

Testis & paratestis
Nonneoplastic lesions
Sertoli cell nodule
Authors: Julia Rivera, M.D., Ritu Bhalla, M.D.
Resident / Fellow Advisory Board: Alcino Pires Gama, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 24 November 2023
Last staff update: 24 November 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Sertoli cell nodule
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Rivera J, Bhalla R. Sertoli cell nodule. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/testissertolihyperplasia.html. Accessed April 18th, 2024.
Definition / general
- Nonneoplastic proliferation of immature Sertoli cells within seminiferous tubules
- Included in the spectrum of testicular dysgenesis syndrome (Clin Endocrinol (Oxf) 2009;71:459, MacLennan: Urologic Surgical Pathology, 4th Edition, 2019)
Essential features
- Usually an incidental finding in adult testis
- Commonly seen in cryptorchid testis, also identified in normal testis
- Nodule size usually varies from microscopic to 5 mm; rarely can reach up to 10 mm
- Comprised of seminiferous tubules containing proliferation of immature Sertoli cells
Terminology
- Sertoli cell hyperplasia
- Tubular dysgenesis
- Hypoplastic zones
- Pick adenoma
ICD coding
- ICD-10: D29.20 - benign neoplasm of unspecified testis
Epidemiology
- Identified in adults with
- Cryptorchid testis (~60%)
- Normal scrotal testes (~22%)
- Occasionally in infertile testis
- Adjacent to germ cell tumor (MacLennan: Urologic Surgical Pathology, 4th Edition, 2019)
Sites
- Testes
Pathophysiology
- Exact pathophysiology of Sertoli cell nodules is unknown
- Proliferation of Sertoli cells has been identified in the setting of
- Sexually immature testis
- Sertoli cells are mitotically active in sexually immature testis and their numbers remain stable in adults (Am J Anat 1957;100:241)
- Developmental arrest of seminiferous tubules
- Lack of lengthening of tubules prevents the distribution of Sertoli cells (J Clin Pathol 2004;57:802, Hum Pathol 1982;13:3)
- Sexually immature testis
- Presence of immature Sertoli cells in cryptorchid testes could be explained by different factors including
- Increased temperature of the undescended testes
- Association with congenital lesions
- Hormonal influences (J Clin Pathol 2004;57:802, Hum Pathol 1982;13:3)
Etiology
- Primary testicular lesion
- Seen within the spectrum of testicular dysgenesis syndrome
- Proliferation of seminiferous tubules which are unable to undergo pubertal development
- Reference: Clin Endocrinol (Oxf) 2009;71:459
Clinical features
- Usually asymptomatic and an incidental finding (Am J Surg Pathol 2010;34:1874)
- Macroscopic lesions can present as a palpable testicular mass or firmness, testicular pain and as a visible mass on ultrasound (Am J Surg Pathol 2010;34:1874)
Diagnosis
- Usually an incidental finding on histological examination
Laboratory
- No significant laboratory findings
Radiology description
- Ultrasound imaging may show a nonspecific hyperechogenic lesion (J Clin Pathol 2006;59:1223)
Radiology images
Contributed by Raman Danrad, M.D.

Ultrasound of left testis
Prognostic factors
- Sertoli cell nodules have no malignant potential (J Clin Pathol 2006;59:1223)
- Presence of Sertoli cell nodules in a testicular biopsy is an adverse prognostic sign for fertility (MacLennan: Urologic Surgical Pathology, 4th Edition, 2019)
- Spontaneous regression may occur with increasing age (J Clin Pathol 2006;59:1223)
Case reports
- 21 year old man with lower left abdomen pain for 10 months (IAIM 2017;4:64)
- 31 year old man with right inguinal pain and undescended testis (Grand J Urol 2022;2:33)
- 33 year old man with a painless, right testicular firmness (J Clin Pathol 2006;59:1223)
Treatment
- Incidental finding; hence, no further intervention is necessary after histologic diagnosis (Am J Surg Pathol 2010;34:1874)
Gross description
- Well circumscribed, white-tan to yellow-tan nodules
- Size ranges from microscopic to 5 mm; may reach up to 10 mm (referred to as macroscopic)
- Can be single or multiple
- Firm to gelatinous
- References: Am J Surg Pathol 2010;34:1874, Pathol Res Pract 2016;212:943, J Clin Pathol 2006;59:1223
Gross images
Images hosted on other servers:

Demarcated, bulging, pale yellowish nodules

Sharply demarcated, yellowish white nodule
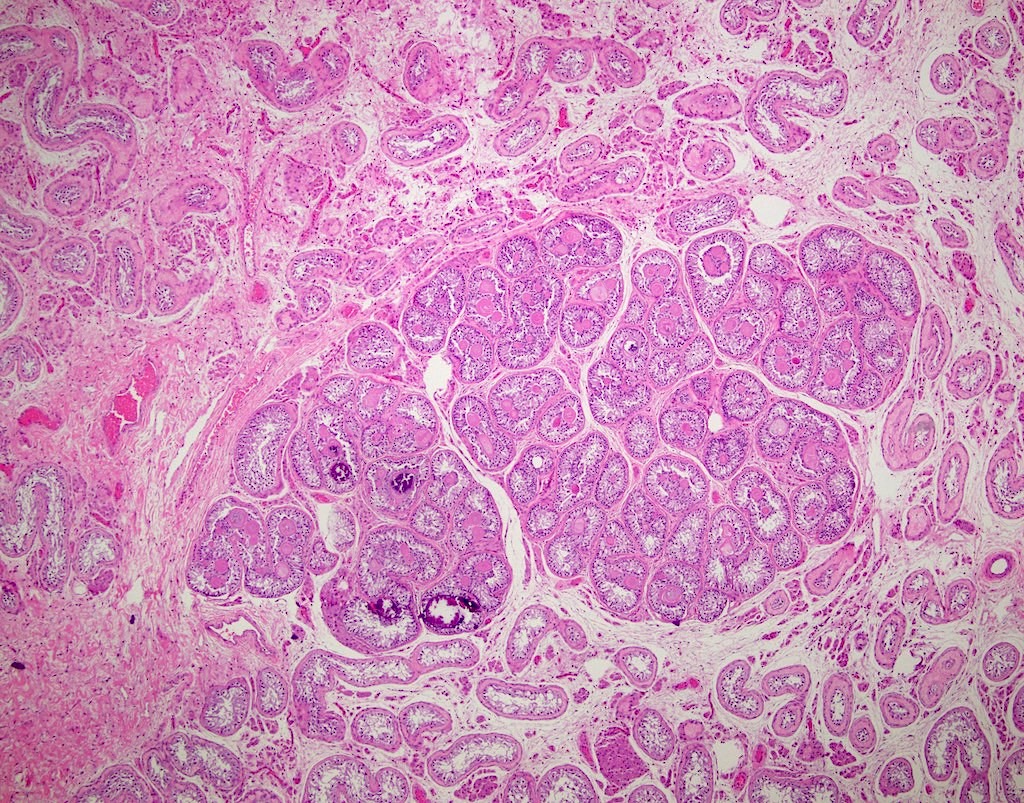
Microscopic (histologic) description
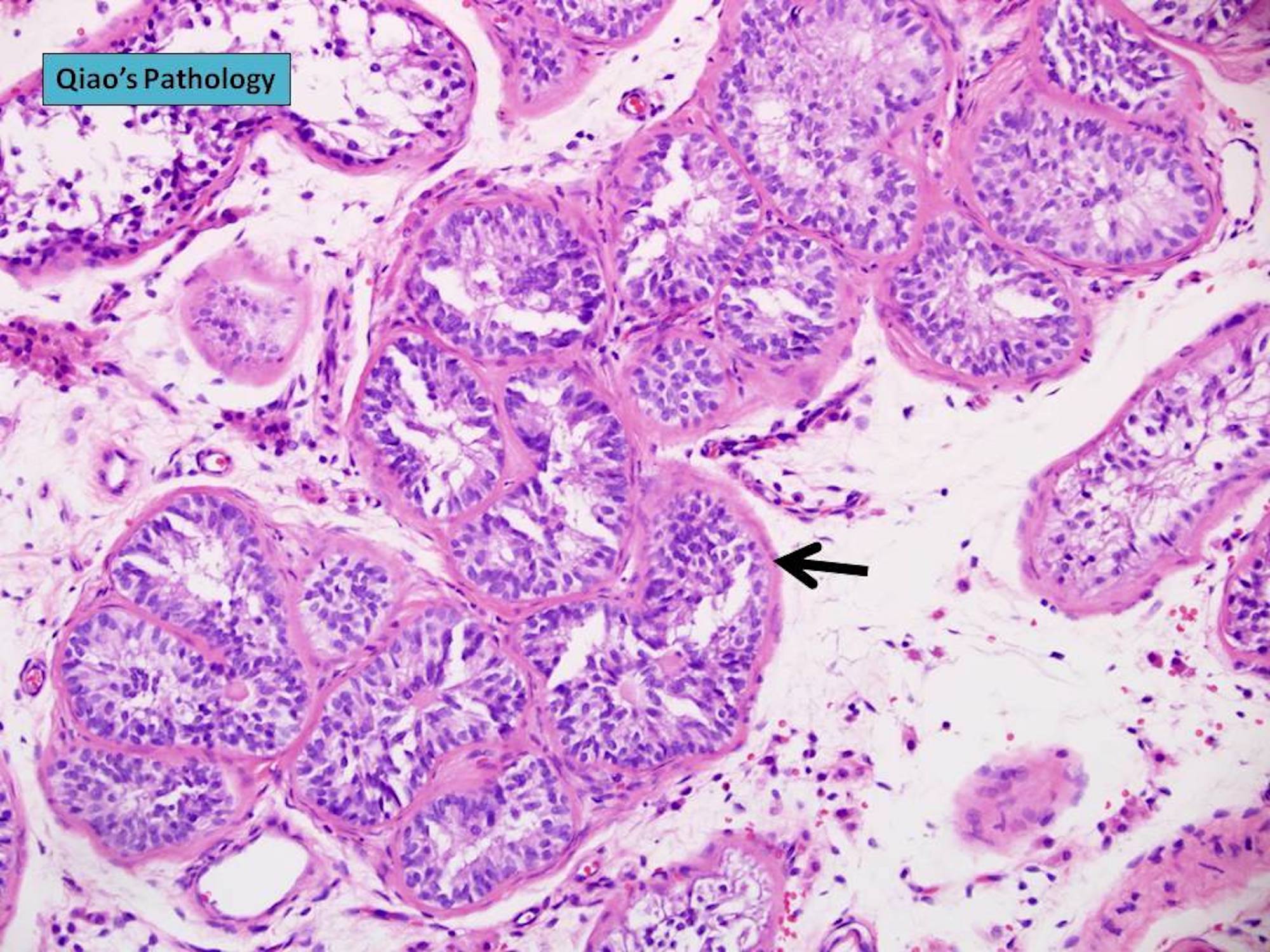
- Circumscribed, unencapsulated nodules, comprised of
- Prepubertal sized seminiferous tubules
- Profiles of tubules vary from round to oval to hourglass in shape
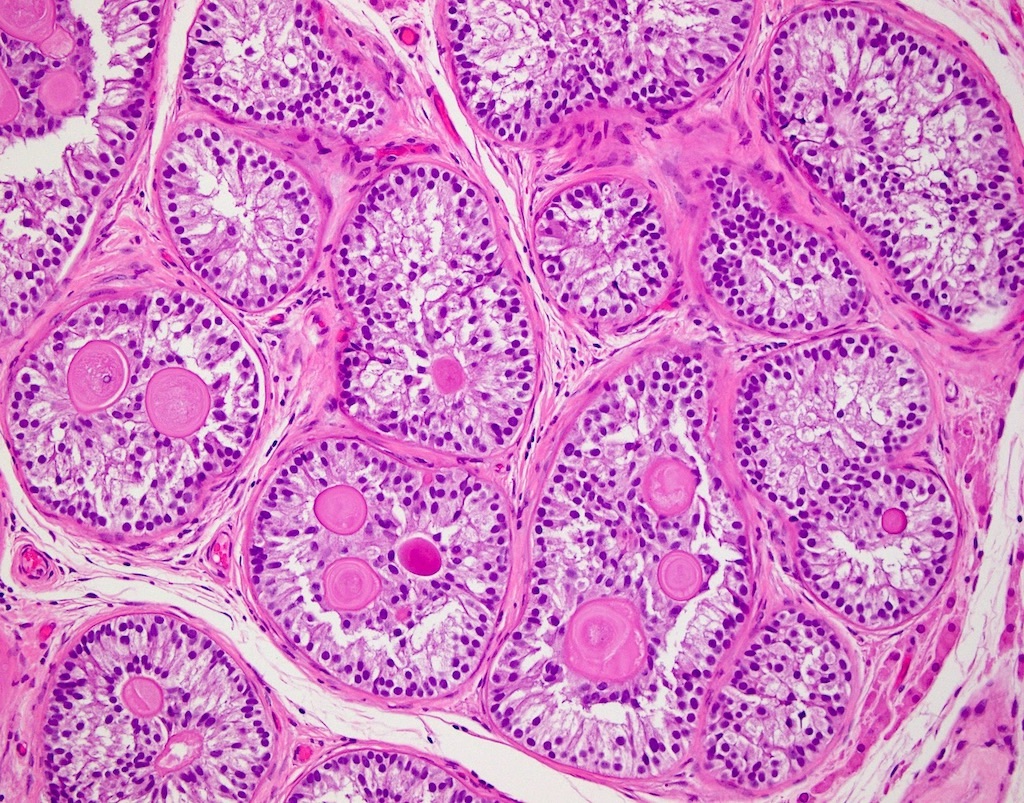
- Lined by columnar to pseudostratified epithelium composed of Sertoli cells with elongated, hyperchromatic nuclei, 1 or more peripherally located nucleoli and scant cytoplasm
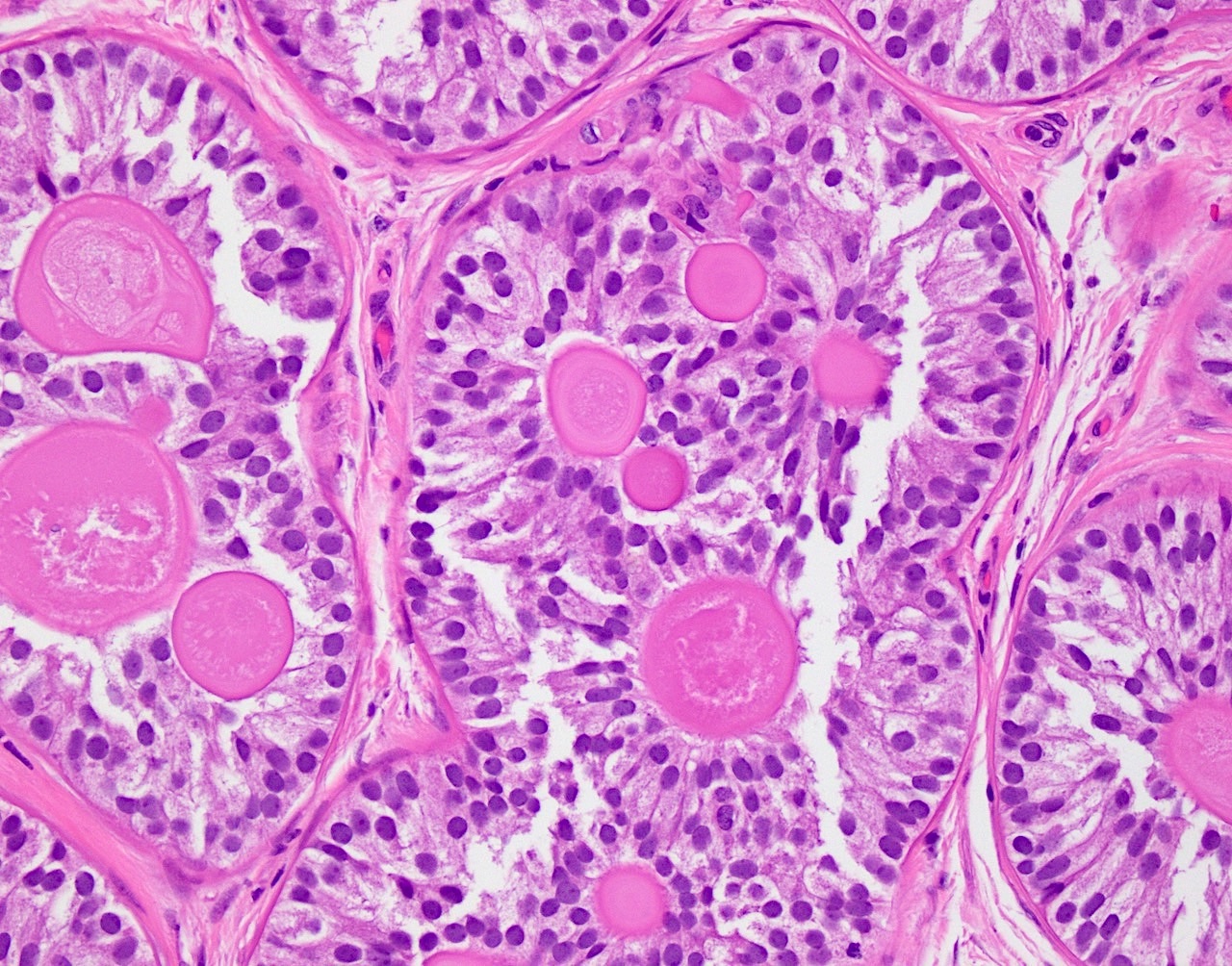
- Tubules are devoid of lumina; however, may contain globular hyaline material deposits, due to invagination of the excess basal lamina produced by Sertoli cells
- Sertoli cells can be arranged in a ring shaped manner around the hyaline material
- Basal lamina (basement membrane) type material may undergo calcification
- Isolated spermatogonia may be observed in some nodules
- Interstitium varies from scant to well collagenized
- Leydig cells are usually absent or low in numbers
- References: MacLennan: Urologic Surgical Pathology, 4th Edition, 2019, Am J Surg Pathol 2010;34:1874, J Clin Pathol 2004;57:802
Microscopic (histologic) images
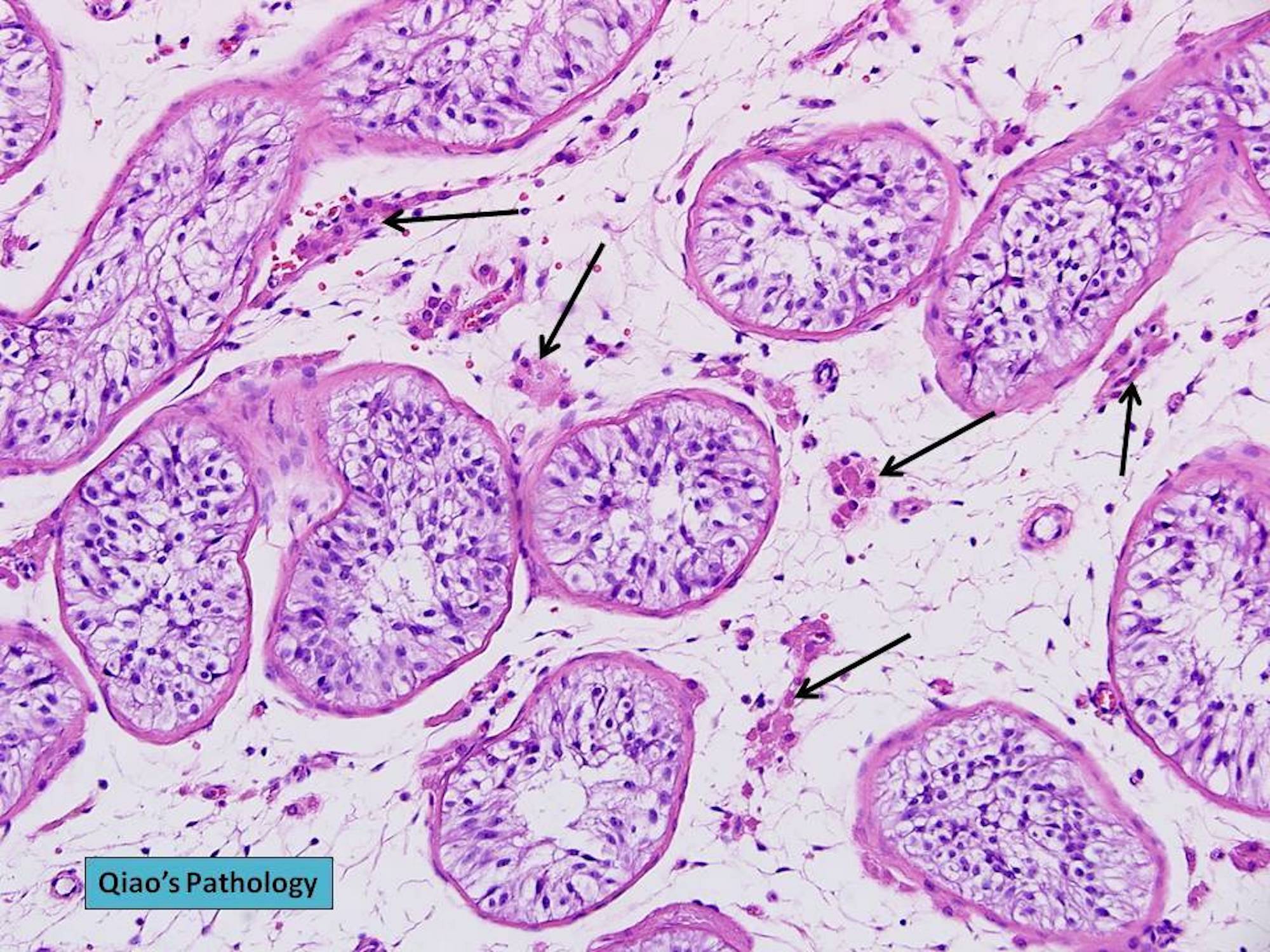
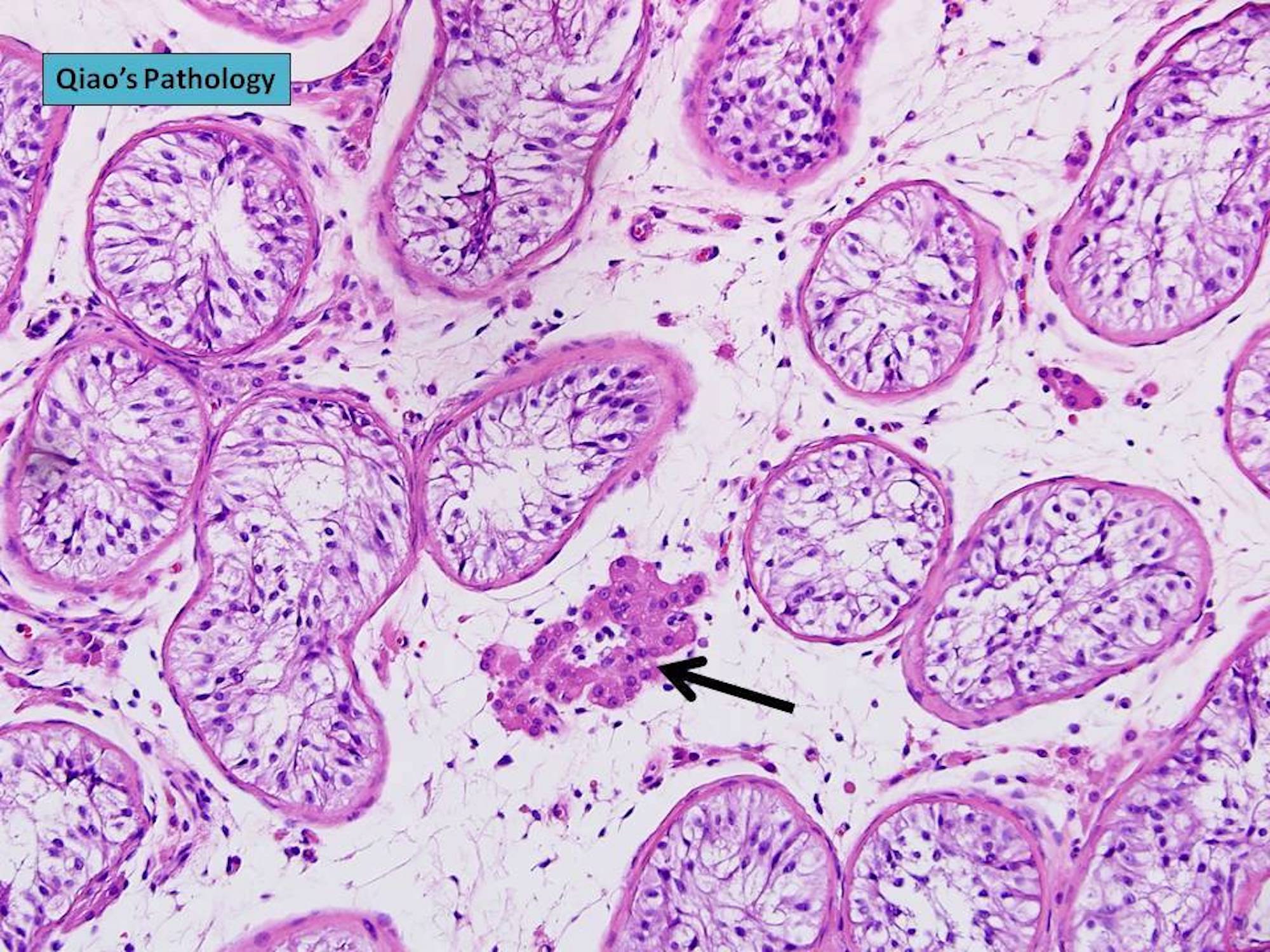
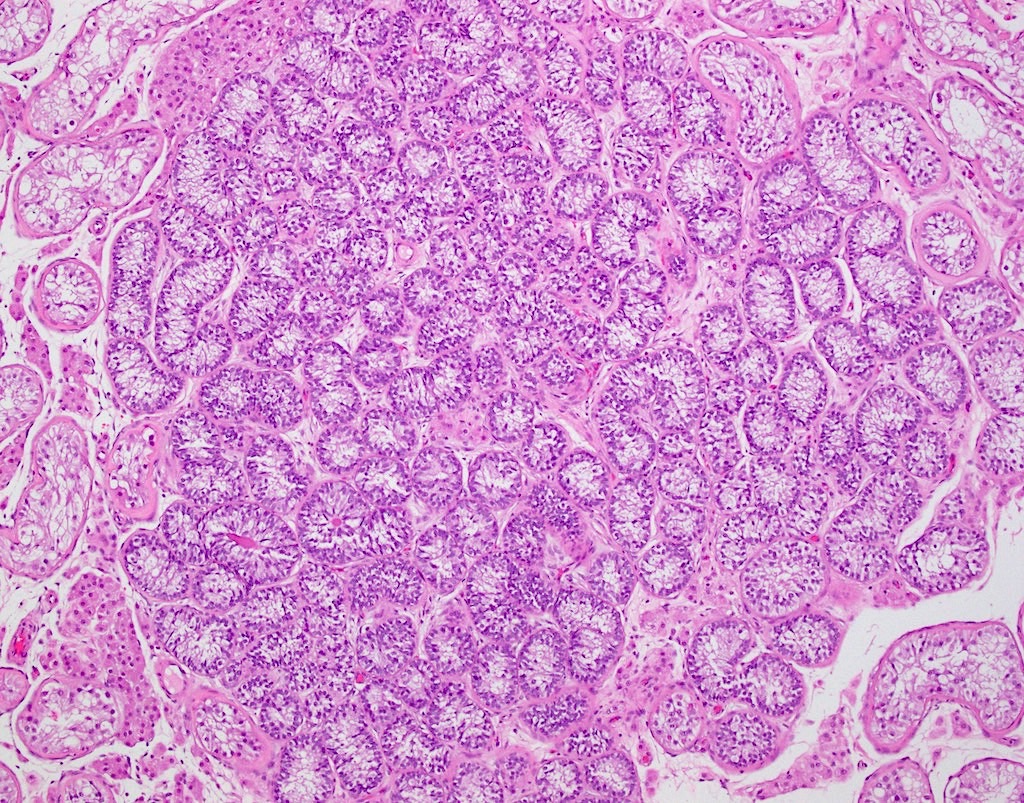
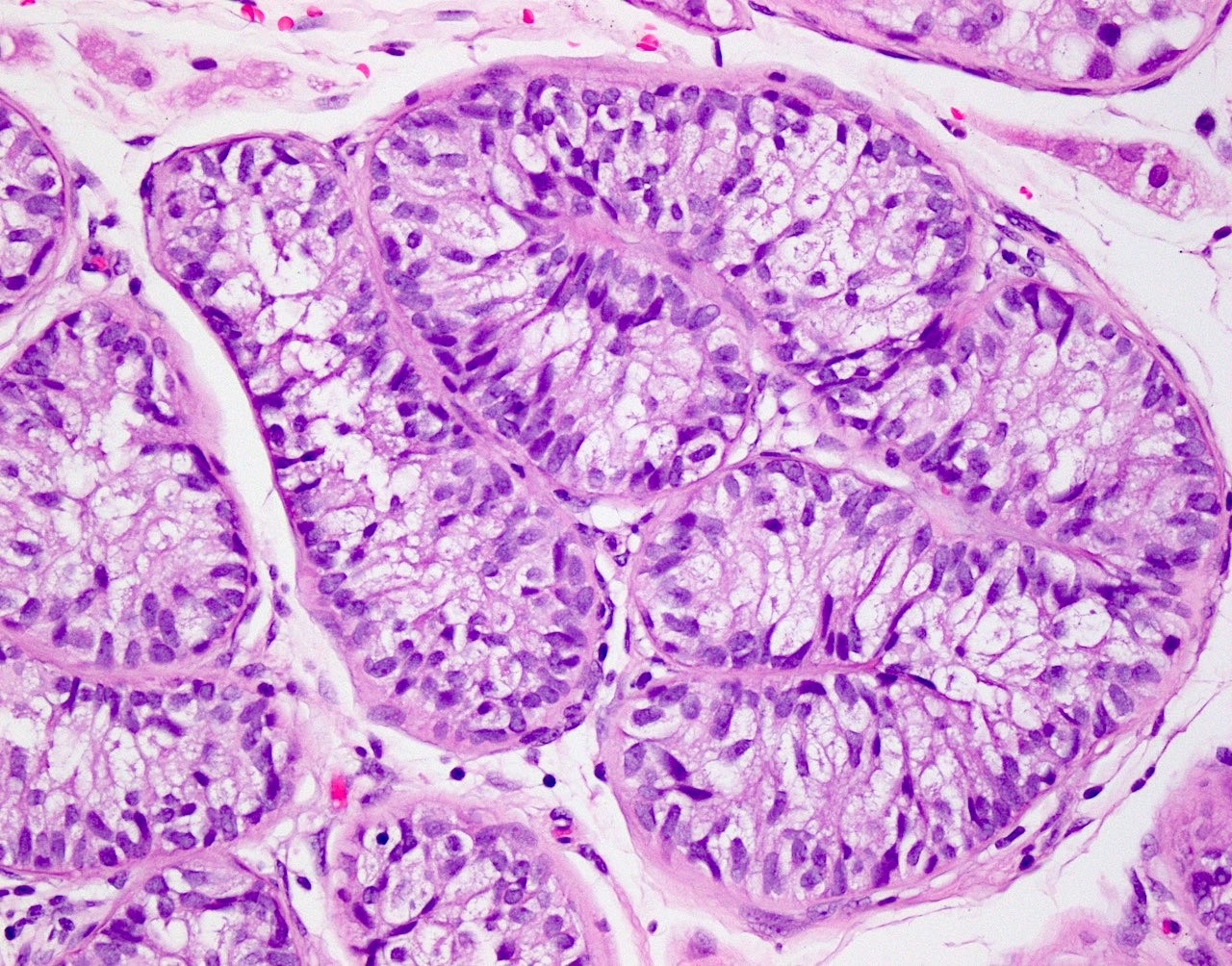
Contributed by Ritu Bhalla, M.D. and Jian-Hua Qiao, M.D.
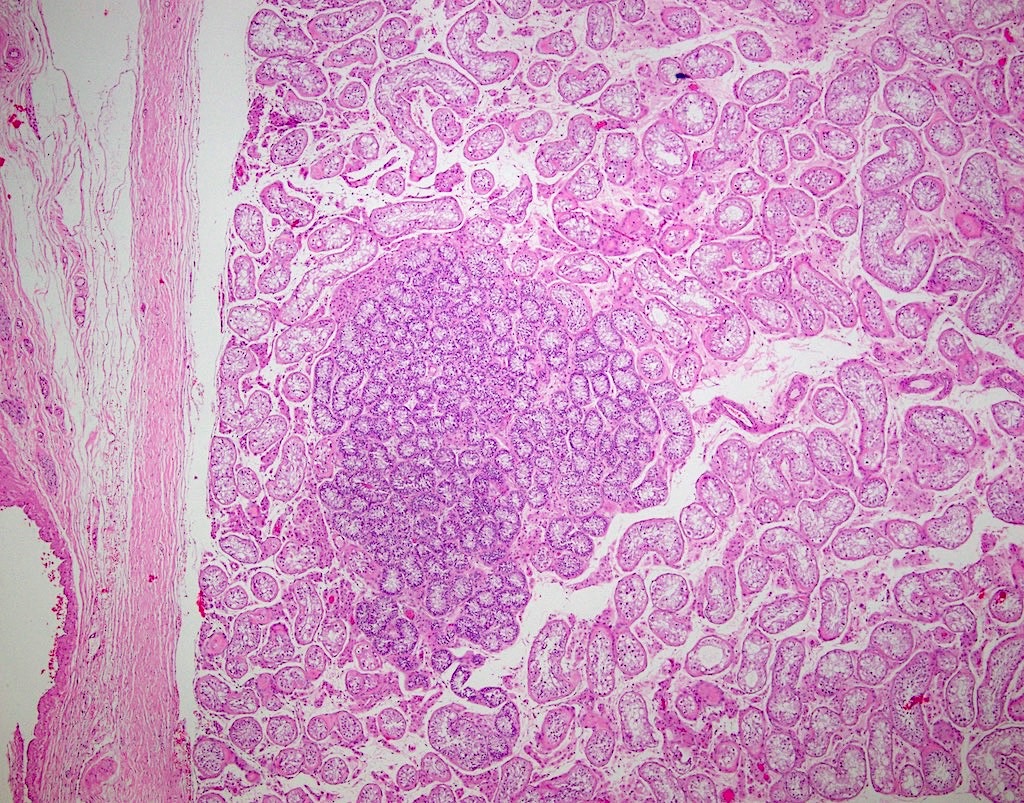
Unencapsulated nodule
Seminiferous tubule proliferation
Focal Leydig cells
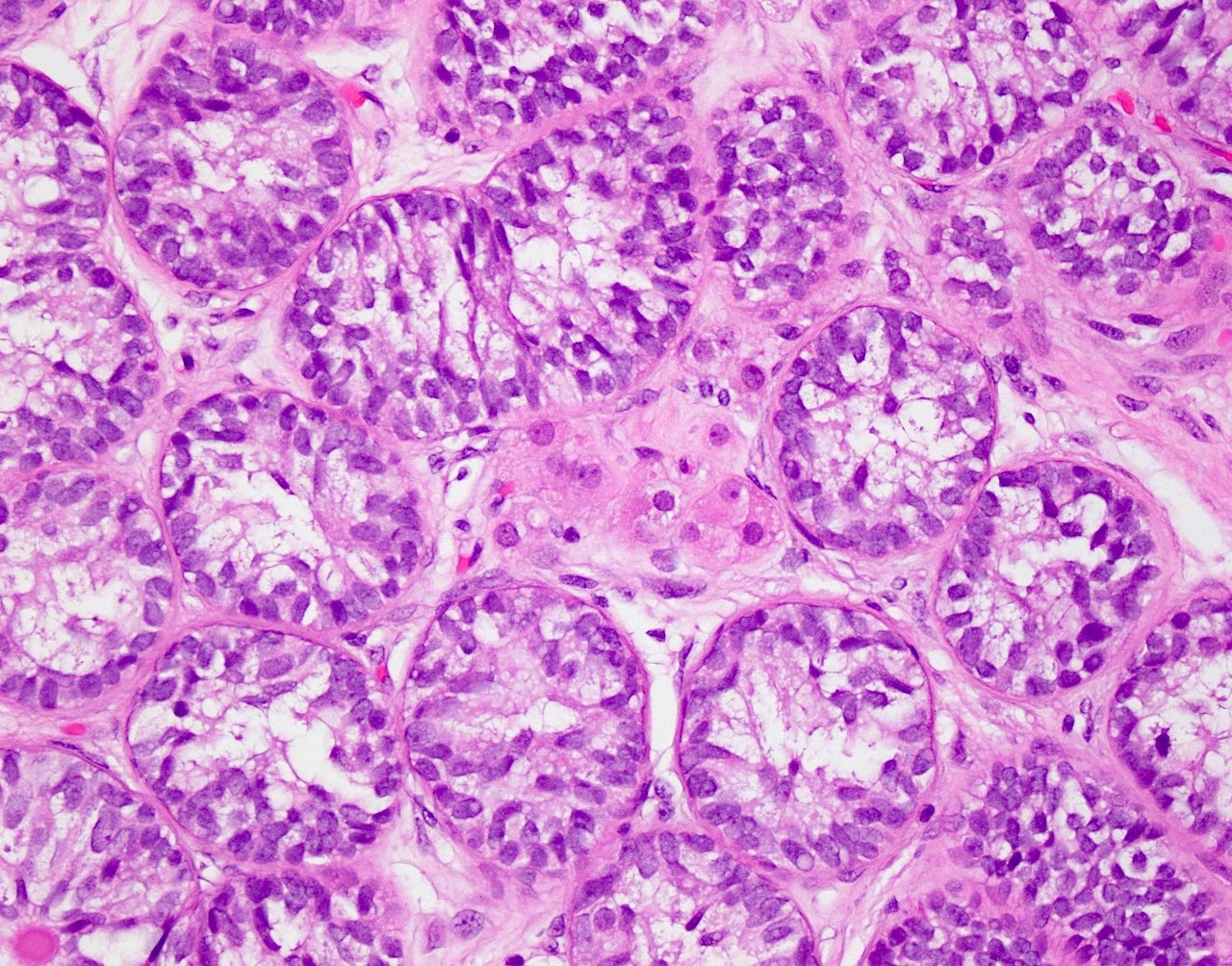
Hyaline basement membrane deposits
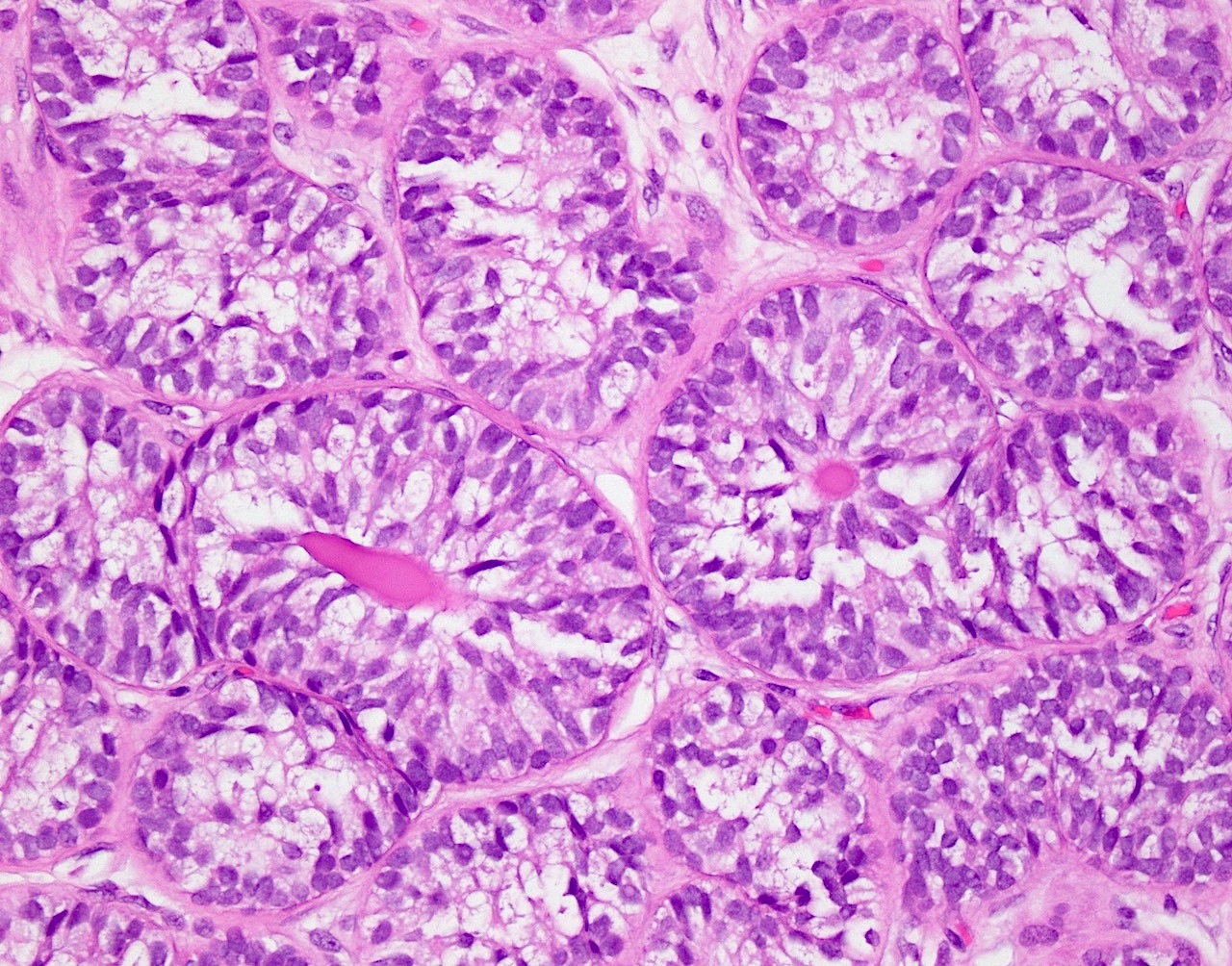
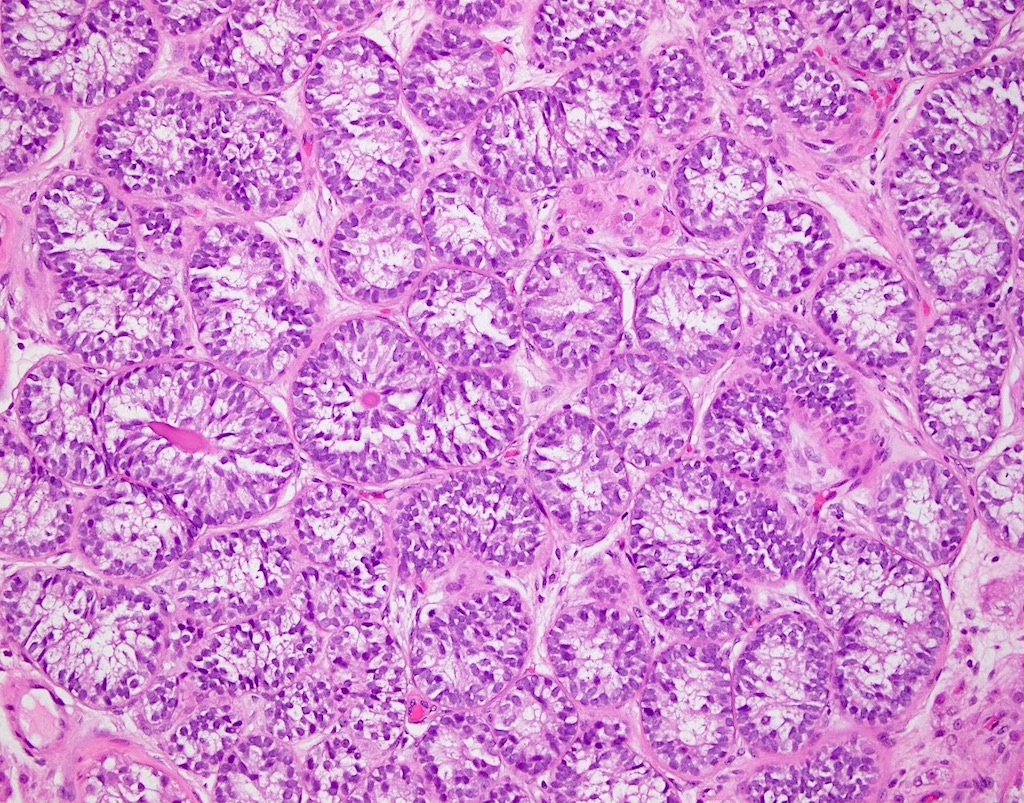
Pseudostratified Sertoli cells
Arrangement of Sertoli cells
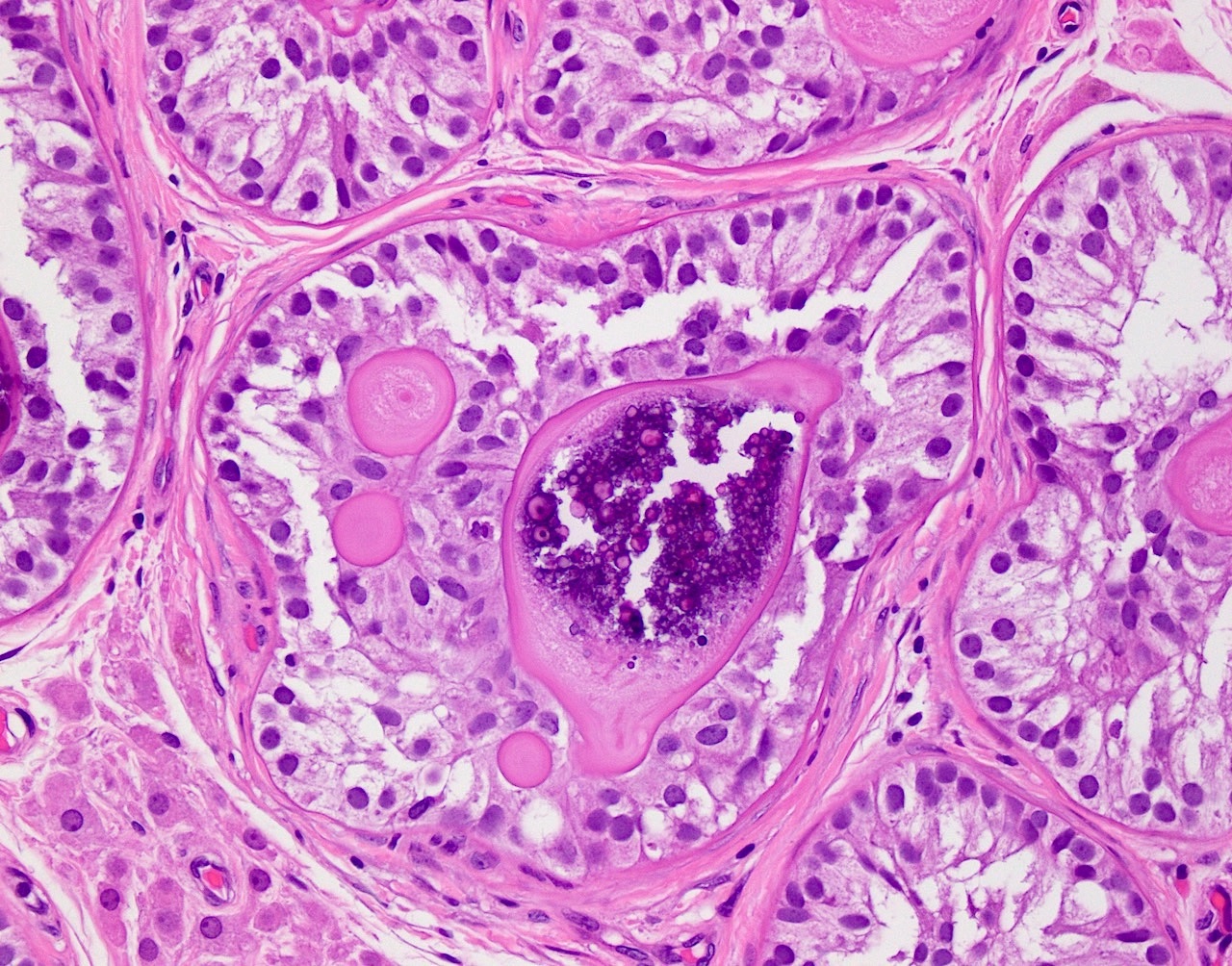
Calcification

Hyperplastic Sertoli cells
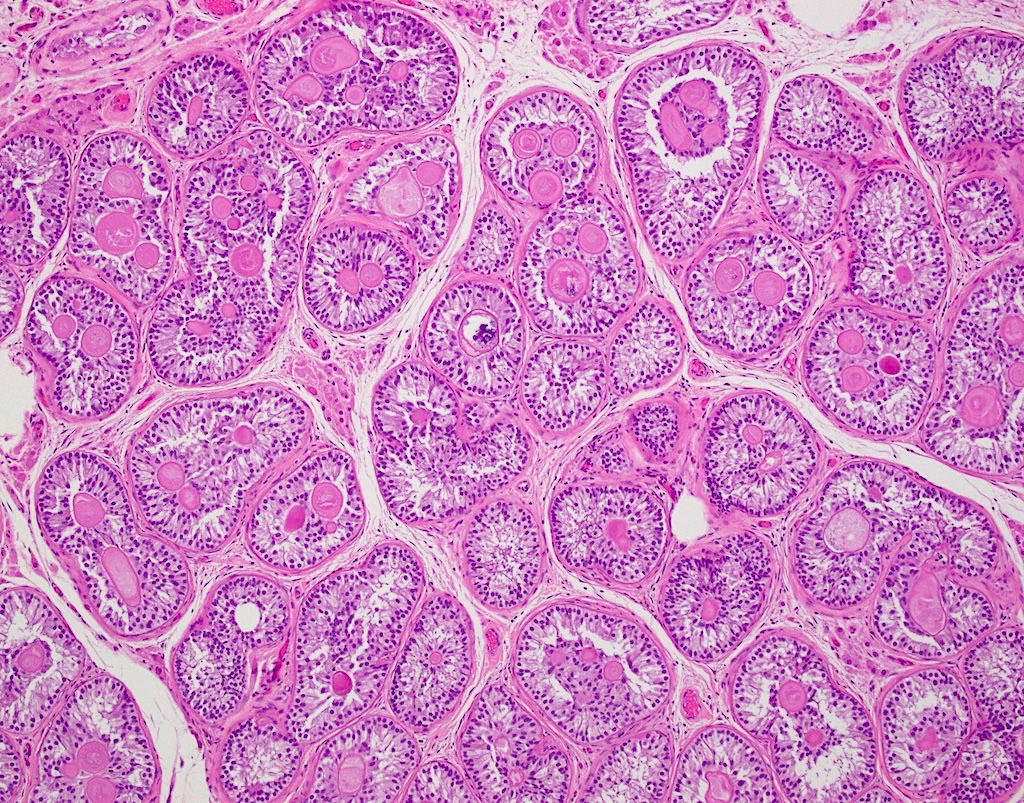
Atrophic seminiferous tubules

Persistent immature tubules
Hyalinization of basement membrane
Atrophic seminiferous tubules
Positive stains
- Immature Sertoli cells
- Occasional spermatogonia seen in some cases can be highlighted by
- NY-ESO-1 (J Clin Pathol 2006;59:1223)
- TSPY (Am J Surg Pathol 2010;34:1874)
- Basement membrane material
Negative stains
Electron microscopy description
- Hyaline material in light microscopy shows as compact multilamellar matrix in electron microscopy (J Clin Pathol 2004;57:802)
Electron microscopy images
Images hosted on other servers:

Thickened, multilamellar basement membranes

Hyaline core
Sample pathology report
- Testes, radical orchiectomy:
- Sertoli cell nodule (see comment)
- Comment: Minute nodular collection of seminiferous tubules comprised predominantly of Sertoli cells with intratubular eosinophilic basement membrane-like material, with background of benign testicular parenchyma.
Differential diagnosis
- Sertoli cell adenoma and tubular hamartoma:
- Usually larger in size
- Almost exclusively seen in patients with androgen insensitivity syndrome (AIS)
- Unencapsulated nodules composed of solid tubules of immature Sertoli cells
- Sertoli cells show spherical nuclei and lack pseudostratification
- Tubular hamartoma has a densely cellular interstitium with fusiform cells and numerous Leydig cells
- Sertoli cell adenoma lacks interstitial Leydig cells
- Absence of intratubular globular basement membrane deposits
- Sertoli cell tumor, not otherwise specified:
- Usually larger in size (> 1 cm)
- Larger cells with vesicular nuclei and prominent nucleoli arranged in cords and tubules
- Nuclear atypia and mitotic activity may be present
- Absence of basal membrane thickening and germ cells
- Intratubular large cell hyalinizing Sertoli cell neoplasia:
- Multiple nodules composed of tubules with larger diameter
- May show thickening of basal membranes and intratubular globular basement membrane deposits
- Sertoli cells with higher grade of maturation (vesicular nuclei with central nucleoli and large eosinophilic cytoplasm)
- Absence of germ cells
- Associated with Peutz-Jeghers syndrome
- Gonadoblastoma:
- Nests consist of Sertoli cells and large, atypical germ cells
- Diffuse nodular distribution
- Germ cells positive for OCT 3/4
- Sex cord stromal tumor of testis with entrapped germ cells:
- Usually larger in size
- Tubular and cord-like arrangements of sex cord cells
- Germ cells are mostly present at the periphery and in clusters
- Absence of prominent basement membrane deposits
- Testes with focal Sertoli only cell tubules:
- Contain a mix of Sertoli only tubules and tubules with germ cells
- Sertoli only tubules are not clustered
- Size of tubules and degree of Sertoli cell maturations is higher
- Absent intratubular globular basement membrane deposits
- References: MacLennan: Urologic Surgical Pathology, 4th Edition, 2019, Am J Surg Pathol 2010;34:1874
Board review style question #1
A 30 year old man presents for evaluation of a nonpainful right testicular firmness. Ultrasound imaging showed a hyperechogenic lesion and orchiectomy was performed to rule out testicular neoplasm. Gross examination reveals a well circumscribed, white-tan, firm nodule measuring 8 mm in its greatest dimension with microscopic appearance as shown in the images above. What additional intervention is necessary after diagnosis?
- Chemotherapy
- Contralateral orchiectomy
- No additional intervention is necessary
- Retroperitoneal lymph node dissection
Board review style answer #1
C. No additional intervention is necessary. The image reflects a Sertoli cell nodule, referred by some studies as macroscopic, being identified grossly with a size of 8 mm. Answers A, B and D are incorrect because Sertoli cell nodule is a nonneoplastic proliferation of immature Sertoli cells with no reported malignant potential; hence, no other intervention is required after histologic diagnosis.
Comment Here
Reference: Sertoli cell nodule
Comment Here
Reference: Sertoli cell nodule
Board review style question #2
A 25 year old man presents for evaluation of left lower abdominal pain. Imaging reveals the location of the left testicle in the inguinal canal. Subsequent orchiectomy revealed an unremarkable cut surface. Microscopic findings showed multiple, well circumscribed nodules with the appearance as shown in the images above. Which of the following immunohistochemical stains is expected to be positive?
- hCG
- Inhibin
- OCT 3/4
- PLAP
Board review style answer #2
B. Inhibin. Sertoli cell nodule is composed mainly of immature Sertoli cells and inhibin helps to highlight and confirm their presence. Answers C, D and A are incorrect because OCT 3/4, PLAP and hCG are negative in Sertoli cell nodule and are helpful to rule out the presence of germ cell neoplasms.
Comment Here
Reference: Sertoli cell nodule
Comment Here
Reference: Sertoli cell nodule
Board review style question #3
Which of the following is a common finding in Sertoli cell nodules?
- Atypical mitoses
- Globular hyaline material deposits
- Nuclei in a syncytium
- Numerous spermatogonia
Board review style answer #3
B. Globular hyaline material deposits. Sertoli cells produce an excess of basal lamina that invaginates into the involved tubules. Answer D is incorrect because spermatogonia, when present, are scattered. Answer A is incorrect because typical mitoses are not a common finding of Sertoli cell nodules and are more common in malignant entities. Answer C is incorrect because nuclei in a syncytium (syncytiotrophoblasts) are usually seen in germ cell tumors and are not an expected finding in Sertoli cell nodules.
Comment Here
Reference: Sertoli cell nodule
Comment Here
Reference: Sertoli cell nodule
