

Thyroid & parathyroid
Thyroiditis
Subacute thyroiditis
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Andrey Bychkov, M.D., Ph.D.

Last author update: 11 January 2022
Last staff update: 11 January 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Subacute thyroiditis pathology "last 5 years"[DP]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Nguyen TPX, Vuong HG. Subacute thyroiditis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidgranuloma.html. Accessed April 19th, 2024.
Definition / general
- Granulomatous inflammation of the thyroid gland with characteristic clinical and microscopic findings
- Most common cause of thyroid related neck pain and typically occurs a few weeks after a viral infection
Essential features
- Diagnosed mainly based on clinical findings (e.g. fever, odynophagia, thyroid tenderness)
- Histopathologically, characterized by granulomatous inflammation composed of multinucleated giant cells, foamy and epithelioid histiocytes, neutrophils, lymphocytes and plasma cells
Terminology
- Historical name: de Quervain thyroiditis
- Synonyms: subacute granulomatous thyroiditis, de Quervain thyroiditis, painful subacute thyroiditis, postviral thyroiditis, giant cell thyroiditis, subacute nonsuppurative thyroiditis, pseudotuberculous thyroiditis, struma granulomatosa
ICD coding
- ICD-10: E06.1 - subacute thyroiditis
Epidemiology
- Mostly seen in middle aged women
- Appears to be seasonal, as most cases occur in the summer and fall (Am Fam Physician 2006;73:1769)
- Young children affected by subacute thyroiditis have been reported (BMJ Case Rep 2020;13:e236909, Clin Pediatr Endocrinol 2021;30:75)
Sites
- Entire gland is usually involved (Heilo: Atlas of Thyroid Lesions, 1st Edition, 2011)
Etiology
- Associated with coxsackievirus, echovirus infections, mumps, measles, influenza and other viruses (Rev Endocr Metab Disord 2021 May 5 [Epub ahead of print], Thompson: Diagnostic Pathology - Head and Neck, 2nd Edition, 2016)
- May be related to pregnancy (J Endocrinol Invest 2006;29:924)
- SARS-CoV-2 can be a potent triggering factor (Rev Endocr Metab Disord 2021 May 5 [Epub ahead of print], SN Compr Clin Med 2021 Apr 29 [Epub ahead of print], Cancer Cytopathol 2021;129:844)
- Several human leukocyte antigen (HLA) alleles increase the risk of acquiring and recurrence (HLA-B*35, HLA-B*18:01, -DRB1*01 and HLA-C*04:01) (Rev Endocr Metab Disord 2021 May 5 [Epub ahead of print])
Diagrams / tables
Images hosted on other servers:

Thyroid function
Clinical features
- Fatigue, low grade fever, myalgias, along with neck pain and diffuse goiter
- Self limited in most of cases, usually resolves in 1 - 2 months
- Presence of a deterioration of tachycardia or an occurrence of heart arrhythmias were reported in COVID-19 patients with subacute thyroiditis (Rev Endocr Metab Disord 2021 May 5 [Epub ahead of print])
- May occasionally coincide with thyroid malignancy (Arq Bras Endocrinol Metabol 2014;58:851)
- 26.8% of subacute thyroiditis patients developed permanent hypothyroidism within 3 years of treatment (Exp Clin Endocrinol Diabetes 2020;128:703)
Diagnosis
- Mainly based on clinical findings (fever, malaise, fatigue, muscle aches, neck pain, thyroid gland tenderness, odynophagia)
- May have hypo or hyperthyroidism symptoms (Int J Endocrinol 2014;2014:794943)
- May have atypical symptoms: thyroid storm, fever of unknown origin, solitary painless thyroid nodule (Cureus 2021;13:e16399, Int J Surg Case Rep 2017;33:112)
Laboratory
- Thyrotoxic phase: hyperthyroid (suppressed thyroid stimulating hormone [TSH] and elevated T4 and T3) due to follicle destruction and release of hormone
- After 4 - 8 weeks: TSH and free T4 levels may be low (Am Fam Physician 2014;90:389)
Radiology description
- Sonography: diffuse hypoechoic and confluent areas with characteristic features like lava flow (Acta Radiol 2014;55:429, Cytojournal 2015;12:9)
- Radioactive iodine uptake in acute phase is very low (< 1% at 24 hours); usually restored with recovery (Am Fam Physician 2014;90:389)
- Increased 18F-FDG uptake on PET / CT (Medicine (Baltimore) 2017;96:e7535)
Radiology images
Contributed by Ayana Suzuki, C.T.
Hypoechoic nodule
Images hosted on other servers:

Hypoechoic nodule with poorly defined margin

High 18F-FDG uptake in enlarged right thyroid lobe
Prognostic factors
- Self limited, with patients returning to a euthyroid state within a few months
- Up to 2% recurrence (Thompson: Diagnostic Pathology - Head and Neck, 2nd Edition, 2016)
Case reports
- 3 year old girl with Epstein-Barr virus infection (Thyroid 2005;15:1189)
- 39 year old woman presented with acute thyroid swelling (Endocr Pathol 2002;13:263)
- 39 year old woman with thyroid nodule (Head Neck Pathol 2019;13:231)
- 44 year old man with fever, tenderness in the right neck and odynophagia (Pathology Case Reviews 2015;20:105)
- 45 year old man with numerous subcutaneous nodules and diffuse muscle pain in the neck (Ann Clin Lab Sci 2017;47:620)
- 46 year old woman who underwent US-FNA for a suspicious thyroid nodule (Diagn Cytopathol 2015;43:399)
- 48 year old woman who underwent FNA of a left thyroid mass (Diagn Cytopathol 2016;44:682)
- 51 year old man with a history of fever, gradual right neck swelling and pain (Diagn Cytopathol 2012;40:433)
Treatment
- Anti-inflammatory treatment is the key
- In some patients, no treatment is required
- Symptoms of hyperthyroidism need to be treated with propranolol or atenolol with close follow up
- Therapy with antithyroid drugs is not indicated because the disorder is caused by the release of preformed thyroid hormone from destroyed follicles instead of synthesis of new T3 and T4 (Am Fam Physician 2000;61:1047)
Microscopic (histologic) description
- Inflammatory infiltrate composed of multinucleated giant cells, foamy histiocytes, epithelioid histiocytes, neutrophils, lymphocytes, plasma cells
- Variable background of fibrosis
- Temporal trend
- Early stage (acute; hyperthyroidism):
- Follicular damage and loss of epithelium and colloid
- Neutrophils, occasional microabscesses
- Inflammation (predominantly lymphohistiocytic), which expands into adjacent interfollicular zones
- Mid stage (hypothyroidism):
- Chronic inflammation: lymphocytes, plasma cells
- Epithelioid and nonepithelioid macrophages and multinucleated giant cells adjacent to or within disrupted follicles, surround and engulf residual colloid
- Well formed granulomata are not seen
- Variable degrees of fibrosis
- Late stage (resolution; recovery):
- Fibrosis replaces destroyed follicles
- Follicular tissue is regenerated, restoring normal structure
- Fibrosis and inflammatory infiltrate resolves
- Early stage (acute; hyperthyroidism):
- Inflammatory process unevenly affects entire gland (65% bilateral) (Thompson: Diagnostic Pathology - Head and Neck, 2nd Edition, 2016)
- Nowadays, rarely seen in resection specimens because of conservative treatment and no need for surgery (Nikiforov: Diagnostic Pathology and Molecular Genetics of the Thyroid, 3rd Edition, 2019)
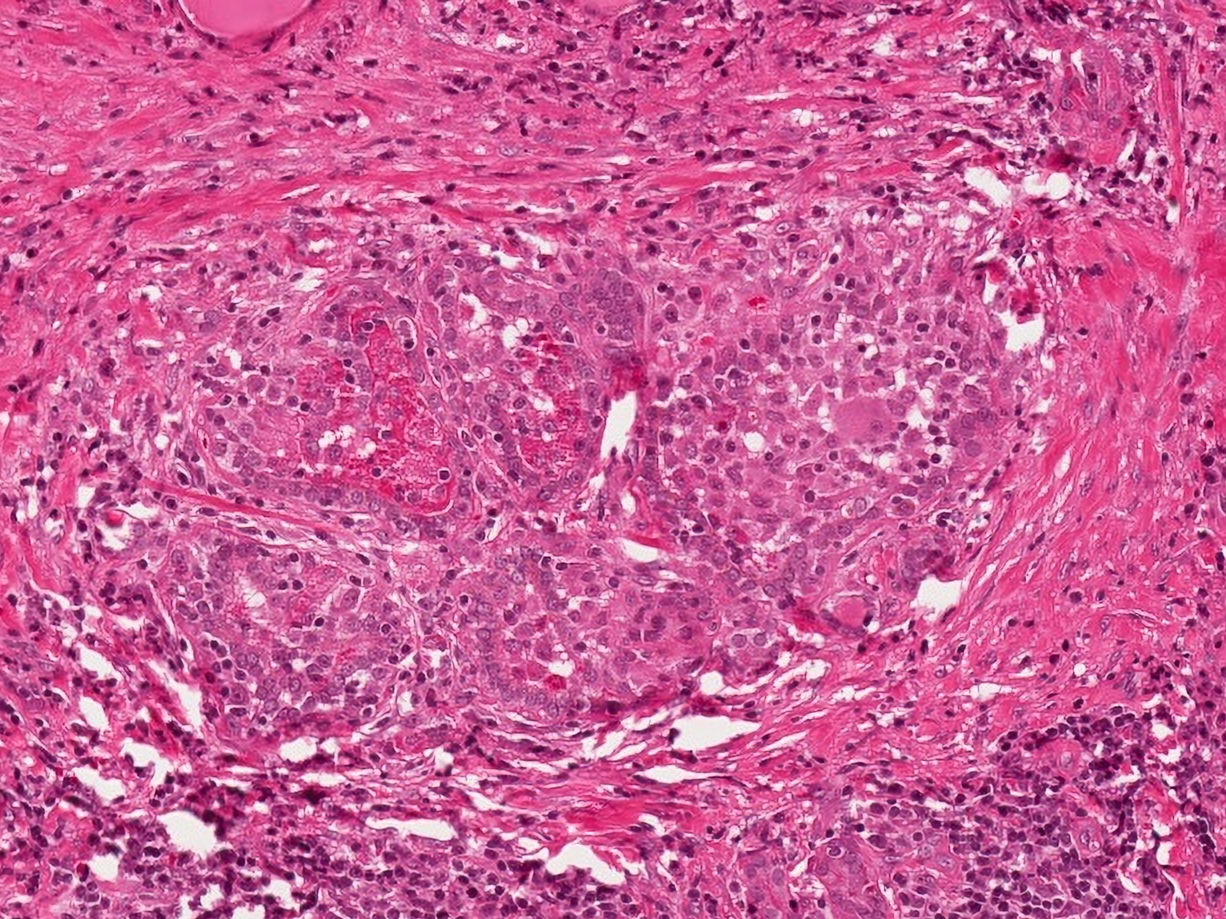
Microscopic (histologic) images
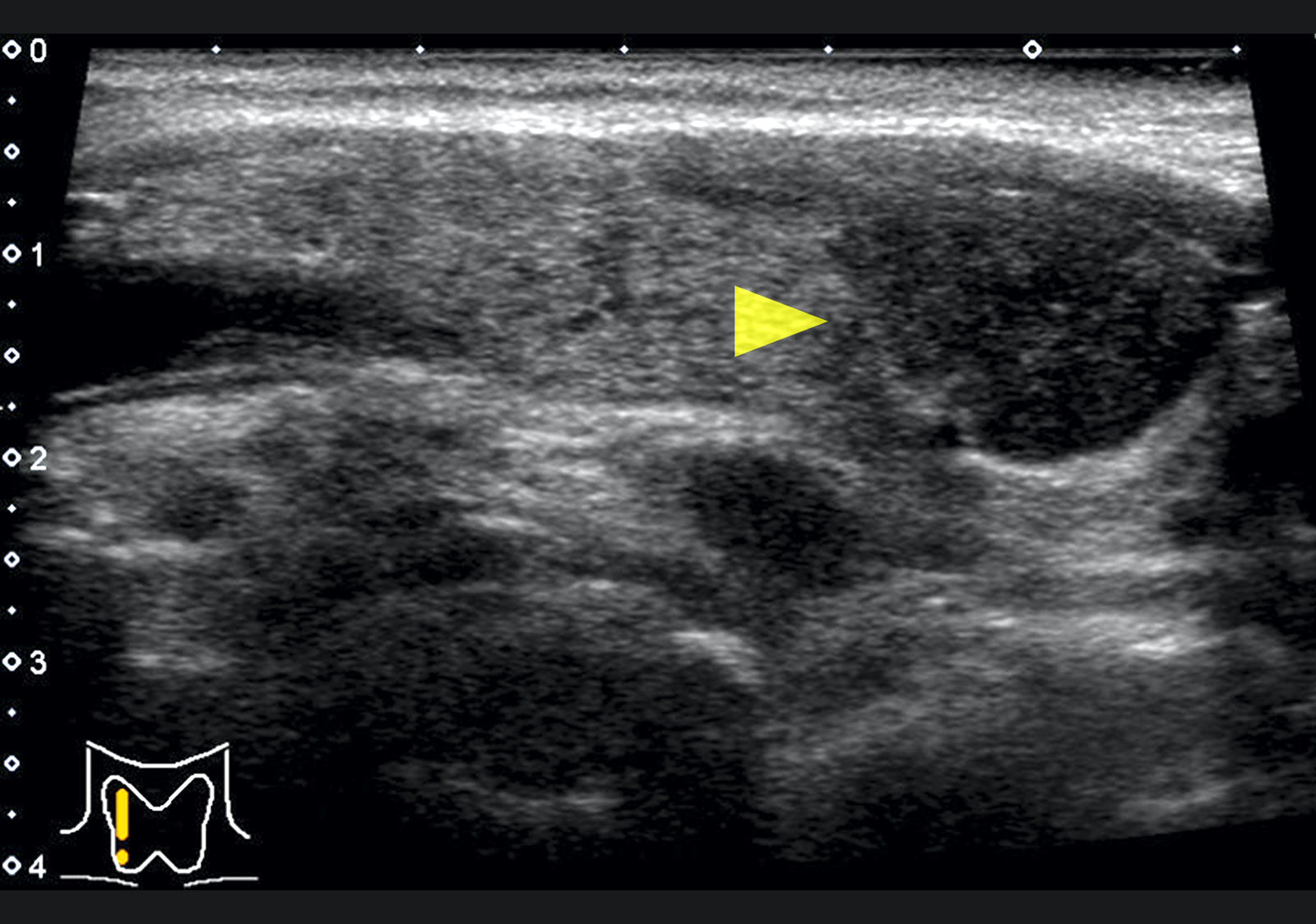
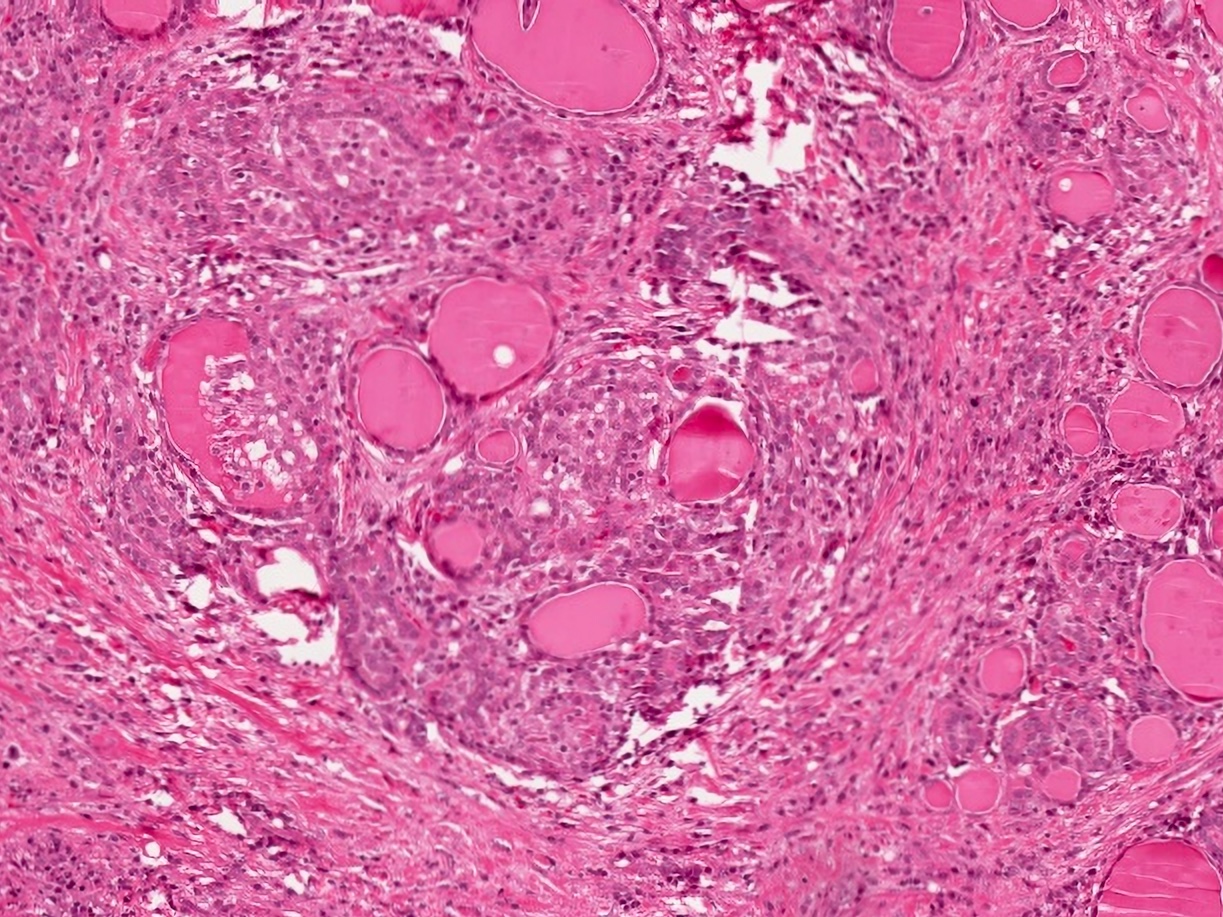
Contributed by Truong Phan Xuan Nguyen, M.D.
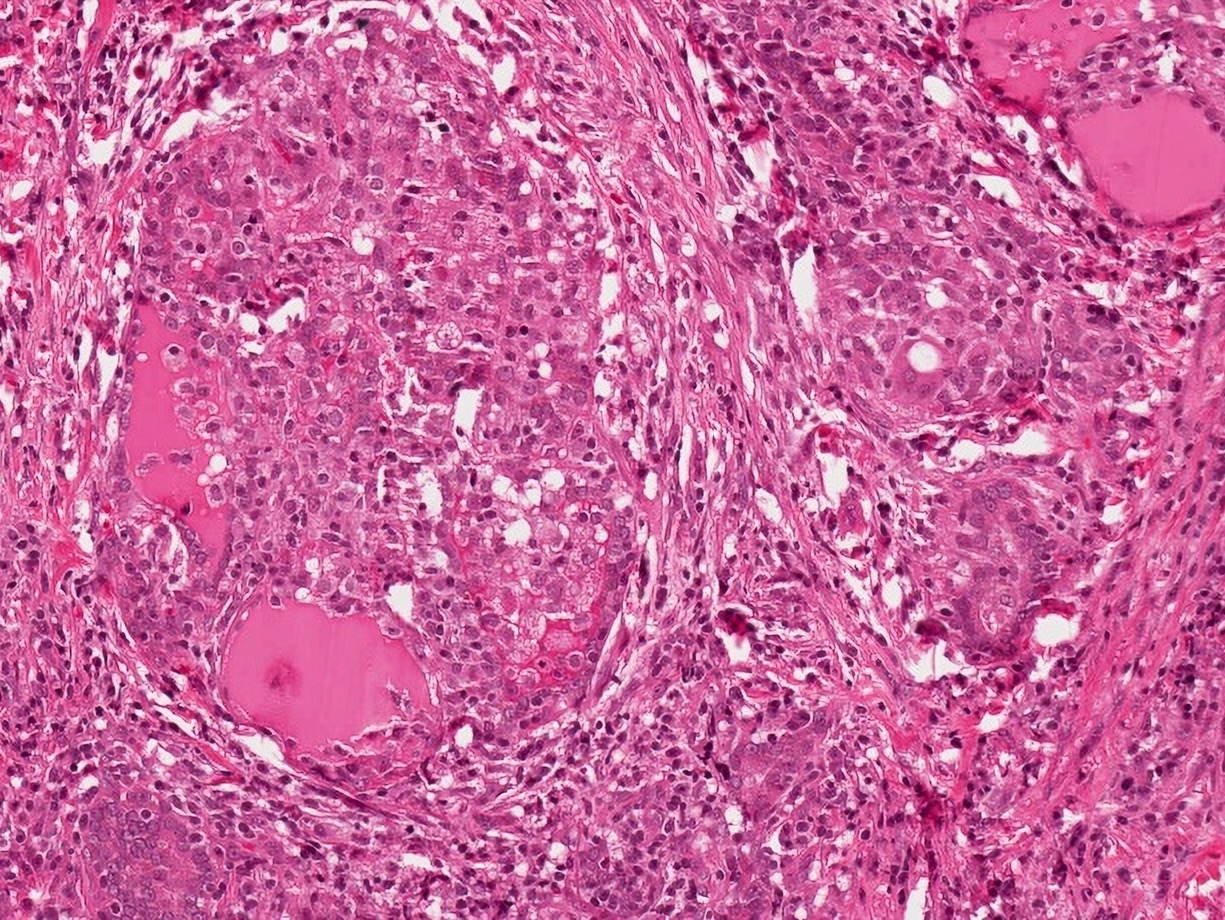
Follicular damage
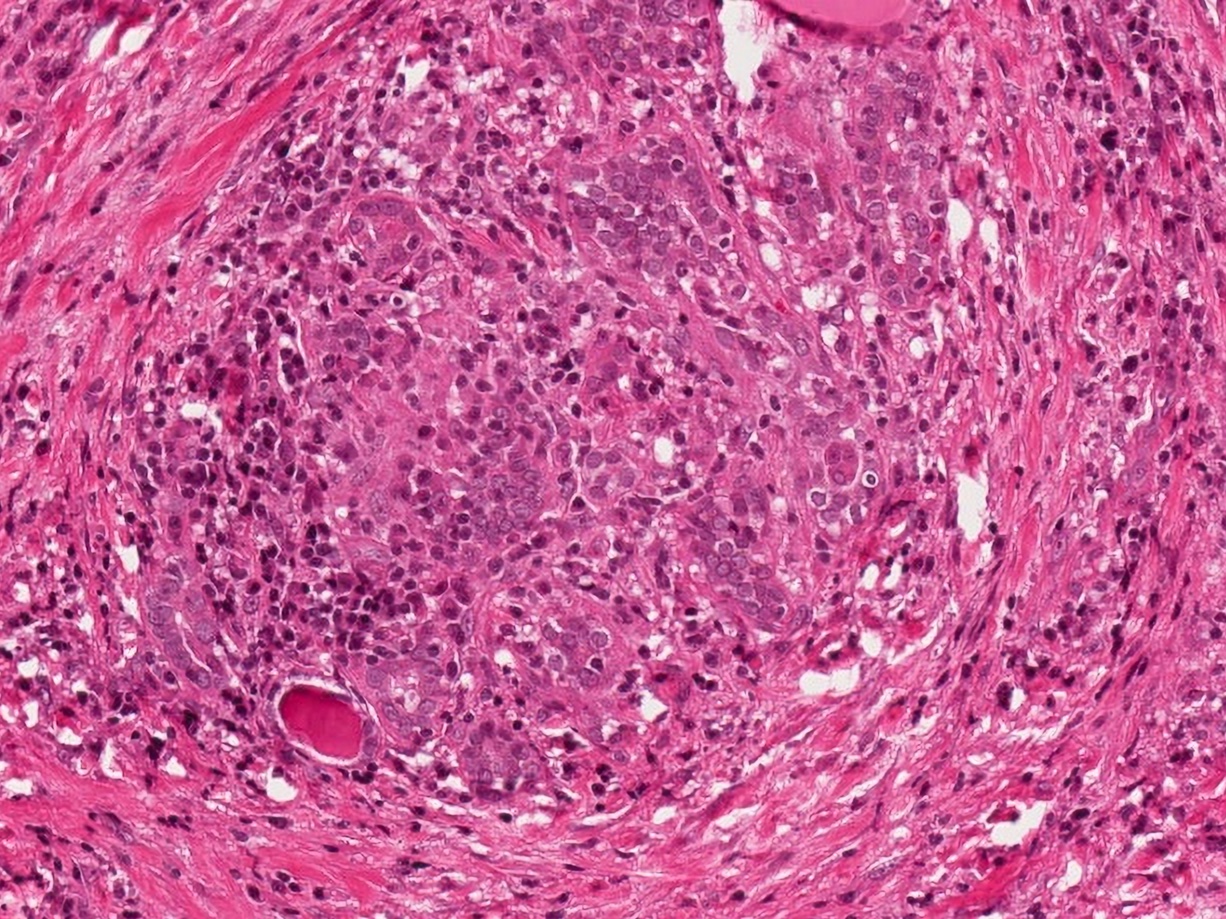
Granuloma
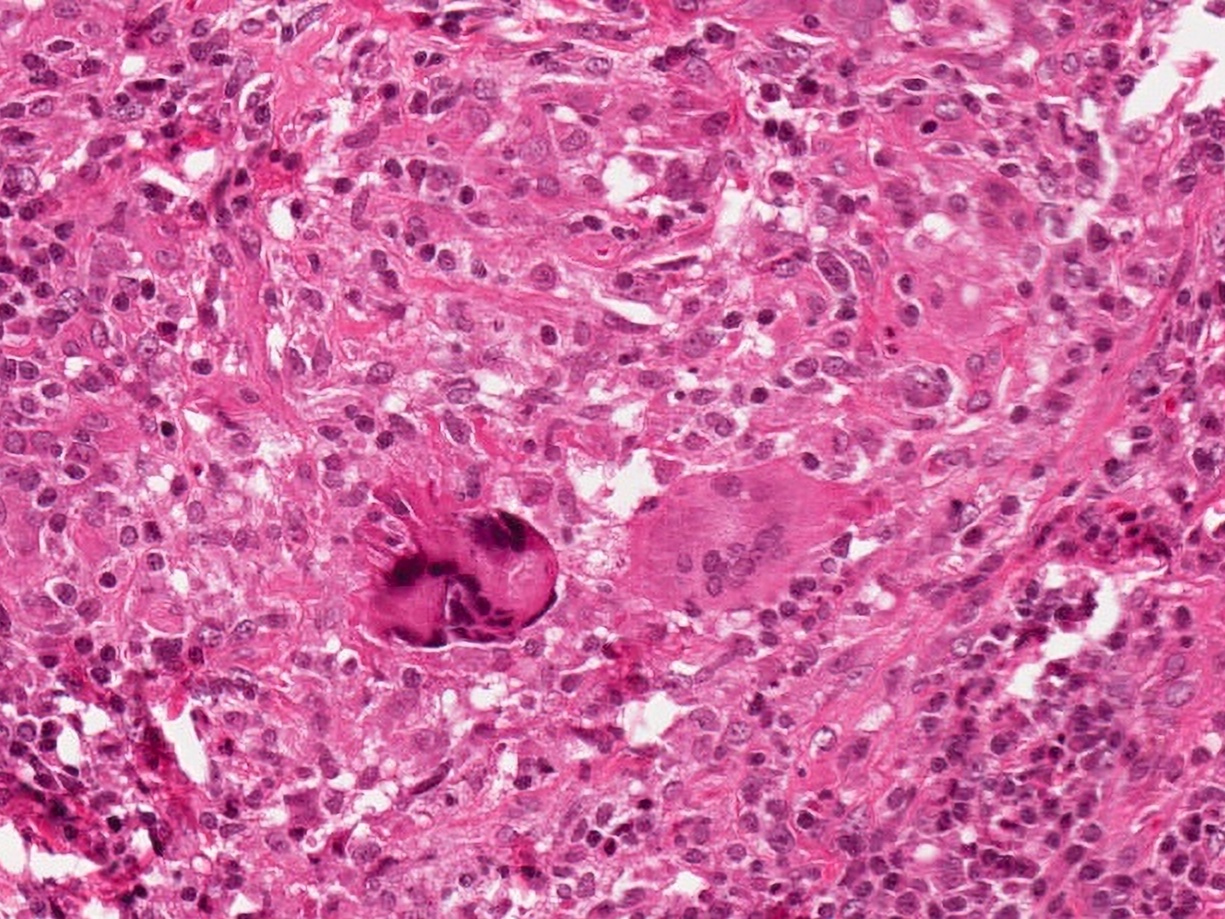
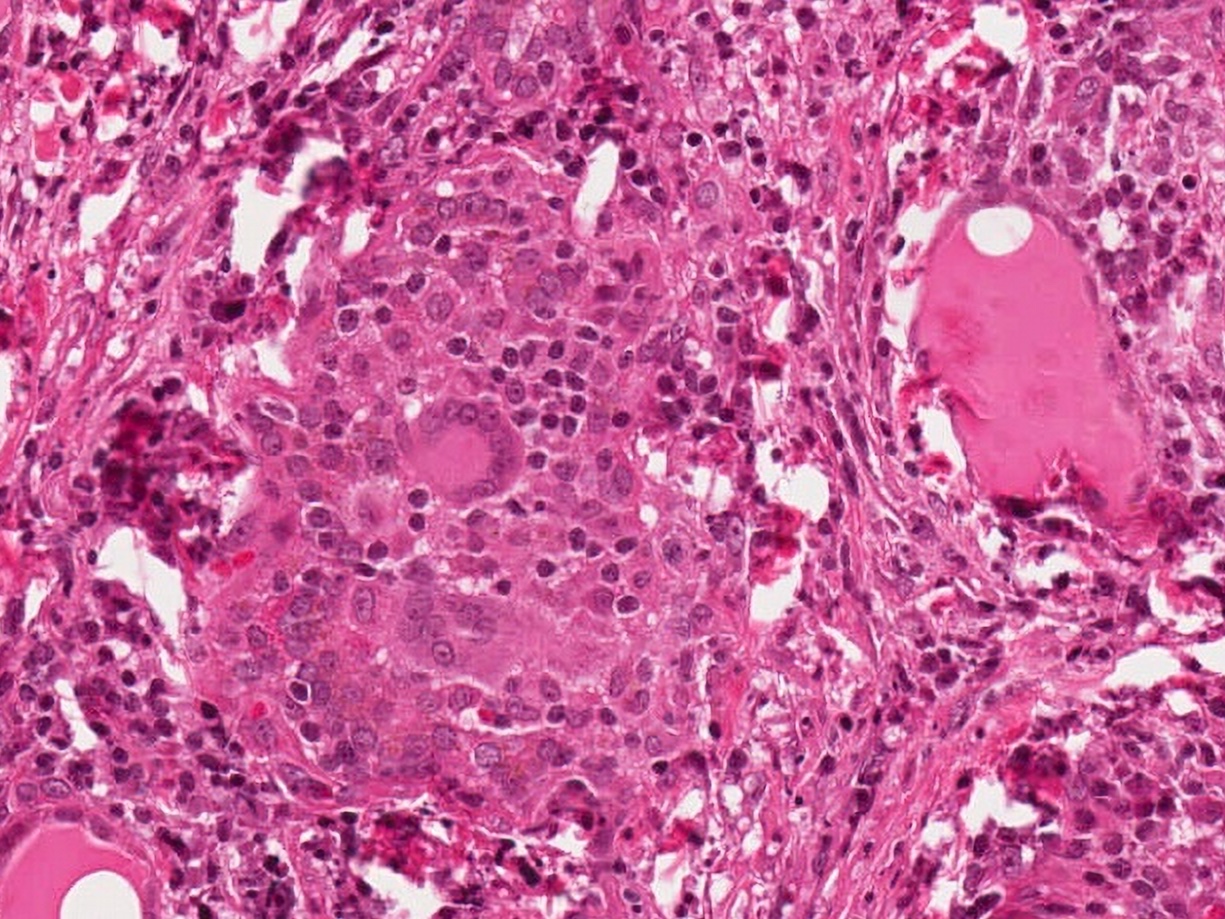
Multinucleated giant cells
Virtual slides
Images hosted on other servers:

Subacute thyroiditis

Acute (subacute) nonsuppurative thyroiditis
Cytology description
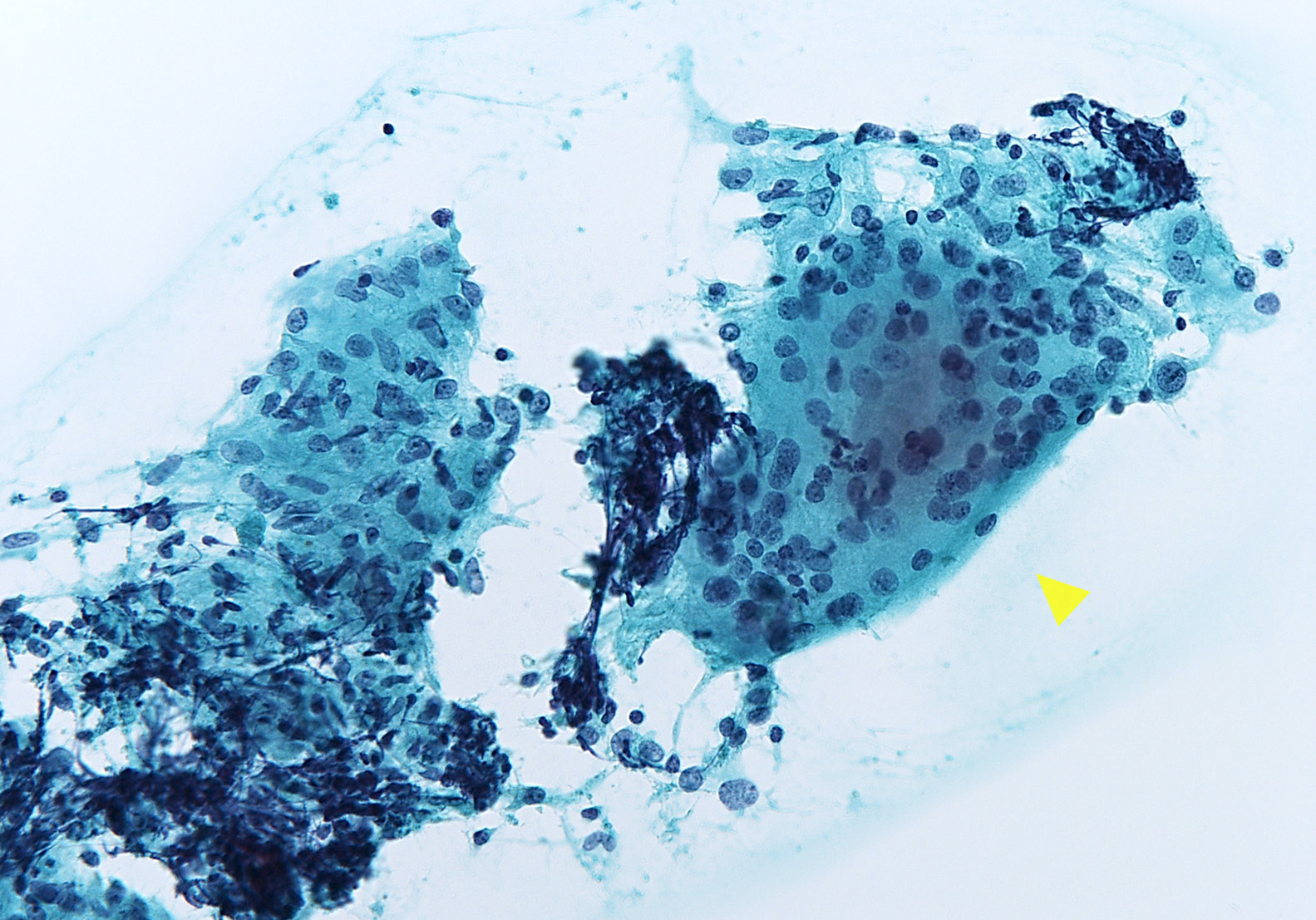
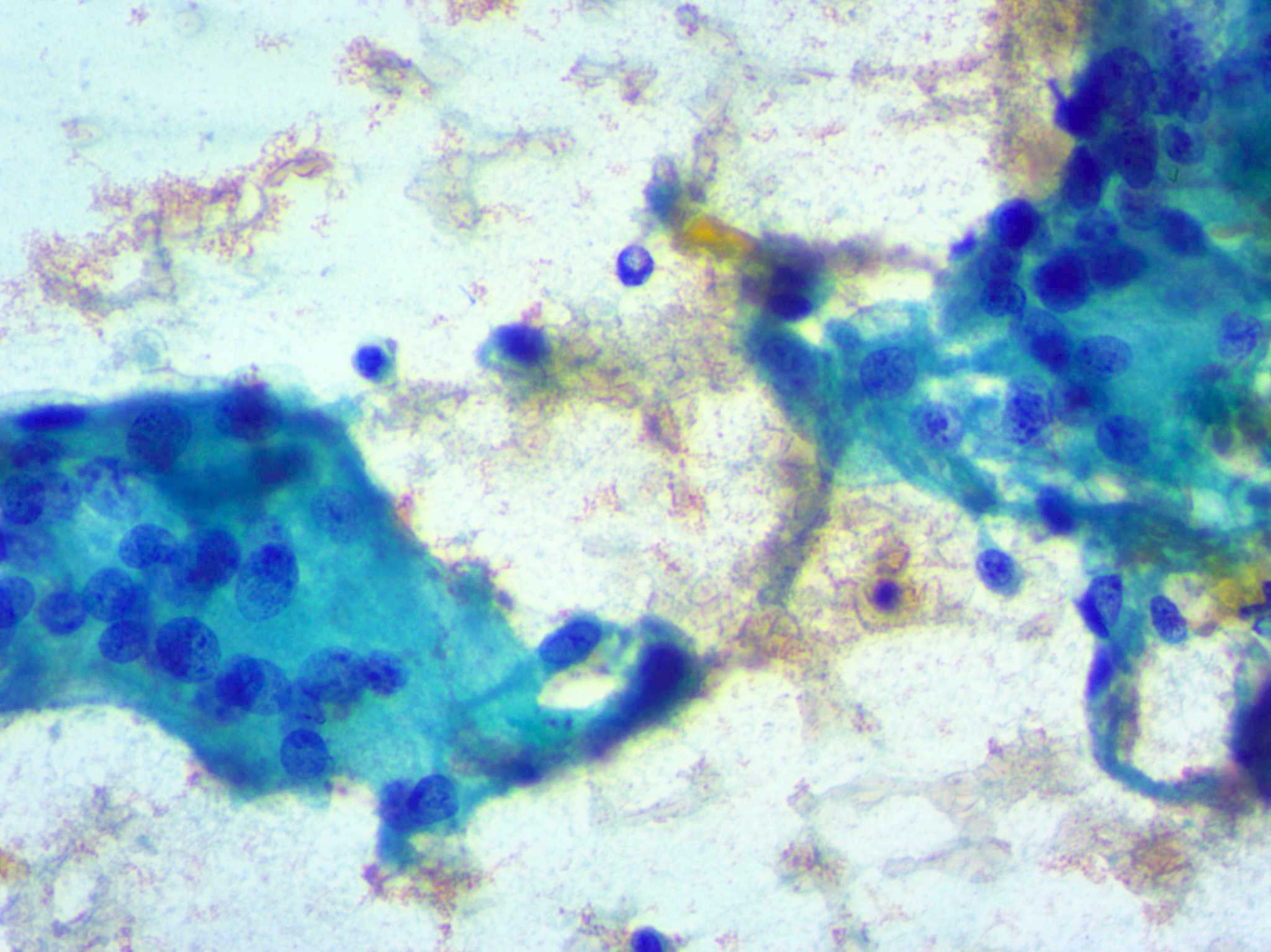
- Cellular smears with clustered epithelioid cells, fibrous fragments with enmeshed inflammatory cells, scattered lymphocytes, histiocytes and neutrophils, occasional multinucleated giant cells containing up to 100 nuclei and ingesting colloid or neutrophils (Ali: The Bethesda System for Reporting Thyroid Cytopathology, 2nd Edition, 2018, J Clin Diagn Res 2017;11:EC09)
- Cellular composition also depends on the stage
- Early stage: many neutrophils and eosinophils, similar to acute thyroiditis
- Later stages: hypocellular, giant cells surrounding and engulfing colloid, epithelioid cells, lymphocytes, macrophages and scant degenerated follicular cells (Diagn Cytopathol 2019;47:1251)
Cytology images
Contributed by Truong Phan Xuan Nguyen, M.D. and Ayana Suzuki, C.T.
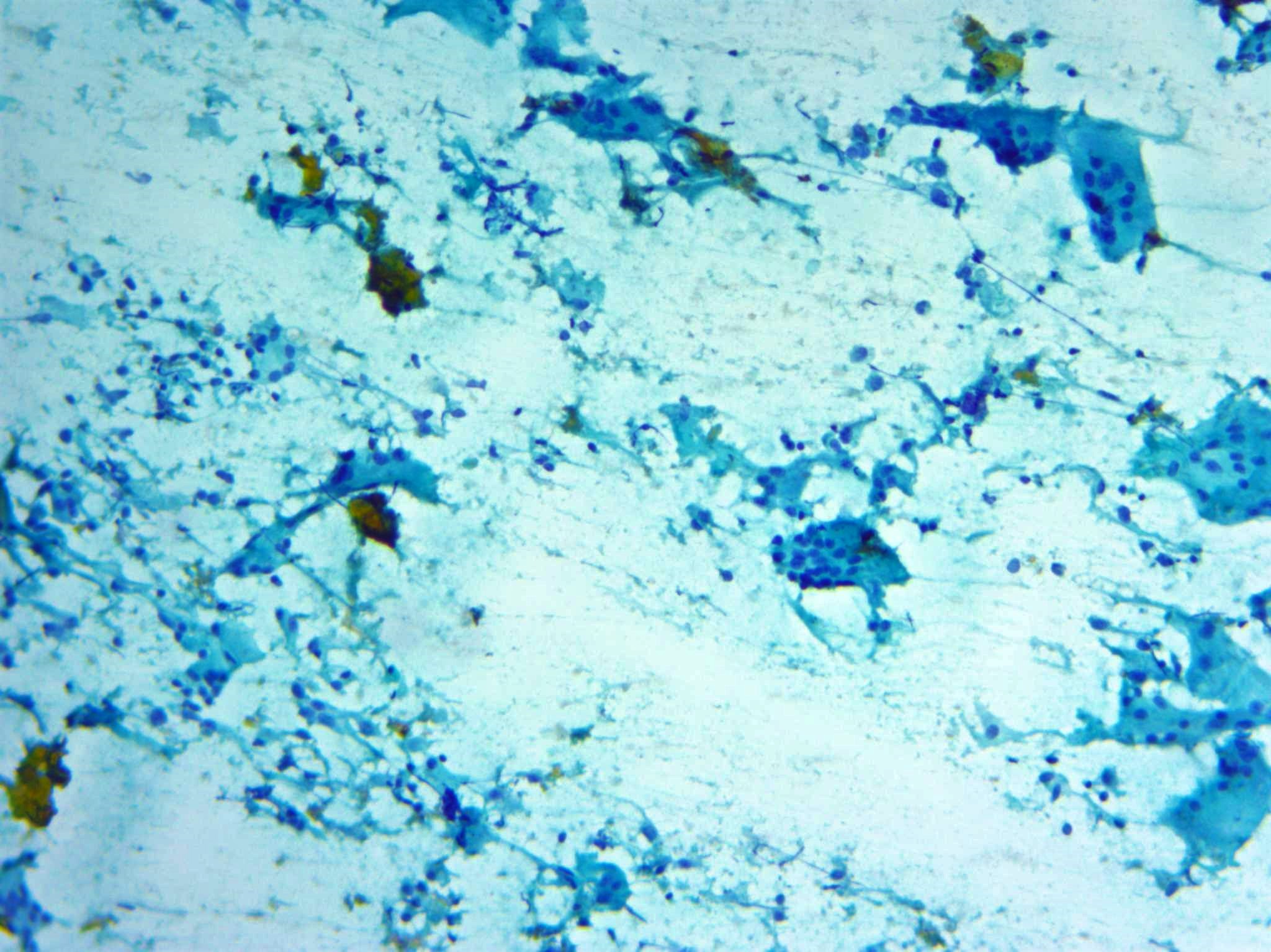
Cellular smear
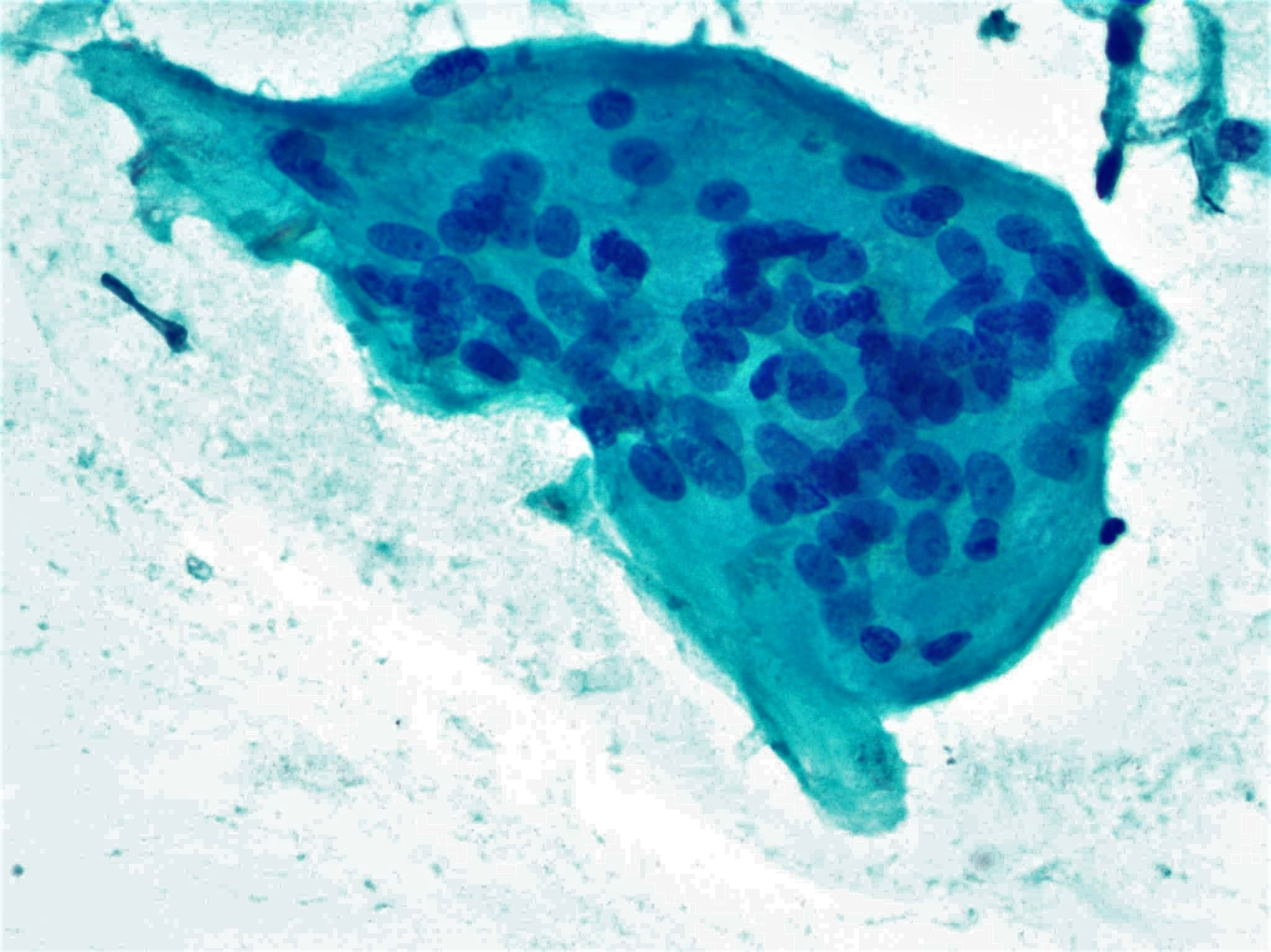
Multinucleated giant cells

Epithelioid cells
Giant cell
Positive stains
Sample pathology report
- Thyroid, left lobe, fine needle aspiration:
- Benign (Bethesda category II)
- Subacute thyroiditis (see comment)
- Comment: Moderately cellular aspirate with multinucleated giant cells, clustered epithelioid histiocytes, scattered lymphocytes and neutrophils consistent with subacute thyroiditis.
- Thyroid, completion thyroidectomy:
- Subacute thyroiditis (see comment)
- Comment: Marked inflammation with granulomas containing multinucleated giant cells and epithelioid histiocytes without caseation necrosis. Areas of fibrosis are patchily distributed. The findings are diagnostic of subacute thyroiditis.
Differential diagnosis
- Palpation thyroiditis:
- Also called multifocal granulomatous thyroiditis
- May be distributed throughout gland
- No neutrophils
- Multinucleated giant cells
- Sarcoidosis:
- Granulomas usually found in interstitium
- Small, compact aggregates of epithelioid histiocytes
- Giant cells may be present
- Necrosis tends to be absent
- Tuberculosis:
- Granulomas with caseation
- Granulation tissue and fibrosis
- AFB positive
- Chronic lymphocytic (Hashimoto) thyroiditis:
- Diffuse, nontender thyroid gland
- Primary features: oncocytic epithelium, lymphocytes, germinal centers
- Lacks follicle destruction and giant cells
- Thyroid primary and metastatic malignant tumors (BMC Endocr Disord 2019;19:86):
- Tumors sometimes imitate symptoms of subacute thyroiditis, which may lead to delayed diagnosis of the thyroid malignancy
- Neck sonography and thyroid FNA are helpful in identifying invasive growth and atypical malignant cells, respectively
Additional references
Board review style question #1
A 40 year old woman presented to her family physician with fatigue. Several weeks ago, she had a runny nose and cough. A physical examination reveals a tender thyroid gland. Laboratory testing reveals a TSH of 0.3 mIU/L and T3 of 5 nmol/L, T4 of 4.5 nmol/L. Of the following, what would a cytologic examination of the thyroid gland reveal?
- Abscesses
- Clear nuclei and psamomma bodies
- Clustered epithelioid cells and giant cells
- Lymphocyte and oncocytic change
- Small follicles
Board review style answer #1
C. Clustered epithelioid cells and giant cells. This case has clinical appearances and cytologic features of subacute thyroiditis.
Comment Here
Reference: Subacute thyroiditis
Comment Here
Reference: Subacute thyroiditis
Board review style question #2
A 45 year old woman reported 1 week symptoms of fatigue, fever, myalgias and neck pain. Neck examination demonstrates significant thyroid gland tenderness. Which histologic changes would likely accompany the above symptoms?
- Enlarged cells with large intranuclear inclusions
- Foreign material
- Granulomas with giant cells and epithelioid histiocytes
- Markedly atypical cells
- Papillae
Board review style answer #2
C. Granulomas made of giant cells and epithelioid histiocytes are a typical histologic feature of subacute thyroiditis.
Comment Here
Reference: Subacute thyroiditis
Comment Here
Reference: Subacute thyroiditis

