
Stomach
Other tumors
Plexiform fibromyxoma
Authors: Yujun Gan, M.D., Ph.D., Xiuli Liu, M.D., Ph.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.


Last author update: 16 June 2020
Last staff update: 26 May 2021
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: gastric plexiform fibromyxoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gan Y, Liu X. Plexiform fibromyxoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stomachplexiformfibromyxoma.html. Accessed April 19th, 2024.
Definition / general
- Benign mesenchymal gastric tumor recognized by WHO (WHO Classification of Tumours Editorial Board: Digestive System Tumours, 5th edition, 2019)
- Most are multinodular masses involving the muscularis propria or submucosa of the antral / prepyloric region (J Surg Res 2019;239:76)
Essential features
- Benign mesenchymal neoplasm that predominantly arises in the gastric antrum and pyloric region
- Multinodular and plexiform architecture with arborizing vasculature at low power
- Cytologically bland spindle cells in myxoid or fibromyxoid stroma
- Rare or no mitotic figures; low proliferation index in most cases
- Metastases and recurrence following complete excision have not been described
Terminology
- Also known as plexiform angiomyxoid myofibroblastic tumor
Epidemiology
- Males and females are equally affected
- Seen over a broad age range, including children (Am J Surg Pathol 2009;33:1624)
Sites
- Mainly reported in the stomach, with rare cases in the duodenum or jejunum reported (BMJ Case Rep 2015;201, World J Clin Cases 2018;6:1067)
Pathophysiology
- Recurrent MALAT1-GLI1 translocation or GLI1 upregulation have been identified in a subset of plexiform fibromyxomas (J Pathol 2016;239:335)
Clinical features
- Symptoms include upper gastrointestinal bleeding, abdominal distension, abdominal pain, nausea, hematemesis, anemia, weight loss, obstruction
- Some cases are incidental endoscopic finding in asymptomatic patients
Case reports
- 5 year old boy with 8.5 cm left upper abdomen mass (Pediatr Blood Cancer 2019;66:e27638)
- 34 year old man with a pyloric submucosal lesion (World J Gastroenterol 2017;23:5817)
- 44 year old woman with 5.0 cm gastric antral mass (Ann Diagn Pathol 2020;44:151453)
- 44 year old woman with gastric antral polyp (Gastroenterol Rep (Oxf) 2018;6:313)
- 71 year old woman with 4.5 cm gastric antral mass (Int J Clin Exp Pathol 2015;8:13613)
- 79 year old woman with a small gastric antral polyp (Case #316)
Treatment
- Surgical resection or endoscopic resection (Int J Clin Exp Pathol 2017;10:10926)
Clinical images
Contributed by Yujun Gan, M.D., Ph.D. and Xiuli Liu, M.D., Ph.D.
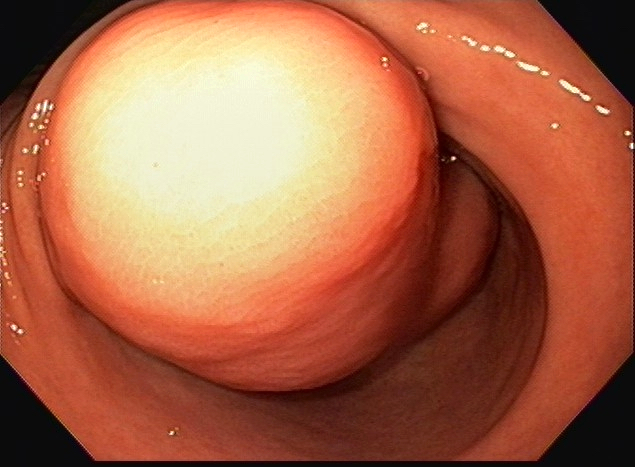
Large gastric antral mass

Large mural hypoechoic mass

FNA of the mass
Gross description
- Presents most commonly as a solitary, circumscribed, multilobulated mass centered in the muscularis propria
- Overlying mucosa may be smooth and unremarkable but sometimes is ulcerated
- Tumor size varies from 1.5 cm up to 15 cm (Am J Surg Pathol 2009;33:1624)
Gross images
Contributed by Yujun Gan, M.D., Ph.D. and Xiuli Liu, M.D., Ph.D.
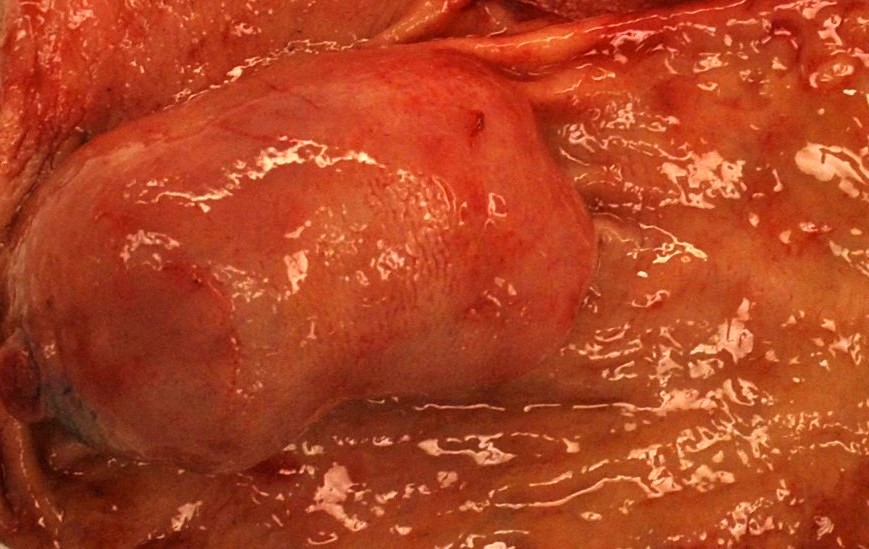
Antral mass
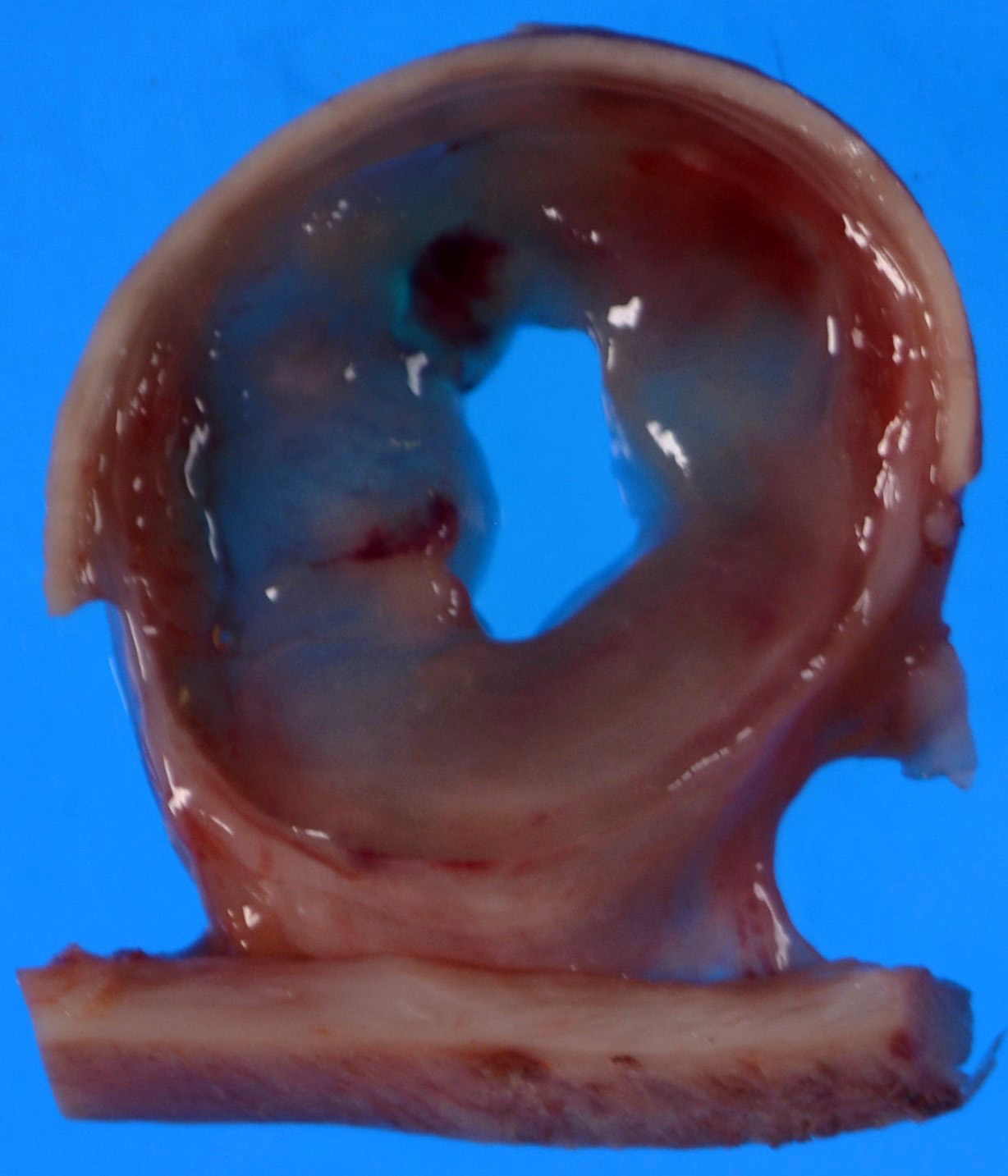
Myxoid and cystic degeneration
Microscopic (histologic) description
- Multinodular proliferation of bland spindle cells and arborizing capillaries in a myxoid stroma (World J Gastroenterol 2010;16:2835)
- Variable cellularity
- Rare or no mitoses
- Some degree of atypia and slightly increased mitotic activity rarely seen (J Surg Res 2019;239:76)
Microscopic (histologic) images
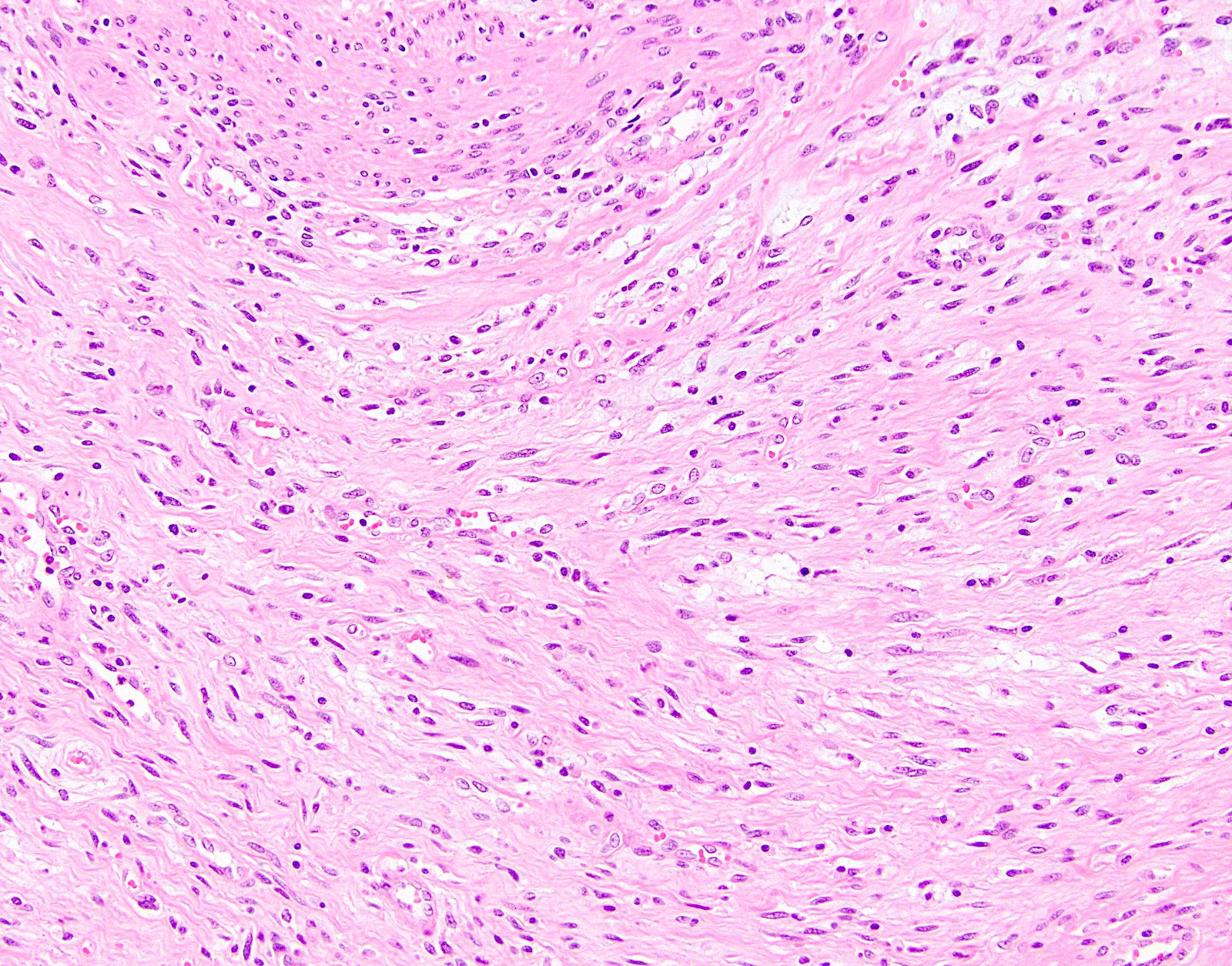
Contributed by Yujun Gan, M.D., Ph.D. and Xiuli Liu, M.D., Ph.D.
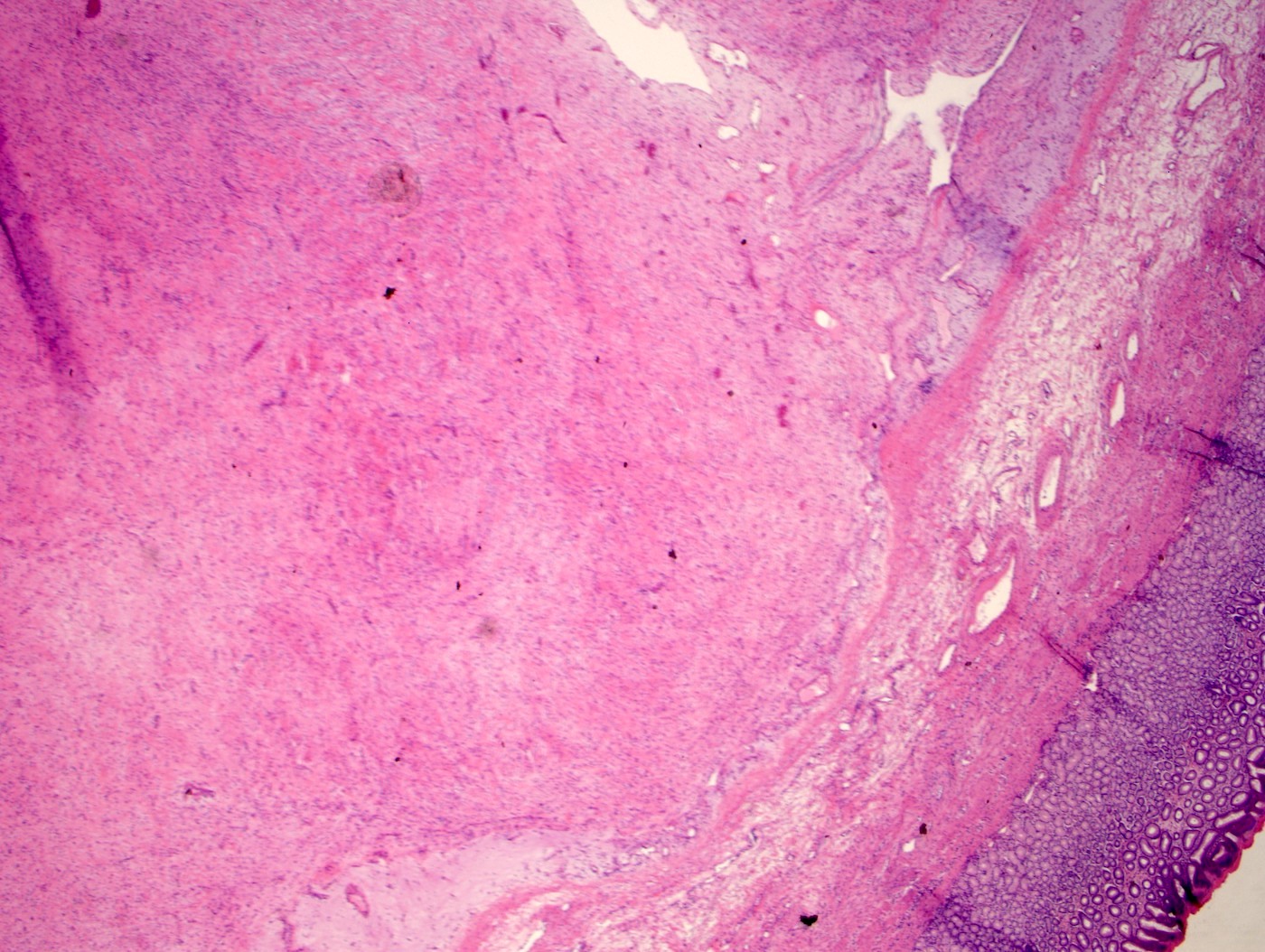
Hypocellular and myxoid tumor

Bland spindle cell proliferation
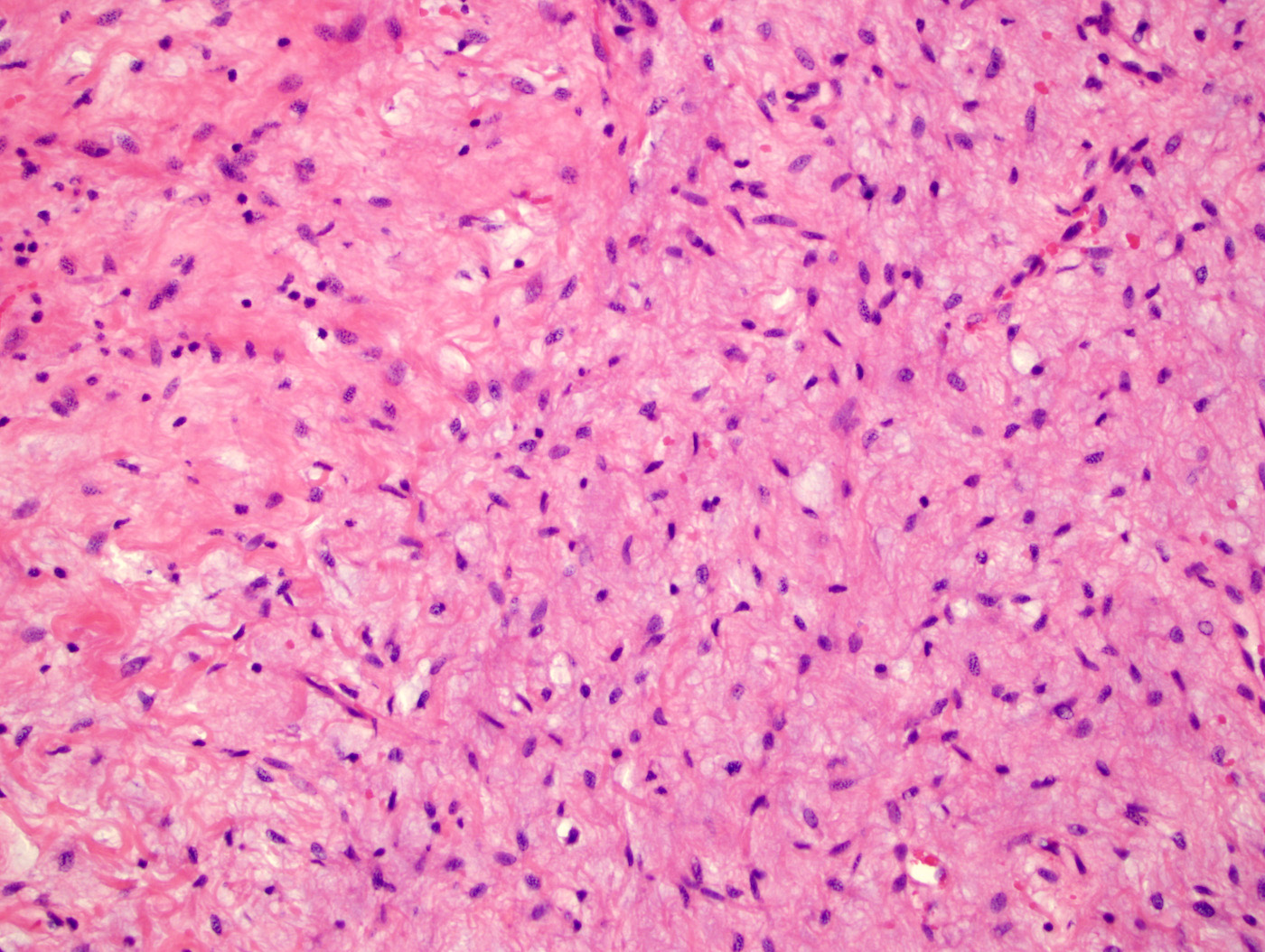
Fibrillary stroma

Spindle and myxoid tumor
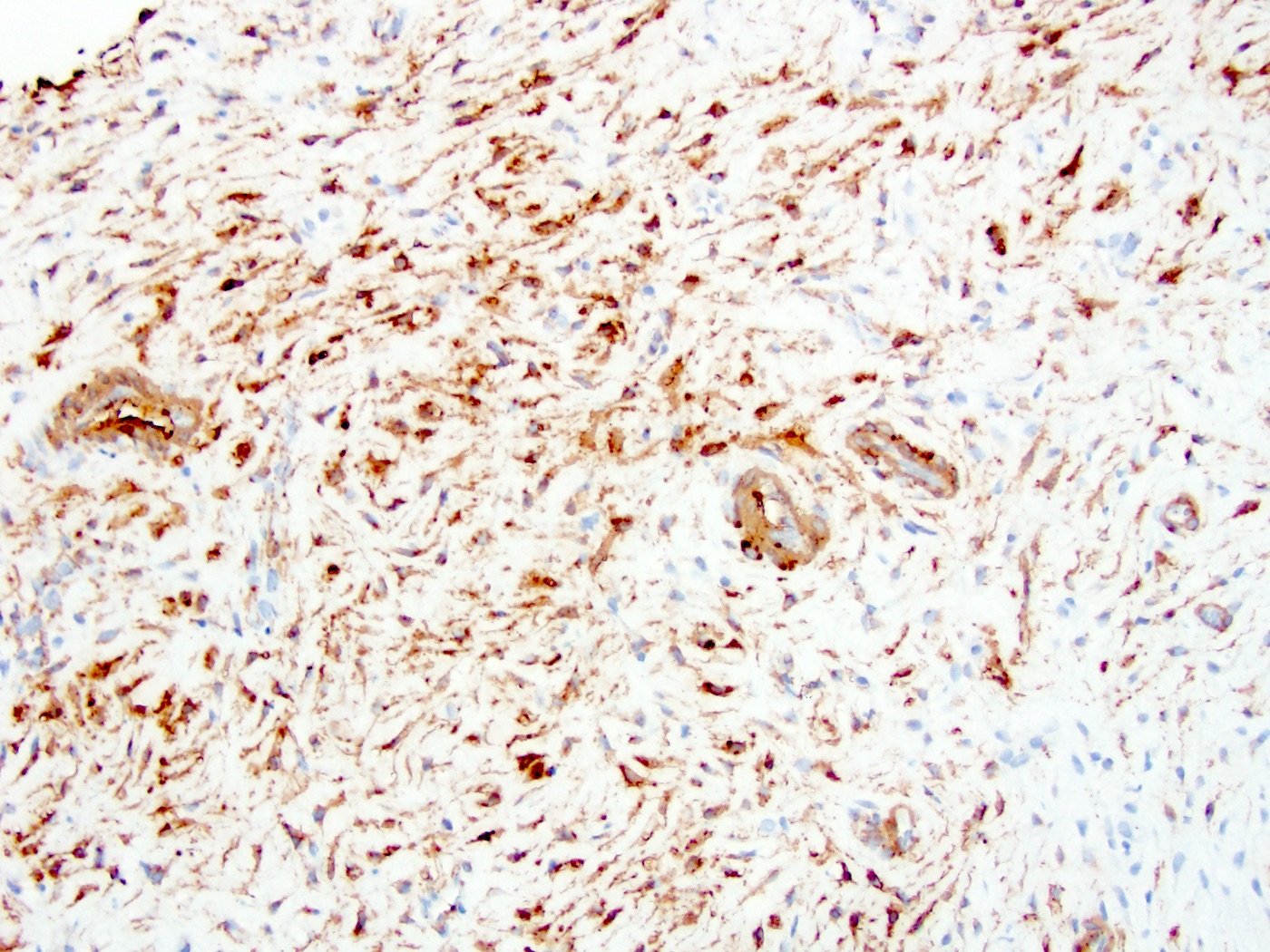
Smooth muscle actin immunoreactivity
Contributed by Raul S. Gonzalez, M.D.
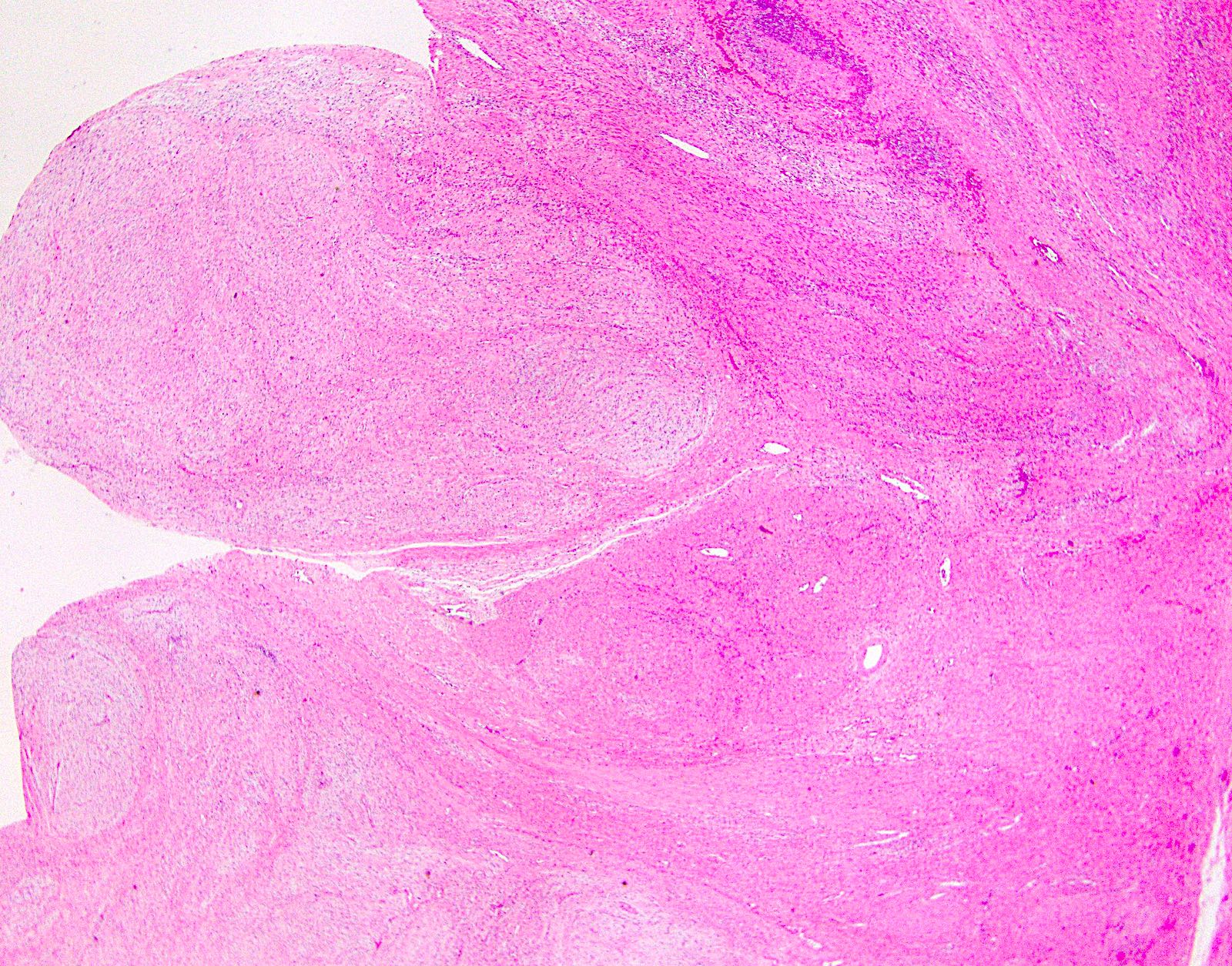
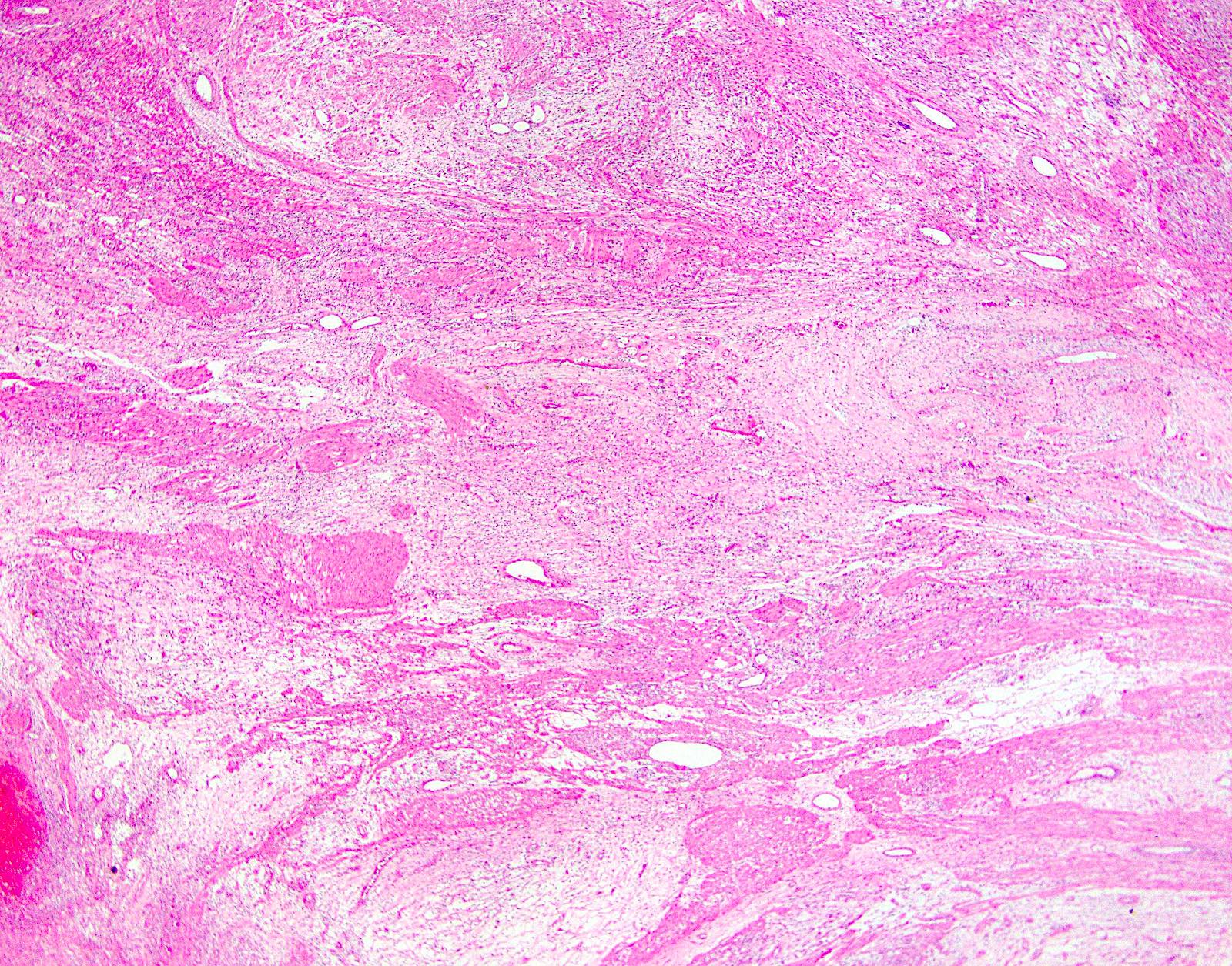
Plexiform architecture
Bland myxoid tumor
Positive stains
- Diffuse positivity for smooth muscle actin and focal positivity for CD10 and caldesmon (Am J Surg Pathol 2007;31:724, Am J Surg Pathol 2009;33:1624, Int J Clin Exp Pathol 2017;10:10926)
Negative stains
Sample pathology report
- Stomach, antrum, endoscopic submucosal dissection:
- Plexiform fibromyoxoma, completely excised (see comment)
- Comment: There is a bland spindle cell proliferation within myxoid stroma. Prominent vasculature transverses the lesion. No significant pleomorphism is noted. No mitotic figures or necrosis are noted. The tumor cells are positive for smooth muscle actin but negative for CD34, c-kit / CD117, desmin, S100 and DOG1. The overall histology and immunophenotype are most consistent with plexiform fibromyxoma. Metastases and recurrence following complete excision of plexiform fibromyxoma have not been reported.
Differential diagnosis
- GIST:
- Usually not multinodular or myxoid
- Almost all GISTs are positive for c-kit / CD117, DOG1 and CD34
- Inflammatory fibroid polyp:
- Primarily arises in the submucosa
- Has more inflammation and often demonstrates a concentric growth of spindle cells around small blood vessels
- In most cases, the spindle cells are CD34 positive
- Neurofibroma:
- Schwannoma:
- Inflammatory myofibroblastic tumor (IMT):
- Often affects children or young adults
- Most common locations are mesentery and omentum
- IMT comprises spindled to stellate myofibroblastic cells with a lymphoplasmacytic background
- About 50% of cases harbor rearrangements of anaplastic lymphoma kinase (ALK) gene and thus are positive for ALK by immunohistochemistry
- Fibromatosis:
- Primarily occurs in the mesentery in patients with familial adenomatous polyposis (FAP)
- Often demonstrates an infiltrative growth pattern with sweeping fascicles of myofibroblasts with evenly spaced nuclei separated by collagen
- Tumor cells are variably positive for smooth muscle actin (SMA) but negative for CD34, S100, CD117 and DOG1
- Tumor cells demonstrate beta catenin nuclear reactivity and LEF-1 nuclear reactivity (Appl Immunohistochem Mol Morphol 2018;26:648)
Board review style question #1
Which of the following is true about plexiform fibromyxoma?
- Complete resection of the lesion provides cure
- Metastases are common after complete resection
- Most plexiform fibromyxomas are malignant
- Plexiform fibromyxoma only occurs in the stomach
- Recurrent translocation of genes have not been reported
Board review style answer #1
Board review style question #2
A 71 year old woman presented with vague upper abdominal pain. EGD examination reveals a 4.5 cm mural mass in the antrum. The patient underwent partial gastrectomy. Gross examination reveals a multilobular mural mass. The tumor shows a bland spindle cell proliferation in a variably myxoid stroma. The tumor cells are positive for smooth muscle actin but negative for CD34, CD117, desmin, ALK, S100 or DOG1. Which of the following is most likely the correct diagnosis?
- Gastrointestinal stromal tumor
- Inflammatory fibroid polyp
- Neurofibroma
- Plexiform fibromyxoma
- Schwannoma
Board review style answer #2
