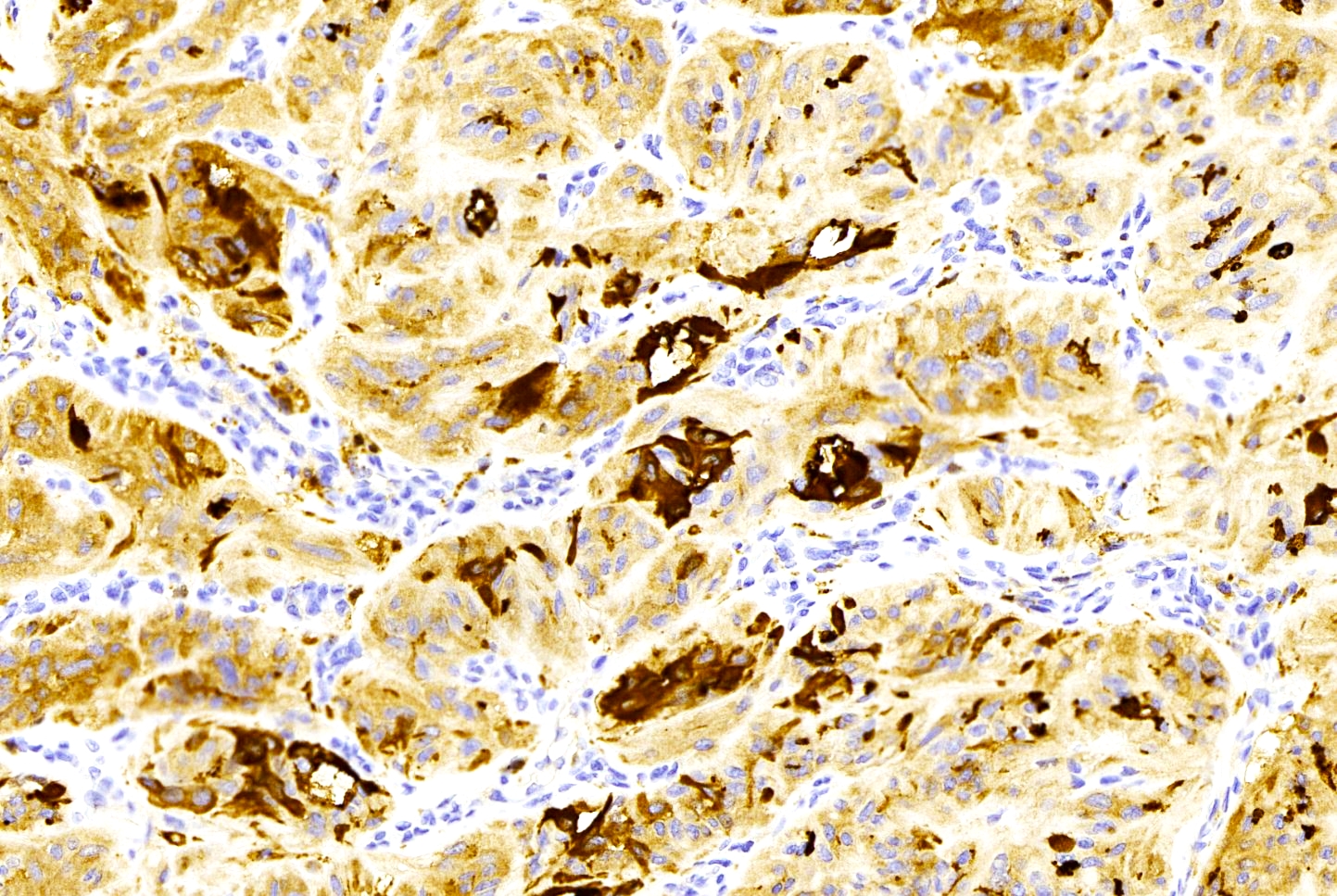
Thyroglobulin stain variable
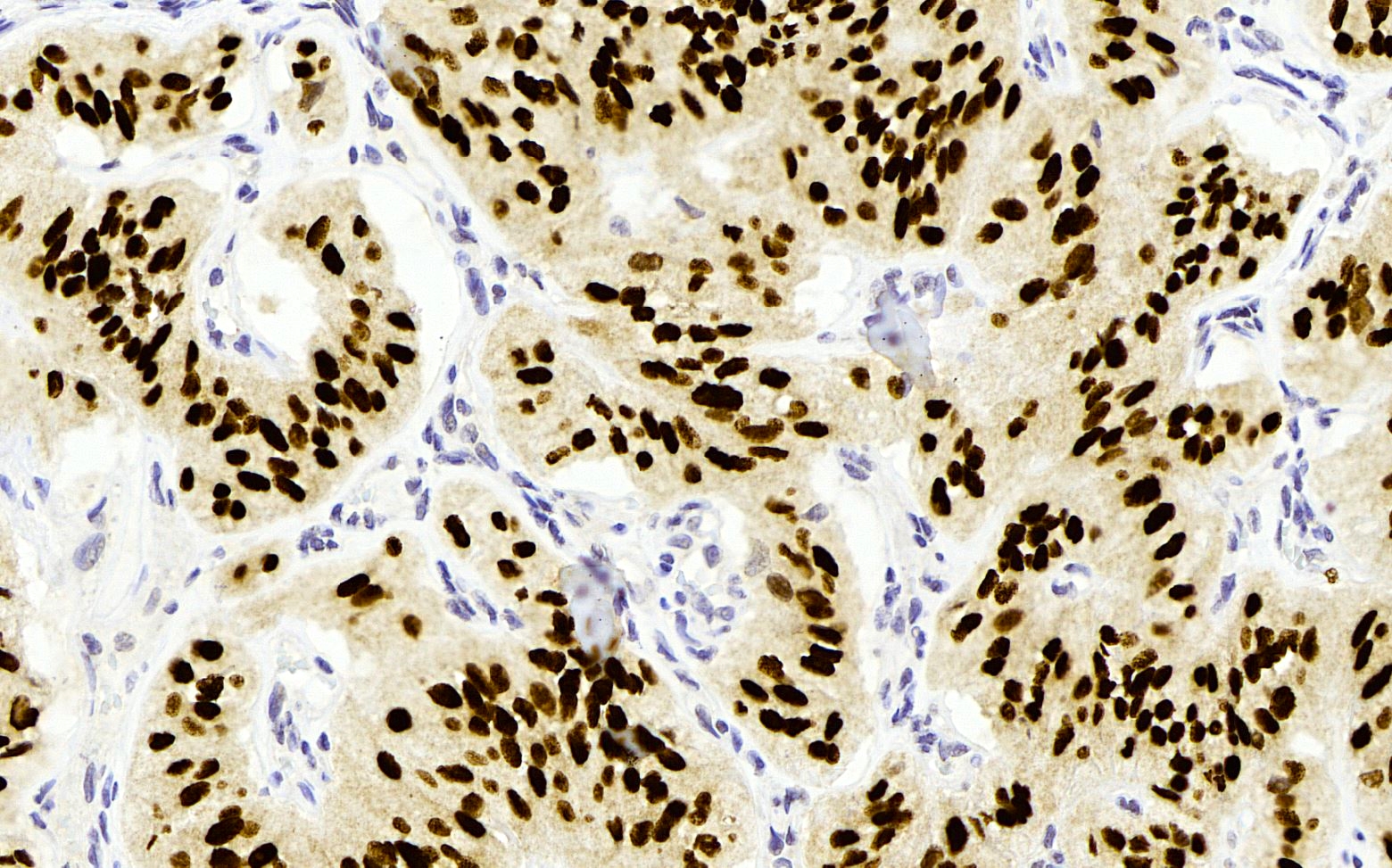
TTF1 decorates nuclei
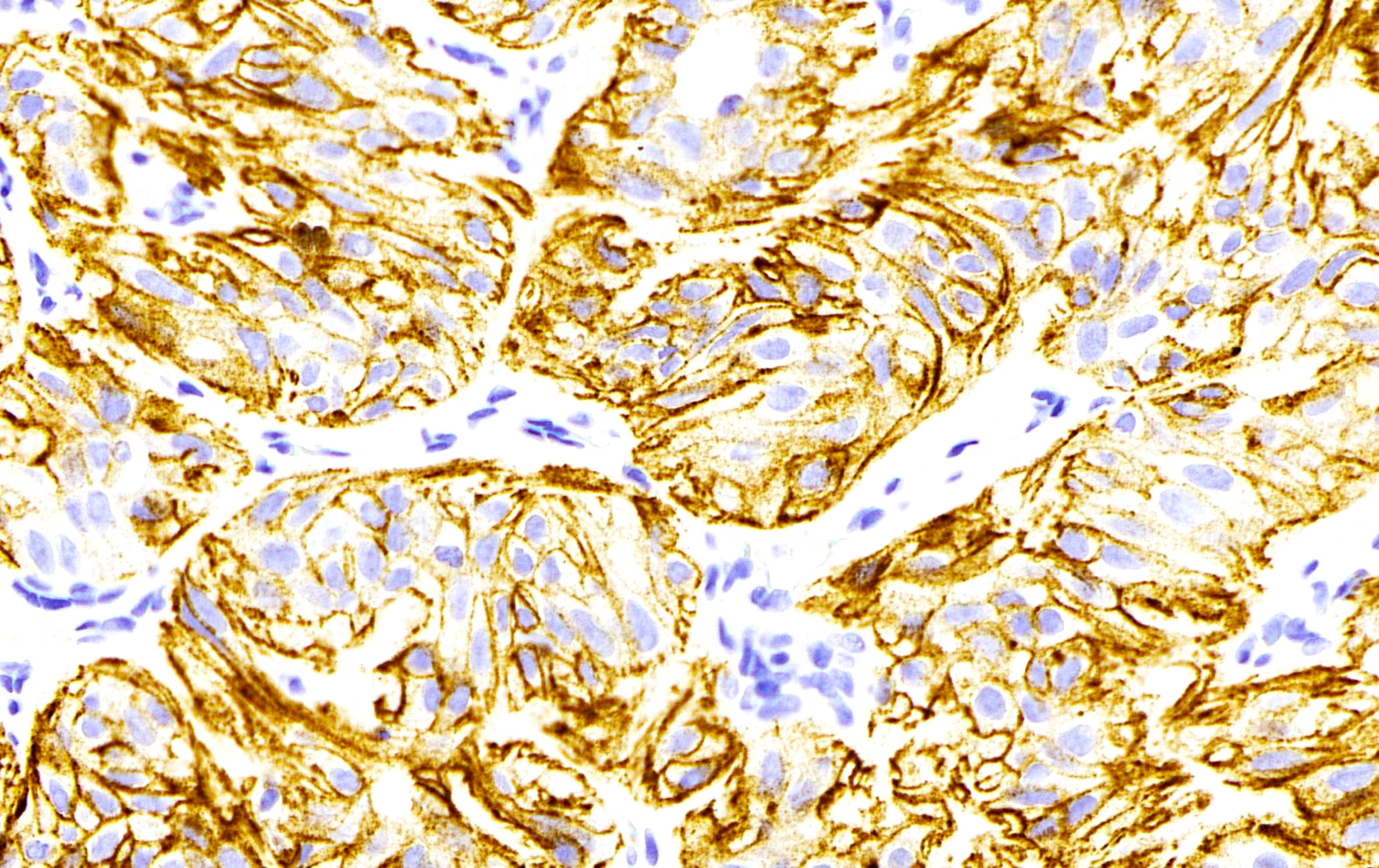
Ki67 decorates membranes
Cytology description
- Usually hypercellular smears
- Cells radially oriented around hyaline material
- Tumor cells elongated with abundant cytoplasm
- Enlarged, elongated nuclei with nuclear clearing, grooves and inclusions; clearing may not be prominent
- Cytoplasmic staining by MIB1 is characteristic
- Stromal amorphous material may be mistaken for amyloid (Congo red stain negative)
- Because of nuclear features and stromal deposits, cytology may be classified as either papillary carcinoma or medullary carcinoma
- References: Am J Surg Pathol 2004;28:859, Diagn Cytopathol 2015;43:710, J Clin Pathol 2017;70:641, Cancer Cytopathol 2019;127:390
Cytology images
Contributed by Ayana Suzuki, C.T.
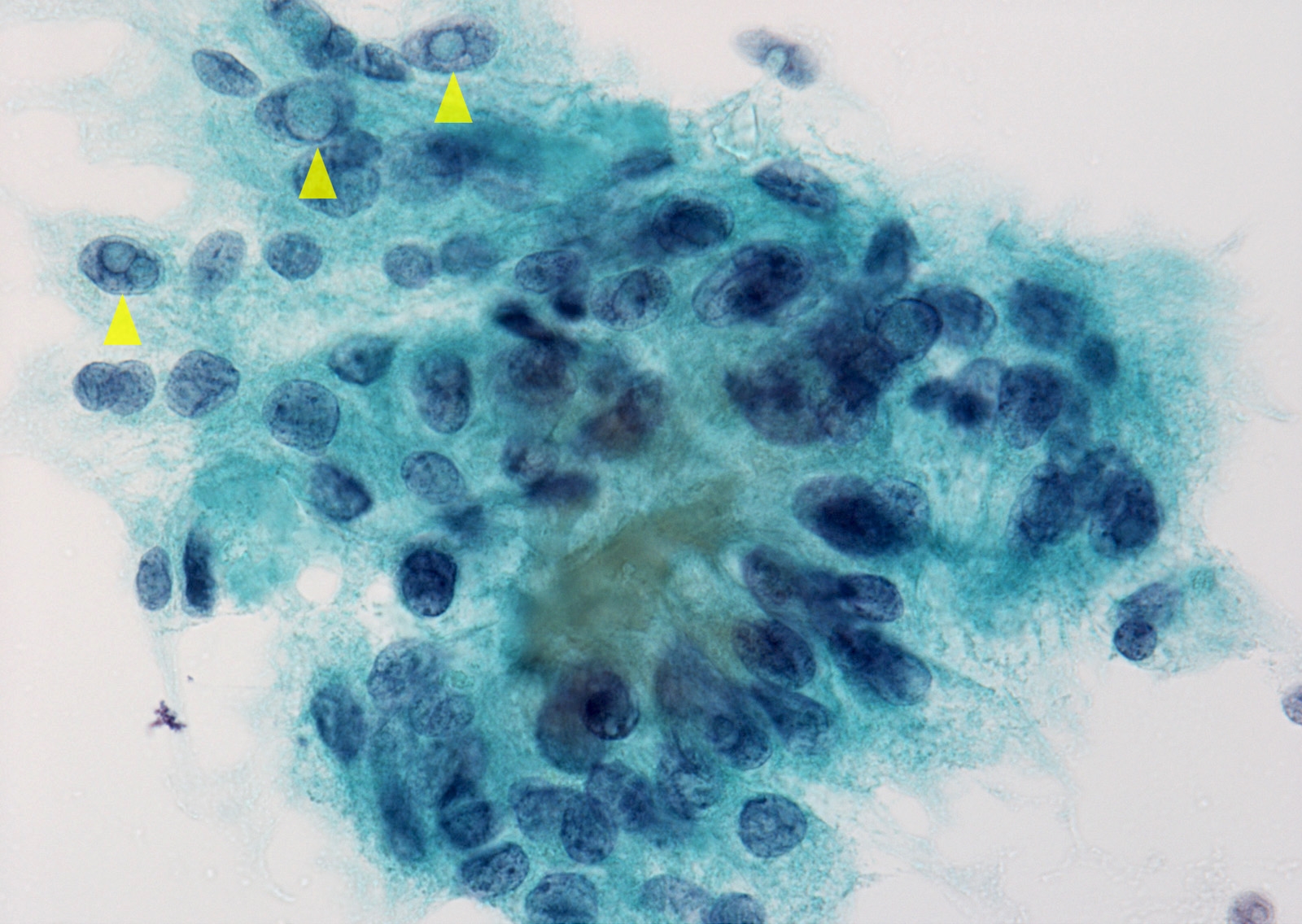
Nuclear pseudoinclusions
Positive stains
- Thyroglobulin
- TTF1
- PAX8
- Cytokeratin
- Ki67 membrane staining is unique to HTT (MIB1 monoclonal antibody at room temp must be used) (Am J Clin Pathol 2004;122:506, Am J Surg Pathol 2000;24:575, Am J Surg Pathol 2008;32:1877, Head Neck Pathol 2020;14:778)
Negative stains
Electron microscopy description
- Giant lysosomes are found in the cytoplasm
Molecular / cytogenetics description
- Characteristic rearrangement of GLIS; only HTT of all thyroid tumors tested thus far demonstrate rearrangement of GLIS (PAX8-GLIS1 and PAX8-GLIS3 [most frequent]) (Cancer Cytopathol 2019;127:560, Mod Pathol 2019;32:1734)
- No BRAF mutation (Appl Immunohistochem Mol Morphol 2007;15:220)
- No RAS mutations (Appl Immunohistochem Mol Morphol 2007;15:220)
- RET / PTC translocations reported but further study makes these reports doubtful (Am J Surg Pathol 2000;24:1615, Eur J Cancer 2005;41:816, Histopathology 2010;56:632)
Sample pathology report
- Thyroid, right lobe, lobectomy:
- Hyalinizing trabecular tumor, 2.5 cm nodule (see comment)
- Comment: Specimen weighs 12 g and measures 4.2 x 2.8 x 1 cm. The surface is smooth and shows a bulging nodule in the lower portion of the lobe. On sectioning, the nodule is solid, tan and circumscribed.
Differential diagnosis
- Medullary thyroid carcinoma:
- Stains for calcitonin and chromogranin A
- Stromal amyloid is seen in 75% of these cancers
- Nuclei show salt and pepper morphology
- Paraganglioma:
- Tumor cells are chromogranin A positive; intermixed S100 positive sustentacular cells should be noted
- Nuclear morphology resembles the salt and pepper nuclei of neuroendocrine cells
- Papillary thyroid carcinoma:
- HTT does not show papillary growth and if follicles are produced they tend to be empty
- Most papillary carcinomas show invasive growth pattern
Board review style question #1
This solitary thyroid nodule represents
- Hyalinizing trabecular tumor
- Medullary thyroid carcinoma
- Papillary thyroid carcinoma, trabecular variant
- Paraganglioma
Board review style answer #1
Board review style question #2
The molecular signature of the tumor illustrated is
- BRAF K601 mutation
- BRAF V600E mutation
- GLIS rearrangement
- NRAS mutation
Board review style answer #2
