

Thyroid & parathyroid
Cytology
Bethesda system
AUS
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 21 April 2022
Last staff update: 12 December 2024 (update in progress)
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: Bethesda guidelines atypia
Table of Contents
Definition / general | Essential features | Terminology | Clinical features | Diagnosis | Case reports | Cytology description | Cytology images | Explanatory notes | Management | Sample pathology report | Videos | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Suzuki A, Bychkov A. AUS. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidatypia.html. Accessed December 16th, 2024.
Definition / general
- The Bethesda category III, Atypia of Undetermined Significance / Follicular Lesion of Undetermined Significance (AUS / FLUS) is used for cases with a minor degree of atypia, primarily cytologic or architectural in nature, insufficient to qualify for either of the suspicious categories (category IV and higher)
Essential features
- AUS / FLUS include cases with few cells that have distinct but mild nuclear atypia or with more extensive but very mild nuclear atypia
- Frequency 8%, resection rate 43.0 - 64.7%, risk of malignancy 10 - 30% of all nodules (6 - 18% after noninvasive follicular thyroid neoplasm with papillary-like nuclear features exclusion) and up to 40% of resected nodules
- The most common histopathological diagnosis of AUS nodules is nodular hyperplasia and follicular adenoma, followed by papillary thyroid carcinoma (PTC)
- Repeat fine needle aspiration (FNA) results in a more definitive cytologic interpretation (70 - 90%)
Terminology
- AUS: preferred term
- FLUS: acceptable alternative for the cases with the atypia of follicular cell origin
- Laboratory should choose the one preferable term and use it exclusively for this category
- AUS can be subdivided into AUS with cytologic (AUS-C) and architectural (AUS-A) atypia, which have different risk of malignancy (AUS-C > AUS-A)
- AUS-C: mostly benign appearing with mild cytologic / nuclear atypia (also called AUS-N)
- AUS-A: cannot be denied a possibility of follicular neoplasm (applicable to FLUS), see Explanatory notes below
Clinical features
- Frequency: 8% in meta analysis (Expert Rev Endocrinol Metab 2014;9:97)
- AUS / FLUS is considered as the last resort after excluding all the rest of the Bethesda categories
- Goal is to have 7 - 10% (Cancer Cytopathol 2015;123:713) and ideally AUS / malignant ratio should not exceed 3:1 (Cancer Cytopathol 2012;120:111) – used as quality control criteria
- Resection rate: 43.0 - 64.7% (Thyroid 2014;24:832, Arch Pathol Lab Med 2013;137:1664)
- Risk of malignancy (ROM): 10 - 30% (Ali: The Bethesda System for Reporting Thyroid Cytopathology - Definitions, Criteria, and Explanatory Notes, 2nd Edition, 2018, Cancer Cytopathol 2012;120:111)
- Cytologic (nuclear) atypia > architectural atypia (Acta Cytol 2011;55:518)
- Hürthle cell type AUS / FLUS < other AUS / FLUS patterns (Acta Cytol 2011;55:518)
- 6 - 18% when noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) is implicated (Ali: The Bethesda System for Reporting Thyroid Cytopathology - Definitions, Criteria, and Explanatory Notes, 2nd Edition, 2018, Cancer Cytopathol 2012;120:111)
Diagnosis
- Aspirates containing cells (follicular, lymphoid or other) with architectural or nuclear atypia that is not sufficient to be classified as suspicious for a follicular neoplasm, suspicious for malignancy or malignant (Ali: The Bethesda System for Reporting Thyroid Cytopathology - Definitions, Criteria, and Explanatory Notes, 2nd Edition, 2018)
- Atypia is more marked than can be ascribed confidently to benign changes
Case reports
- 36 year old woman with primary sclerosing paraganglioma of the thyroid (Ann Otol Rhinol Laryngol 2012;121:510)
- 47 year old woman with IgG4-related disease of the thyroid (Head Neck Pathol 2018 May 31 [Epub ahead of print])
- 60 year old woman with aggressive PTC (Thyroid 2015;25:1375)
- 74 year old man with metastatic clear cell renal cell carcinoma to the thyroid (Diagn Cytopathol 2017;45:161)
Cytology description
- Cytologic atypia
- Can be focal or can show most cells with mild cytologic atypia
- Most of the aspirate appears benign but rare cells have:
- Nuclear enlargement
- Pale chromatin
- Irregular nuclear contours
- No nuclear pseudoinclusions
Cytology images
Contributed by Ayana Suzuki, C.T.
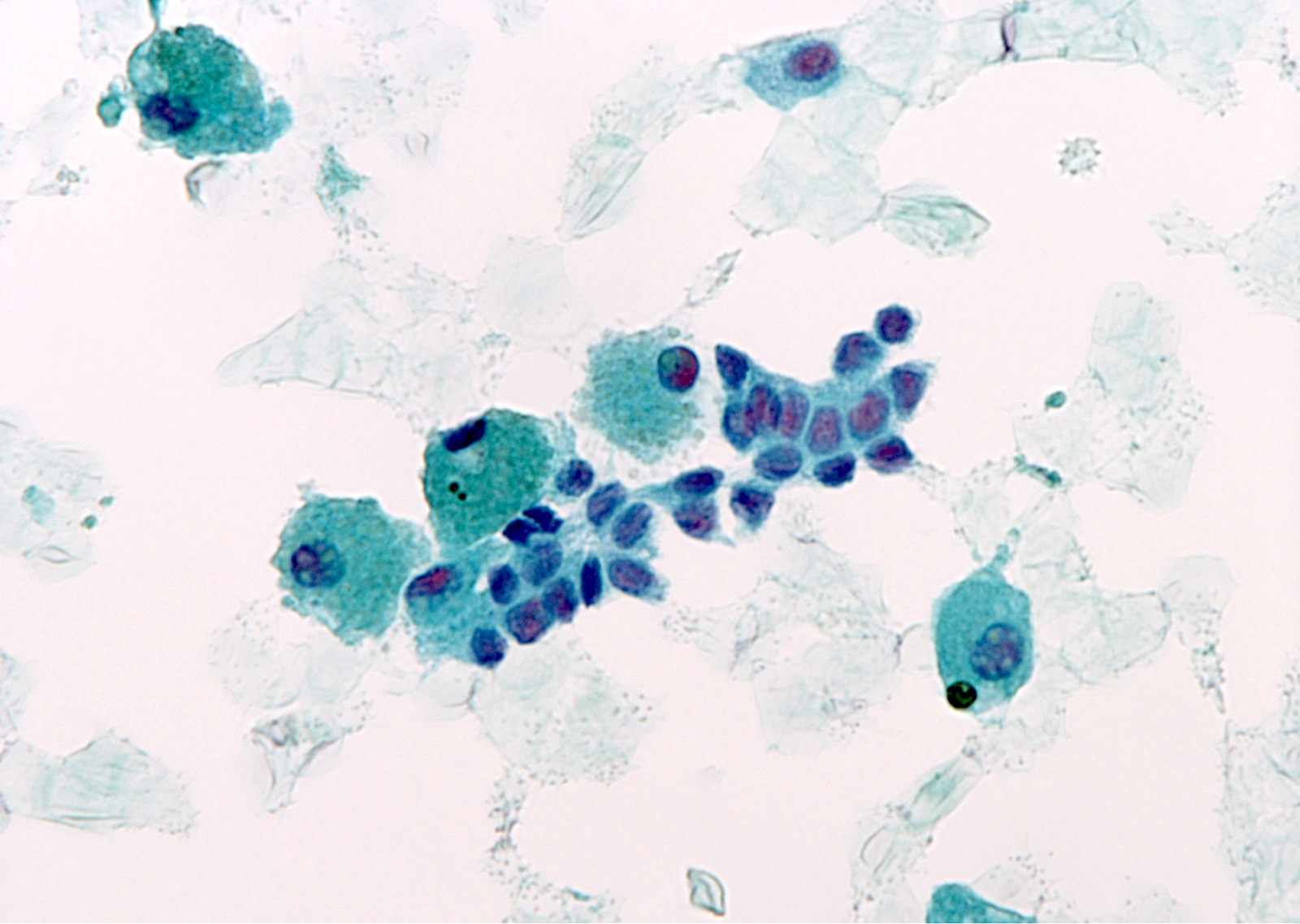
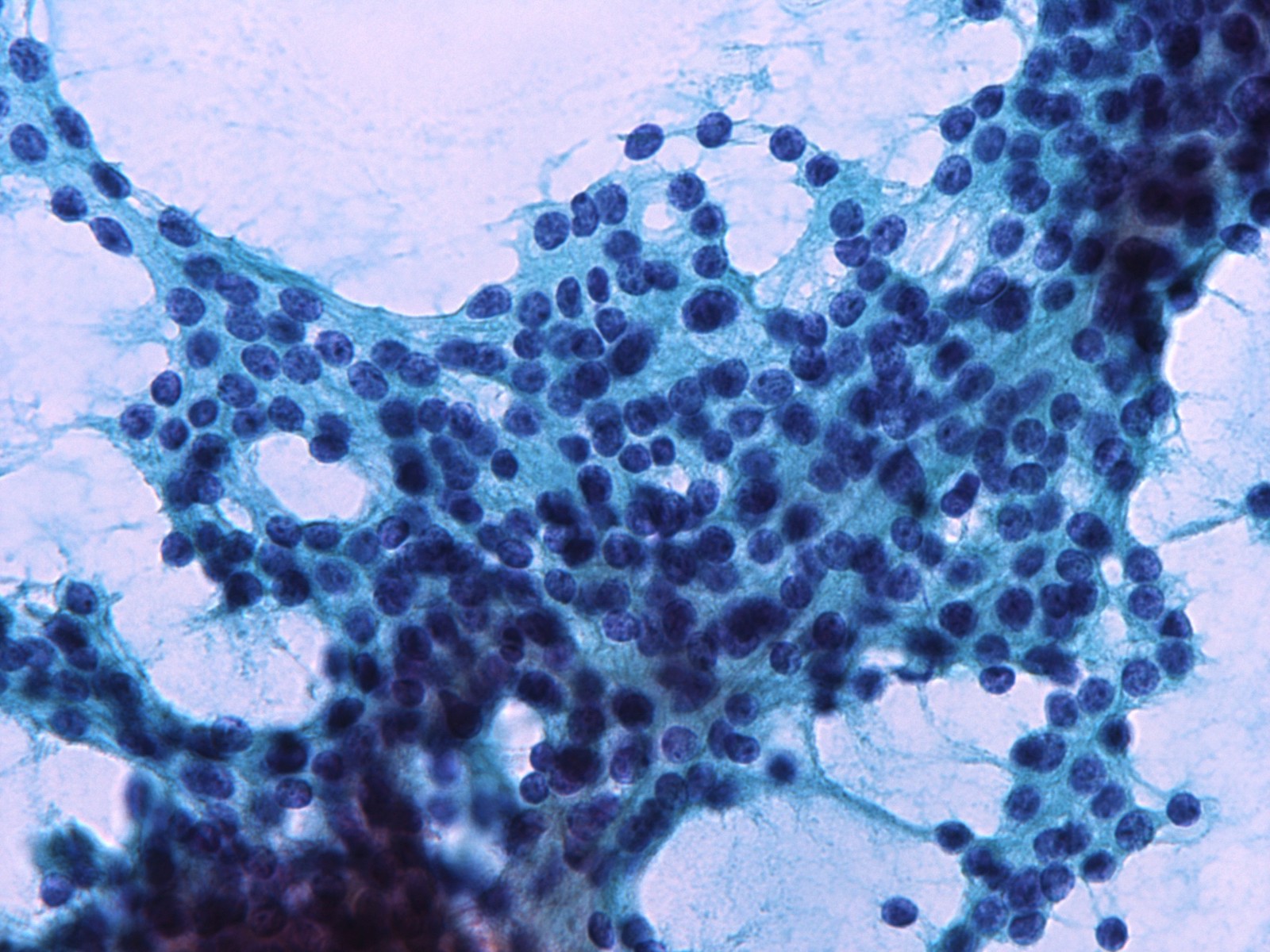
Cytologic atypia
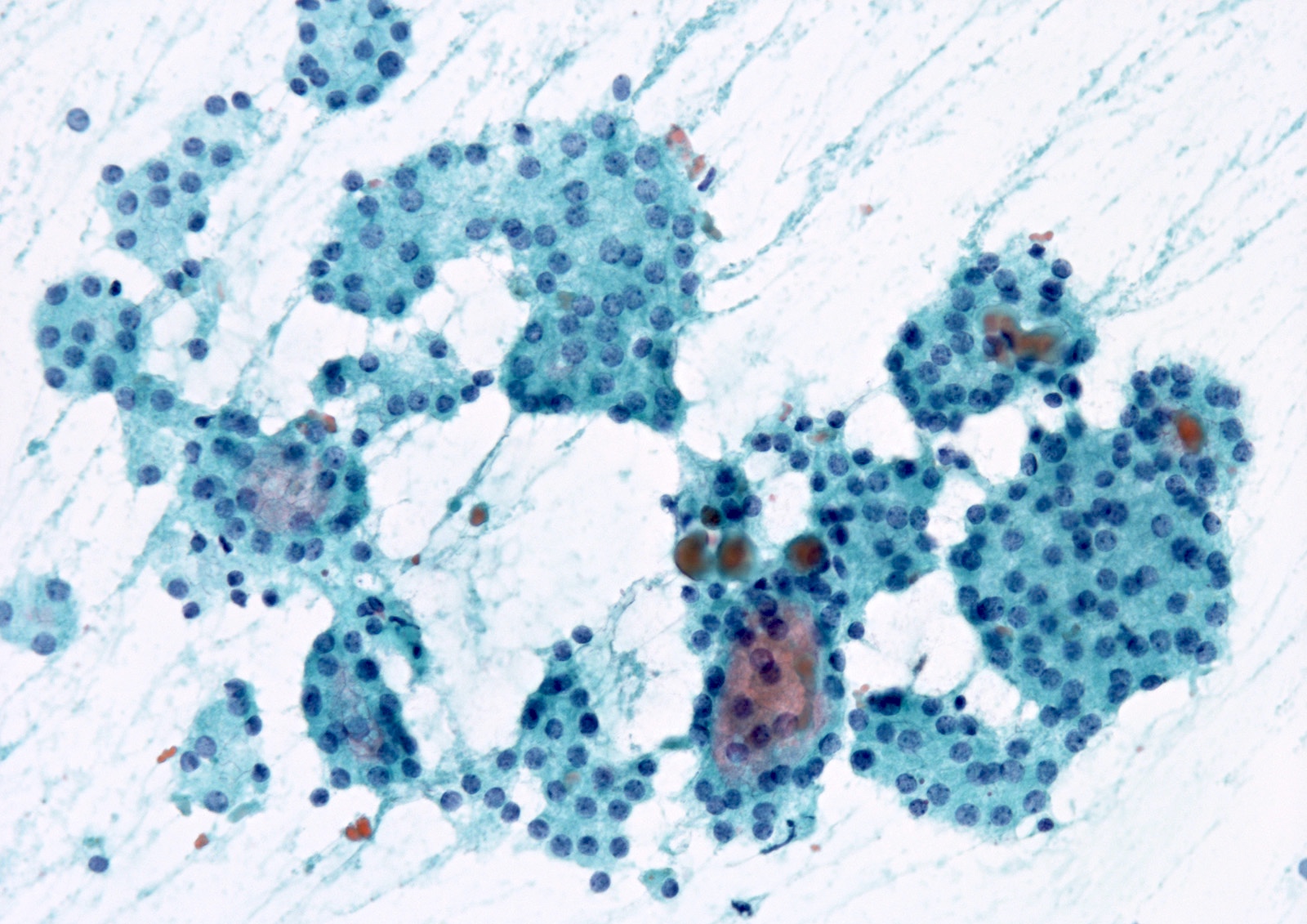
Architectural atypia
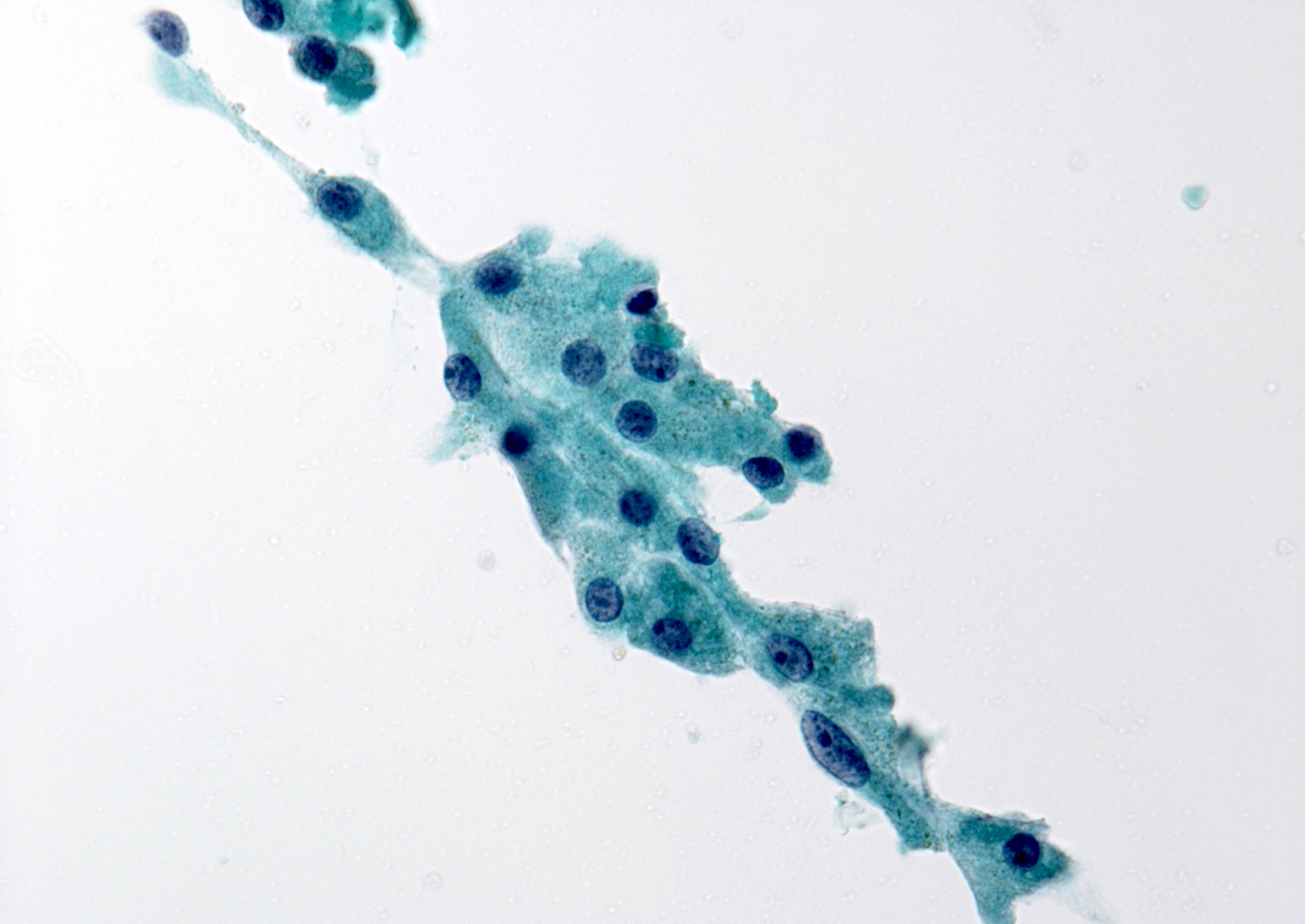
Hürthle cell atypia
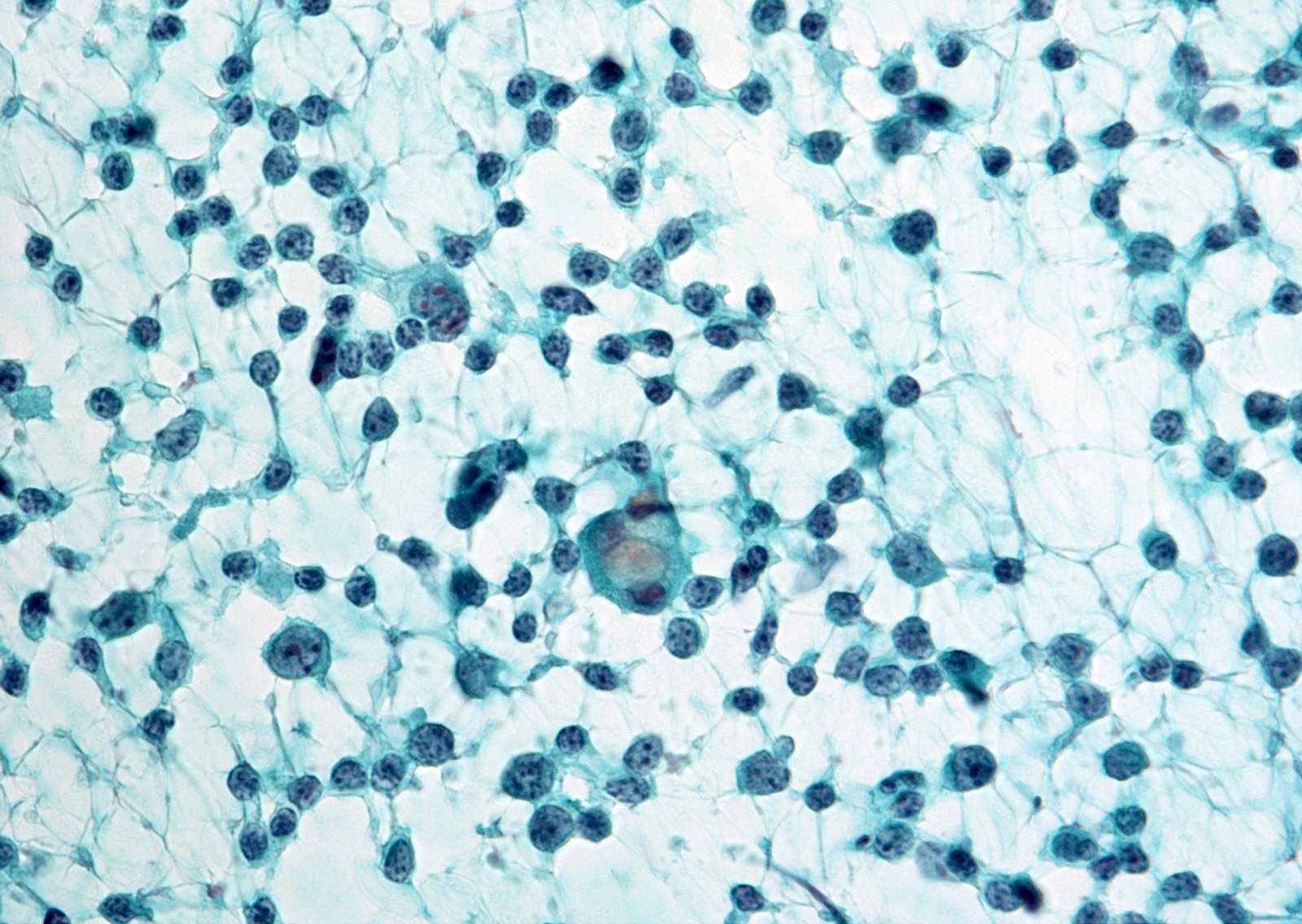
Atypical lymphocytes
Images hosted on other servers:




Cytologic atypia



Atypical cyst lining cells

Architectural atypia

Atypical lymphocytes
Explanatory notes
- AUS / FLUS is an interpretation of last resort and should be used judiciously
- Specimen preparation artifacts may potentially raise concern for AUS / FLUS
- AUS with cytologic atypia is associated with PTC (28 - 56%) (Am J Clin Pathol 2011;136:572, Diagn Cytopathol 2012;40:410)
- Rare cells (< 20 cells) with enlarged, often overlapping, nuclei, pale chromatin, irregular nuclear outlines and nuclear grooves
- Well defined, intranuclear pseudoinclusions or psammomatous calcifications (more suspicious) (Acta Cytol 2008;52:320)
Management
- 2015 American Thyroid Association Management Guidelines recommend either repeat FNA or molecular testing (Thyroid 2016;26:1)
- About half of AUS / FLUS cases have a negative Afirma gene expression classifier (GEC) result (architectural atypia > cytologic atypia)
- Hürthle cell pattern of AUS / FLUS has a lower rate of GEC benign results despite its very low risk of malignancy (Thyroid 2015;25:789)
- Surgery versus continued observation is based on a synthesis of cytologic, molecular, clinical and radiologic findings as well as clinical risk factors and patient preference
- Noninvasive follicular thyroid neoplasm with papillary-like nuclear features will diminish the overall risk of malignancy for AUS / FLUS (Thyroid 2015;25:987, Cancer Cytopathol 2016;124:181)
Sample pathology report
- Dx/Category: Atypia of undetermined significance (AUS), a possibility of follicular neoplasm.
Sparsely cellular aspirate comprised of follicular cells with microfollicular pattern colloid is absent.
- Note: A repeat FNA or molecular testing may be helpful if clinically indicated.
- Dx/Category: Atypia of undetermined significance (AUS), a possibility of papillary thyroid carcinoma.
Follicular cells with mild nuclear irregularity.
- Note: A repeat FNA or molecular testing may be helpful if clinically indicated.
- Dx/Category: Atypia of undetermined significance (AUS), a possibility of papillary thyroid carcinoma.
Follicular cells, predominantly benign appearing, with focal cytologic atypia.
- Note: A repeat FNA or molecular testing may be helpful if clinically indicated.
- Dx/Category: Atypia of undetermined significance (AUS), a possibility of lymphoma.
Numerous relatively monomorphic lymphoid cells.
- Note: An additional aspiration, with apportioning of needle wash out fluid for flow cytometry, may be helpful if clinically indicated.
Videos
Atypical thyroid FNA
Head and tail of the Bethesda system for thyroid
Thyroid cytology - Bethesda classification
Differential diagnosis
-
Extensive but mild cytologic atypia
- Many if not most cells have mildly enlarged nuclei with:
- Slightly pale chromatin
- Only limited nuclear contour irregularity
- No nuclear pseudoinclusions
-
Atypical cyst lining cells
- Cyst lining cells may appear atypical (rare cases) such as:
- Nuclear grooves
- Prominent nucleoli
- Elongated nuclei and cytoplasm
- Rare intranuclear pseudoinclusions
- Associated with hemosiderin laden macrophages
- Reactive follicular or mesenchymal cells associated with cystic degeneration of thyroid nodules
- Most cases are benign (Cancer 2005;105:71)
-
Histiocytoid cells
- Compared with histiocytes:
- Larger
- Rounder nuclei
- Higher nuclear to cytoplasmic ratio
- Harder (glassier) cytoplasm
- Larger, discrete vacuoles without the hemosiderin or microvacuolization of histiocytes
- Characteristic of cystic PTC (Cancer 2002;96:240)
- Immunostaining: keratins (PTC cells), CD68 (histiocytes)
-
Architectural atypia
- Rare clusters with microfollicles or crowded three dimensional groups with scant colloid
- Low risk
- Follicular neoplasm / suspicious for a follicular neoplasm (FN / SFN) diagnosis if the specimen were more cellular
-
Focally prominent microfollicles with minimal nuclear atypia
- A more prominent than usual population of microfollicles but not sufficient for a diagnosis of FN / SFN
- Should not be confused with an overall mixed but predominantly macrofollicular, aspirate (benign)
-
Cytologic and architectural atypia
- The presence of both mild cytologic and architectural atypia may be more common with noninvasive follicular thyroid neoplasm with papillary-like nuclear features
-
Hürthle cell aspirates
- A sparsely cellular aspirate comprised of Hürthle cells with minimal colloid
- Very low risk
- Follicular neoplasm, Hürthle cell type / suspicious for a follicular neoplasm, Hürthle cell type diagnosis if the specimen were highly cellular
-
Markedly cellular sample composed of Hürthle cells with sparse colloid, yet the clinical setting suggests benign
- Clinically suggesting lymphocytic thyroiditis or a multinodular goiter
- More highly predictive of a hyperplastic Hürthle cell nodule than usual (Am J Clin Pathol 2011;135:139)
- Hürthle cells are all in cohesive flat sheets without nuclear atypia and there is abundant colloid → benign (in the absence of high risk clinical or radiologic findings)
- To follow a patient rather than perform a lobectomy will often be based on clinical and sonographic correlation
-
Atypia, not otherwise specified (NOS)
- A minor population of follicular cells with nuclear enlargement and prominent nucleoli
- Does not raise concern for PTC and best classified as NOS
- Specimens from patients with a history of radioactive iodine, carbimazole or other pharmaceutical agents can usually be diagnosed as benign
-
Psammomatous calcifications in the absence of nuclear features of PTC
- Psammoma bodies raise concern for PTC and should prompt careful scrutiny of PTC cells
- Lamellar bodies of inspissated colloid may be indistinguishable from true psammomatous calcifications
-
Atypical lymphoid cells, rule out lymphoma
- There is an atypical lymphoid infiltrate but the degree of atypia is insufficient for suspicious for malignancy
- Repeat aspirate for flow cytometry is desirable
-
Parathyroid lesion
- Crowded three dimensional clusters or trabecular arrangements, abundant granular cytoplasm, salt and pepper chromatin (Head Neck 2002;24:157, Acta Cytol 2004;48:133)
- 25 - 30% of parathyroid lesions can be recognized
- Immunohistochemistry (GATA3, PTH, chromogranin A) and ancillary studies (parathyroid hormone assays, molecular studies) can confirm the diagnosis
-
Descriptive language may occasionally influence management
- Scant or poorly preserved → Repeat aspirate
- Follow up of a cellular, well preserved aspirate with diffuse mild atypia → Molecular testing
Board review style question #1
- Which case belongs to architectural atypia?
- A sparsely cellular aspirate comprised of Hürthle cells with minimal colloid
- Atypical lymphoid cells
- Focally prominent microfollicles with minimal nuclear atypia
- Most of the aspirate appears benign but rare cells have irregular nuclear contours
- Psammomatous calcifications in the absence of nuclear features of PTC
Board review style answer #1
C. Focally prominent microfollicles with minimal nuclear atypia. Microfollicles are architectural atypia suggesting follicular neoplasm.
Comment Here
Reference: Atypia of undetermined significance / follicular lesion of undetermined significance
Comment Here
Reference: Atypia of undetermined significance / follicular lesion of undetermined significance
Board review style question #2
- A 70 year old man underwent FNA for the nodule of the thyroid right lobe. A cytological image of the lesion is shown.
Which marker would most likely show positive staining?
- PAX8
- Calcitonin
- GATA3
- Thyroglobulin
- TTF1
Board review style answer #2
C. GATA3. This is intrathyroidal parathyroid adenoma.
Comment Here
Reference: Atypia of undetermined significance / follicular lesion of undetermined significance
Comment Here
Reference: Atypia of undetermined significance / follicular lesion of undetermined significance

